
Abstract
Purpose
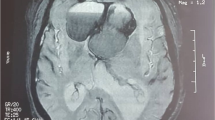
We aimed to assess clinical characteristics of apoplexy of pituitary microadenomas compared to macroadenomas.
Methods
We retrieved clinical records of patients > 18 years old, hospitalized in Rambam hospital between January 2001 and October 2017, with pituitary apoplexy and follow-up of at least one year. We compared clinical course and outcomes of apoplexy between patients with microadenomas and macroadenomas, and between patients who received conservative or surgical treatment. Statistical analysis was done using Fisher’s exact and Mann–Whitney tests.
Results
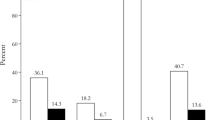
Twenty-seven patients with pituitary apoplexy were included in the final analysis: mean age was 40.7 ± 12.5 years, 13(48%) were female, 7(26%) had microadenomas, and 21(78%) harbored clinically nonfunctioning pituitary adenomas. Upon admission, hyponatremia, random cortisol level of < 200 nmol/L, and secondary hypothyroidism, were evident in 6/20, 8/18, and 4/18 patients with macroadenoma and 1/5, 2/5, and 1/6 patients with microadenoma, respectively (P = 1.0). Hypogonadotropic hypogonadism was evident in 9/12 men with macroadenoma. In 12 macroadenoma patients, the tumor abutted the optic chiasm, of whom eight had visual field defects. Fifteen patients with macroadenoma and two with microadenoma underwent transsphenoidal surgery. Median follow-up was 3 years. At last follow-up visit, patients with microadenoma had lower rates of corticotropic deficiency or secondary hypothyroidism compared to macroadenoma patients (1/7 vs. 13/20 respectively, p = 0.033). Only two patients with macroadenomas had persistent visual field defects. Outcomes were comparable between conservative and surgical treatment groups.
Conclusions
Long term pituitary hormone deficiencies are more common in pituitary apoplexy patients with macroadenomas. Apoplexy of pituitary microadenoma carries a more favorable prognosis.
Similar content being viewed by others

References
Briet C, Salenave S, Bonneville JF, Laws ER, Chanson P (2015) Pituitary apoplexy. Endocrine Reviews 36:622–645
Semple PL, Webb MK, De Villiers JC, Laws ER (2005) Pituitary apoplexy Neurosurgery 56:65–72 discussion 72 – 3
Randall BR, Couldwell WT (2010) Apoplexy in pituitary microadenomas. Acta Neurochir (Wien) 52:1737–1740
Pignatta AB, Díaz AG, Gómez RM, Bruno OD (2004) Spontaneous remission of Cushing’s disease after disappearance of a microadenoma attached to the pituitary stalk. Pituitary 7:45–49
Bass D, Bartels C, Eshraghi S, Ioachimescu A, Oyesiku N, Pradilla G (2016) The Presentation and Clinical Management of Pituitary Microadenoma Apoplexy. J Neurol Surg Part B Skull Base 77:A070
Möller-Goede DL, Brändle M, Landau K, Bernays RL, Schmid C (2011) Pituitary apoplexy: Re-evaluation of risk factors for bleeding into pituitary adenomas and impact on outcome. Eur J Endocrinol 164:37–43
Sibal L, Ball SG, Connolly V, James RA, Kane P, Kelly WF, Kendall-Taylor P, Mathias D, Perros P, Quinton R, Vaidya B (2004) Pituitary apoplexy: a review of clinical presentation, management and outcome in 45 cases. Pituitary 7:157–163
Gruber A, Clayton J, Kumar S, Robertson I, Howlett T, Mansell P (2006) Pituitary apoplexy: Retrospective review of 30 patients - Is surgical intervention always necessary? Br J Neurosurg 20:379–385
Ayuk J, McGregor EJ, Mitchell RD, Gittoes NJL (2004) Acute management of pituitary apoplexy - Surgery or conservative management? Clin Endocrinol (Oxf) 61:747–752
Tu M, Lu Q, Zhu P, Zheng W (2016) Surgical versus non-surgical treatment for pituitary apoplexy: A systematic review and meta-analysis. Journal of the Neurological Sciences Elsevier BV 370:258–262
Pal A, Capatina C, Tenreiro AP, Guardiola PD, Byrne JV, Cudlip S, Karavitaki N, Wass JAH (2011) Pituitary apoplexy in non-functioning pituitary adenomas: Long term follow up is important because of significant numbers of tumour recurrences. Clin Endocrinol (Oxf) 75:501–504
Sahyouni R, Goshtasbi K, Choi E, Mahboubi H, Le R, Khahera AS, Hanna GK, Hatefi D, Hsu FP, Bhandarkar ND, Kuan EC, Cadena G (2019) Vision Outcomes in Early versus Late Surgical Intervention of Pituitary Apoplexy: Meta-Analysis. World neurosurg 127:52–57
Rutkowski MJ, Kunwar S, Blevins L, Aghi MK (2018) Surgical intervention for pituitary apoplexy: An analysis of functional outcomes. J Neurosurg 129:417–424
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Ethics approval
The study was approved by the RHCC Institutional Review Board.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nakhleh, A., Assaliya Naffa, M., Sviri, G. et al. Outcomes of pituitary apoplexy: a comparison of microadenomas and macroadenomas. Pituitary 24, 492–498 (2021). https://doi.org/10.1007/s11102-020-01124-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-020-01124-1