
Abstract
Introduction
Hypogonadism is the most common form of hypopituitarism in men with macroprolactinoma. However, evidence on factors related to hypogonadism recovery is limited.
Objectives
We estimated the proportion of hypogonadism in men with macroprolactinoma exclusively treated with dopamine agonists, and we assessed the factors predicting hypogonadism recovery.
Patients and methods:
This was a multicenter retrospective study of men with macroprolactinoma identified using ICD 9 and 10 codes and treated between 2009 and 2019 in five centers in the United Arab Emirates and Saudi Arabia. We evaluated hypogonadism, defined as low total testosterone (TT) level with normal or low gonadotropins on presentation and during the last clinic visit.
Results
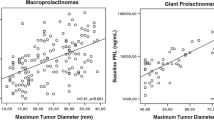
A total of 79 patients (median age 32 years) were included in the study. The most common symptoms at presentation were headache (73.7%), erectile dysfunction (55.4%), and low libido (54.3%). The median tumor size was 2.9 cm (1.0–9.7) at diagnosis. Sixty-three patients (79.7%) had hypogonadism at baseline. Growth hormone deficiency (GHD) and hypothyroidism were present in 34.4% and 32.9% of patients, respectively. The median serum prolactin (PRL) level was 20,175 (min-max 2254 − 500,000) mIU/l with a median serum TT of 4.5 (min-max 0.4–28.2) nmol/l. Most patients were treated with cabergoline (n = 77, 97.5%) with a median of 6 (min-max 0.6–22) years. At follow-up, 65% of patients recovered their pituitary-testicular axis. Patients with recovered hypogonadism had smaller median tumor size (2.4 [1-5.4] vs. 4.3 [1.6–9.7], p = 0.003), lower PRL level (18, 277 [2254 − 274, 250] vs. 63,703 [ 3,365–500,000], p = 0.008 ), higher TT level (4.6 [0.6–9.2] vs. 2.3 [0.5–7.3], p = 0.008), lower PRL normalization time on medical therapy (8 months (0.7–72) vs. 24 (3-120), p = 0.009) as well as lower frequency of GHD (17.1% vs. 60%, p = 0.006) and secondary hypothyroidism (17.9% vs. 57.1%, p = 0.003) compared with those with persistent hypogonadism respectively. Age at diagnosis, presenting symptoms and duration of medical therapy did not predict hypogonadism recovery.
Conclusions
About two-thirds of men with macroprolactinoma recover from hypogonadism, mostly with 24 months of therapy. Smaller adenoma size, lower prolactin level, earlier prolactin normalization, and higher testosterone patients were related to testosterone normalization.



Similar content being viewed by others


References
Fernandez A, Karavitaki N, Wass JA (2010) Prevalence of pituitary adenomas: a community-based, cross-sectional study in Banbury (Oxfordshire, UK). Clin Endocrinol 72:377–382
Al-Dahmani K, Mohammad S, Imran F, Theriault C, Doucette S, Zwicker D et al (2016) Sellar Masses: An Epidemiological Study. Can J Neurol Sci 43(2):291–297
Delgrange E, Trouillas J, Master D, Donckier J, Tourniaire J (1997) Jul;82(7):2102-7 Sex-related difference in the growth of prolactinomas: a clinical and proliferation marker study. J Clin Endocrinol Metab. DOI: https://doi.org/10.1210/jcem.82.7.4088. PMID: 9215279
Colao A, Vitale G, Cappabianca P, Briganti F, Ciccarelli A, De Rosa M, Zarrili S, Lombardi G (2004) Outcome of cabergoline treatment in men with prolactinoma: effects of a 24-month treatment on prolactin levels, tumor mass, recovery of pituitary function, and semen analysis. J Clin Endocrinol Metab 89:1704–1711
Sibal L, Ugwu P, Kendall-Taylor P, Ball SG, James RA, Pearce SH, Hall K, Quinton R (2002) Medical therapy of macroprolactinomas in males: I. Prevalence of hypopituitarism at diagnosis. II. The proportion of cases exhibiting recovery of pituitary function.Pituitary5243–246
Karavitaki N, Dobrescu R, Byrne JV, Grossman AB, Wass JAH (2013) Does hypopituitarism recover when macroprolactinomas are treated with cabergoline? Clin Endocrinol 79:217–223
Barber TM, Kyrou I, Kaltsas G, Grossman AB, Randeva HS, Weickert MO Mechanisms of Central Hypogonadism. Int J Mol Sci. 2021 Jul 30;22(15):8217. DOI: https://doi.org/10.3390/ijms22158217. PMID: 34360982; PMCID: PMC8348115
Melmed S, Casanueva FF, Hoffman AR, Kleinberg DL, Montori VM, Schlechte JA, Wass JA, Endocrine Society (2011) Feb;96(2):273 – 88 ;. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. DOI: https://doi.org/10.1210/jc.2010-1692. PMID: 21296991
Pinzone JJ, Katznelson L, Danila DC, Pauler DK, Miller CS, Klibanski A (2000) Primary medical therapy of micro-and macroprolactinomas in men. J Clin Endocrinol Metab 85:3053–3057
Prior JC, Cox TA, Fairholm D, Kostashuk E, Nugent R (1987) Testosterone-related exacerbation of a prolactin-producing macro- adenoma: possible role for estrogen. J Clin Endocrinol Metab 64:391–394
Jayasena CN, Anderson RA, Llahana S, Barth JH, MacKenzie F, Wilkes S, Smith N, Sooriakumaran P, Minhas S, Wu FCW, Tomlinson J, Quinton R (2022 Feb) Society for Endocrinology guidelines for testosterone replacement therapy in male hypogonadism. Clin Endocrinol (Oxf) 96(2):200–219
Fleseriu M, Hashim IA, Karavitaki N, Melmed S, Murad MH, Salvatori R, Samuels MH (2016 Nov) Hormonal Replacement in Hypopituitarism in Adults: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 101(11):3888–3921. DOI: https://doi.org/10.1210/jc.2016-2118. Epub 2016 Oct 13. PMID: 27736313
Sehembly M, Lila AR, Sarathi V, Shah R, Sankhe S, Jaiswal SK, Ramteke-Jadhav S, Patil V, Shah N, Bandgar T Predictors of Chronic LH-Testosterone Axis Suppression in Male Macroprolactinomas With Normoprolactinemia on Cabergoline. J Clin Endocrinol Metab. 2020 Dec 1;105(12):dgaa650. DOI: https://doi.org/10.1210/clinem/dgaa650. PMID: 32942295
Tirosh, Benbassat C, Lifshitz A, Shimon I (2015) Hypopituitarism patterns and prevalence among men with macroprolactinomas. Pituitary 18:108–115
Almistehi WM, Vaninetti N, Mustafa S, Hebb ALO, Zwicker D, Doucette S, Alqahtani S, Clarke DB, Imran SA (2020) Dec;23(6):622–629 Secondary pituitary hormonal dysfunction patterns: tumor size and subtype matter. Pituitary. DOI: https://doi.org/10.1007/s11102-020-01067-7. PMID: 32715387
Smith TP, Suliman AM, Fahie-Wilson MN, McKenna TJ (2002) Dec;87(12):5410-5 Gross variability in the detection of prolactin in sera containing big big prolactin (macroprolactin) by commercial immunoassays. J Clin Endocrinol Metab. DOI: https://doi.org/10.1210/jc.2001-011943. PMID: 12466327
Funding
None.
Author information
Authors and Affiliations
Contributions
All the named authors fulfilled the ICMJE criteria of authorship. They all reviewed the manuscript for intellectual content and approved its final version.
Corresponding author
Ethics declarations
Conflict of interest
None of the authors declared any conflict of interest.
Compliance with ethical principles
Research ethics committees of all participating centers approved the study. Cases were identified using ICD 9 and 10 codes (253.2, D35.2, respectively. The condition of consent was waived due to the study’s retrospective nature.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Al Dahmani, K.M., Almalki, M.H., Ekhzaimy, A. et al. Proportion and predictors of Hypogonadism Recovery in Men with Macroprolactinomas treated with dopamine agonists. Pituitary 25, 658–666 (2022). https://doi.org/10.1007/s11102-022-01242-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-022-01242-y