
Abstract
Background
Pituitary metastases are rare and commonly described in case reports or small case series. Due to its rarity this entity is not subject to standardized treatment guidelines, there is debate about typical initial symptoms that may lead to finding the correct diagnosis and information about the clinical course is also sparse.
Methods
We have conducted a retrospective analysis of patients with pituitary metastases who were surgically treated via a transsphenoidal procedure at our institution between 2006 and 2014. Underlying primary disease, clinical and surgical course as well as adjuvant radiotherapy and follow-up data are presented.
Results
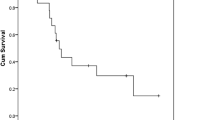
14 patients met the inclusion criteria (8 female, 6 male). Mean age was 61.5 years. Most patients became symptomatic with visual symptoms—both visual deterioration and/or diplopia (n = 13)—and anterior lobe insufficiency (n = 8). Surprisingly diabetes insipidus was only seen in three patients. All patients underwent transsphenoidal surgery initially, four patients had to undergo surgery for residual tumor or recurrence, two of them via a transcranial route. Breast cancer was the most common entity (n = 6), followed by prostate cancer (n = 3), nsclc (n = 2) and melanoma, thyroid cancer and renal cancer in one case each. Postoperative MRI showed gross total resection in four cases and residual disease in eight cases (subtotal resection, partial resection and biopsy), two patients files were incomplete regarding MRI-results. All patients underwent adjuvant radiotherapy. Survival after the initial diagnosis of cancer was 36 and 16 months after diagnosis of pituitary metastases.
Conclusion
Our results indicate that transsphenoidal surgery is a safe method to resect pituitary metastases and that the extend of resection does not have an influence on survival time. Our results also indicate that diabetes insipidus may not be the most common initial symptom of pituitary metastases and lack thereof should not lead to making a wrong diagnosis and delaying appropriate therapy.




Similar content being viewed by others


References
Saeger W, Ludecke DK, Buchfelder M, Fahlbusch R, Quabbe HJ, Petersenn S (2007) Pathohistological classification of pituitary tumors: 10 years of experience with the German Pituitary Tumor Registry. Eur J Endocrinol 156(2):203–216. doi:10.1530/eje.1.02326
Quaresma M, Coleman MP, Rachet B (2014) 40-year trends in an index of survival for all cancers combined and survival adjusted for age and sex for each cancer in England and Wales, 1971–2011: a population-based study. Lancet. doi:10.1016/S0140-6736(14)61396-9
He W, Chen F, Dalm B, Kirby PA, Greenlee JD (2014) Metastatic involvement of the pituitary gland: a systematic review with pooled individual patient data analysis. Pituitary. doi:10.1007/s11102-014-0552-2
Fassett DR, Couldwell WT (2004) Metastases to the pituitary gland. Neurosurg Focus 16(4):E8
Morita A, Meyer FB, Laws ER Jr (1998) Symptomatic pituitary metastases. J Neurosurg 89(1):69–73. doi:10.3171/jns.1998.89.1.0069
Buchfelder M, Schlaffer S (2014) Imaging of pituitary pathology. Handbook Clin Neurol 124:151–166. doi:10.1016/B978-0-444-59602-4.00011-3
Kovacs K (1973) Metastatic cancer of the pituitary gland. Oncology 27(6):533–542
Branch CL Jr, Laws ER Jr (1987) Metastatic tumors of the sella turcica masquerading as primary pituitary tumors. J Clin Endocrinol Metab 65(3):469–474. doi:10.1210/jcem-65-3-469
McCormick PC, Post KD, Kandji AD, Hays AP (1989) Metastatic carcinoma to the pituitary gland. Br J Neurosurg 3(1):71–79
Flitsch J, Bernreuther C, Hagel C, Ludecke DK (2008) Hypophysectomy for prostate cancer: A revival of old knowledge? J Neurosurg 109(4):760–764. doi:10.3171/JNS/2008/109/10/0760
Abrams HL, Spiro R, Goldstein N (1950) Metastases in carcinoma; analysis of 1000 autopsied cases. Cancer 3(1):74–85
Marin F, Kovacs KT, Scheithauer BW, Young WF Jr (1992) The pituitary gland in patients with breast carcinoma: a histologic and immunocytochemical study of 125 cases. Mayo Clin Proc 67(10):949–956
Houck WA, Olson KB, Horton J (1970) Clinical features of tumor metastasis to the pituitary. Cancer 26(3):656–659
Kimmel DW, O’Neill BP (1983) Systemic cancer presenting as diabetes insipidus. Clinical and radiographic features of 11 patients with a review of metastatic-induced diabetes insipidus. Cancer 52(12):2355–2358
Oi S, Ciric I, Mayer TK (1978) Metastatic breast carcinoma in the pituitary gland. Brain Nerve 30(1):69–73
Komninos J, Vlassopoulou V, Protopapa D, Korfias S, Kontogeorgos G, Sakas DE, Thalassinos NC (2004) Tumors metastatic to the pituitary gland: case report and literature review. J Clin Endocrinol Metab 89(2):574–580. doi:10.1210/jc.2003-030395
Sioutos P, Yen V, Arbit E (1996) Pituitary gland metastases. Ann Surg Oncol 3(1):94–99
Santen RJ, Worgul TJ, Samojlik E, Interrante A, Boucher AE, Lipton A, Harvey HA, White DS, Smart E, Cox C, Wells SA (1981) A randomized trial comparing surgical adrenalectomy with aminoglutethimide plus hydrocortisone in women with advanced breast cancer. N Engl J Med 305(10):545–551. doi:10.1056/NEJM198109033051003
Studer UE, Whelan P, Albrecht W, Casselman J, de Reijke T, Hauri D, Loidl W, Isorna S, Sundaram SK, Debois M, Collette L (2006) Immediate or deferred androgen deprivation for patients with prostate cancer not suitable for local treatment with curative intent: European Organisation for Research and Treatment of Cancer (EORTC) Trial 30891. J Clin Oncol 24(12):1868–1876. doi:10.1200/JCO.2005.04.7423
Bolla M, de Reijke TM, Van Tienhoven G, Van den Bergh AC, Oddens J, Poortmans PM, Gez E, Kil P, Akdas A, Soete G, Kariakine O, van der Steen-Banasik EM, Musat E, Pierart M, Mauer ME, Collette L, Group, E.R.O., Genito-Urinary Tract Cancer, G. (2009) Duration of androgen suppression in the treatment of prostate cancer. N Engl J Med 360(24):2516–2527. doi:10.1056/NEJMoa0810095
Early Breast Cancer Trialists’ Collaborative, G., Davies C, Godwin J, Gray R, Clarke M, Cutter D, Darby S, McGale P, Pan HC, Taylor C, Wang YC, Dowsett M, Ingle J, Peto R (2011) Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet 378(9793):771–784. doi:10.1016/S0140-6736(11)60993-8
Schiavon G, Smith IE (2014) Status of adjuvant endocrine therapy for breast cancer. Breast Cancer Res 16(2):206
Heidenreich A, Bastian PJ, Bellmunt J, Bolla M, Joniau S, van der Kwast T, Mason M, Matveev V, Wiegel T, Zattoni F, Mottet N, European Association of Urology (2014) EAU guidelines on prostate cancer. Part II: treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur Urol 65(2):467–479. doi:10.1016/j.eururo.2013.11.002
Kluth LA, Shariat SF, Kratzik C, Tagawa S, Sonpavde G, Rieken M, Scherr DS, Pummer K (2014) The hypothalamic-pituitary-gonadal axis and prostate cancer: implications for androgen deprivation therapy. World J Urol 32(3):669–676. doi:10.1007/s00345-013-1157-5
Seidenfeld J, Samson DJ, Hasselblad V, Aronson N, Albertsen PC, Bennett CL, Wilt TJ (2000) Single-therapy androgen suppression in men with advanced prostate cancer: a systematic review and meta-analysis. Ann Intern Med 132(7):566–577
Kaisary AV, Iversen P, Tyrrell CJ, Carroll K, Morris T (2001) Is there a role for antiandrogen monotherapy in patients with metastatic prostate cancer? Prostate Cancer Prostatic Dis 4(4):196–203. doi:10.1038/sj.pcan.4500531
Beer TM, Armstrong AJ, Rathkopf DE, Loriot Y, Sternberg CN, Higano CS, Iversen P, Bhattacharya S, Carles J, Chowdhury S, Davis ID, de Bono JS, Evans CP, Fizazi K, Joshua AM, Kim CS, Kimura G, Mainwaring P, Mansbach H, Miller K, Noonberg SB, Perabo F, Phung D, Saad F, Scher HI, Taplin ME, Venner PM, Tombal B, Investigators P (2014) Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med 371(5):424–433. doi:10.1056/NEJMoa1405095
Acknowledgments
The authors would like to thank Dr. Jakob Matschke at the Hamburg University, Institute of Neuropathology for his support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Financial fundings
This is an unsponsored research, the authors declare that no financial fundings were received.
Additional information
T. Burkhardt and M. Henze have contributed equally to this work.
Rights and permissions
About this article

Cite this article
Burkhardt, T., Henze, M., Kluth, L.A. et al. Surgical management of pituitary metastases. Pituitary 19, 11–18 (2016). https://doi.org/10.1007/s11102-015-0676-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-015-0676-z