
Abstract
Purpose
To compare hypothalamus–pituitary–adrenal (HPA) axis integrity at diagnosis and recovery after transsphenoidal surgery (TSS), in acromegaly patients, compared with tumor size matched non-functioning adenoma (NFA) patients.
Methods
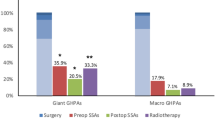
A retrospective 7-year evaluation of acromegaly patients, who underwent TSS with 52 weeks follow-up at a single institution, was undertaken. 50 acromegaly with complete follow-up data at all points and 50 NFA patients were matched for tumor size; HPA axis was similarly assessed pre-operatively and at 6, 12 and 52 weeks post-operatively. Recovery of HPA axis and gender specific prevalence of adrenal insufficiency (AI), were analyzed in both groups. We also studied AI in acromegaly patients requiring medical therapy post-operatively vs those in remission after surgery.
Results
AI remained less prevalent in acromegaly vs NFA (acromegaly, p = 0.01; NFA, p = 0.15) at 52 weeks after surgery, although the prevalence of AI decreased in both groups from baseline by 52 weeks. Additionally, recovery from baseline AI was significantly greater by 52 weeks in acromegaly patients over NFA patients (p = 0.001). Recovery of HPA axis in acromegaly patients remained significant (p = 0.03) despite the need for medical therapy. AI at baseline was proportionately more prevalent in acromegalic males at baseline (p = 0.002) but no gender difference was apparent at 52 weeks (p = 0.35). Conversely, in NFA patients, no gender difference was apparent pre-operatively (p = 0.49), but AI was more prevalent in males at 52 weeks (p = 0.001).
Conclusion
In the longest comparative study to date using a standard assessment modality, HPA axis recovery was more frequent in acromegaly compared to NFA patients, independent of tumor size, cavernous sinus invasion (CSI), and body mass index (BMI). HPA axis integrity must be carefully and periodically monitored in acromegaly patients during short- and long-term follow-up to prevent overtreatment with glucocorticoids.


Similar content being viewed by others


References
Melmed S (2009) Acromegaly pathogenesis and treatment. J Clin Investig 119(11):3189–3202
Nachtigall L, Delgado A, Swearingen B, Lee H, Zerikly R, Klibanski A (2008) Changing patterns in diagnosis and therapy of acromegaly over two decades. J Clin Endocrinol Metab 93(6):2035–2041
Arafah BM (1986) Reversible hypopituitarism in patients with large nonfunctioning pituitary adenomas. J Clin Endocrinol Metab 62(6):1173–1179
Greenman Y, Tordjman K, Kisch E, Razon N, Ouaknine G, Stern N (1995) Relative sparing of anterior pituitary function in patients with growth hormone-secreting macroadenomas: comparison with nonfunctioning macroadenomas. J Clin Endocrinol Metab 80(5):1577–1583
Tominaga A, Uozumi T, Arita K, Kurisu K, Yano T, Hirohata T (1995) Anterior pituitary function in patients with nonfunctioning pituitary adenoma: results of longitudinal follow-up. Endocr J 42(3):421–427
Webb SM, Rigla M, Wagner A, Oliver B, Bartumeus F (1999) Recovery of hypopituitarism after neurosurgical treatment of pituitary adenomas. J Clin Endocrinol Metabolism 84(10):3696–3700
Giustina A, Chanson P, Kleinberg D, Bronstein MD, Clemmons DR, Klibanski A, van der Lely AJ, Strasburger CJ, Lamberts SW, Ho KK, Casanueva FF, Melmed S (2014) Expert consensus document: a consensus on the medical treatment of acromegaly. Nat Rev Endocrinol 10(4):243–248
Jane JA Jr, Starke RM, Elzoghby MA, Reames DL, Payne SC, Thorner MO, Marshall JC, Laws ER Jr, Vance ML (2011) Endoscopic transsphenoidal surgery for acromegaly: remission using modern criteria, complications, and predictors of outcome. J Clin Endocrinol Metab 96(9):2732–2740
Melmed S, Casanueva FF, Klibanski A, Bronstein MD, Chanson P, Lamberts SW, Strasburger CJ, Wass JA, Giustina A (2013) A consensus on the diagnosis and treatment of acromegaly complications. Pituitary 16(3):294–302
Starke RM, Raper DM, Payne SC, Vance ML, Oldfield EH, Jane JA Jr (2013) Endoscopic vs microsurgical transsphenoidal surgery for acromegaly: outcomes in a concurrent series of patients using modern criteria for remission. J Clin Endocrinol Metab 98(8):3190–3198
Burgers AM, Kokshoorn NE, Pereira AM, Roelfsema F, Smit JW, Biermasz NR, Romijn JA (2011) Low incidence of adrenal insufficiency after transsphenoidal surgery in patients with acromegaly: a long-term follow-up study. J Clin Endocrinol Metab 96(7):E1163–E1170
Ronchi CL, Ferrante E, Rizzo E, Giavoli C, Verrua E, Bergamaschi S, Lania AG, Beck-Peccoz P, Spada A (2008) Long-term basal and dynamic evaluation of hypothalamic-pituitary-adrenal (HPA) axis in acromegalic patients. Clin Endocrinol 69(4):608–612
Fleseriu M (2013) The role of combination medical therapy in acromegaly: hope for the nonresponsive patient. Curr Opin Endocrinol Diabetes Obes 20(4):321–329
Fleseriu M, Delashaw JB Jr, Cook DM (2010) Acromegaly: a review of current medical therapy and new drugs on the horizon. Neurosurg Focus 29(4):E15
Fleseriu M (2014) Advances in the pharmacotherapy of patients with acromegaly. Discov Med 18(96):329–338
Mestron A, Webb SM, Astorga R, Benito P, Catala M, Gaztambide S, Gomez JM, Halperin I, Lucas-Morante T, Moreno B, Obiols G, de Pablos P, Paramo C, Pico A, Torres E, Varela C, Vazquez JA, Zamora J, Albareda M, Gilabert M (2004) Epidemiology, clinical characteristics, outcome, morbidity and mortality in acromegaly based on the Spanish Acromegaly Registry (Registro Espanol de Acromegalia, REA). Eur J Endocrinol 151(4):439–446
Sherlock M, Reulen RC, Alonso AA, Ayuk J, Clayton RN, Sheppard MC, Hawkins MM, Bates AS, Stewart PM (2009) ACTH deficiency, higher doses of hydrocortisone replacement, and radiotherapy are independent predictors of mortality in patients with acromegaly. J Clin Endocrinol Metab 94(11):4216–4223
Sherlock M, Reulen RC, Aragon-Alonso A, Ayuk J, Clayton RN, Sheppard MC, Hawkins MM, Bates AS, Stewart PM (2014) A paradigm shift in the monitoring of patients with acromegaly: last available growth hormone may overestimate risk. J Clin Endocrinol Metab 99(2):478–485
Ben-Shlomo A (2010) Pituitary gland: predictors of acromegaly-associated mortality. Nat Rev Endocrinol 6(2):67–69
Sherlock M, Stewart PM (2013) Updates in growth hormone treatment and mortality. Curr Opin Endocrinol Diabetes Obes 20(4):314–320
Zueger T, Kirchner P, Herren C, Fischli S, Zwahlen M, Christ E, Stettler C (2012) Glucocorticoid replacement and mortality in patients with nonfunctioning pituitary adenoma. J Clin Endocrinol Metab 97(10):E1938–E1942
Fleseriu M, Gassner M, Yedinak C, Chicea L, Delashaw JB Jr, Loriaux DL (2010) Normal hypothalamic-pituitary-adrenal axis by high-dose cosyntropin testing in patients with abnormal response to low-dose cosyntropin stimulation: a retrospective review. Endocr Pract 16(1):64–70
Kazlauskaite R, Evans AT, Villabona CV, Abdu TA, Ambrosi B, Atkinson AB, Choi CH, Clayton RN, Courtney CH, Gonc EN, Maghnie M, Rose SR, Soule SG, Tordjman K (2008) Corticotropin tests for hypothalamic-pituitary- adrenal insufficiency: a metaanalysis. J Clin Endocrinol Metab 93(11):4245–4253
Beauregard C, Truong U, Hardy J, Serri O (2003) Long-term outcome and mortality after transsphenoidal adenomectomy for acromegaly. Clin Endocrinol 58(1):86–91
Swearingen B, Barker FG 2nd, Katznelson L, Biller BM, Grinspoon S, Klibanski A, Moayeri N, Black PM, Zervas NT (1998) Long-term mortality after transsphenoidal surgery and adjunctive therapy for acromegaly. J Clin Endocrinol Metab 83(10):3419–3426
Arafah BM, Prunty D, Ybarra J, Hlavin ML, Selman WR (2000) The dominant role of increased intrasellar pressure in the pathogenesis of hypopituitarism, hyperprolactinemia, and headaches in patients with pituitary adenomas. J Clin Endocrinol Metab 85(5):1789–1793
Berg C, Meinel T, Lahner H, Mann K, Petersenn S (2010) Recovery of pituitary function in the late-postoperative phase after pituitary surgery: results of dynamic testing in patients with pituitary disease by insulin tolerance test 3 and 12 months after surgery. Eur J Endocrinol 162(5):853–859
Marazuela M, Astigarraga B, Vicente A, Estrada J, Cuerda C, Garcia-Uria J, Lucas T (1994) Recovery of visual and endocrine function following transsphenoidal surgery of large nonfunctioning pituitary adenomas. J Endocrinol Investig 17(9):703–707
Wass JA, Reddy R, Karavitaki N (2011) The postoperative monitoring of nonfunctioning pituitary adenomas. Nat Rev Endocrinol 7(7):431–434
Caputo C, Sutherland T, Farish S, McNeill P, Ng KW, Inder WJ (2013) Gender differences in presentation and outcome of nonfunctioning pituitary macroadenomas. Clin Endocrinol 78(4):564–570
Ahmed S, Elsheikh M, Stratton IM, Page RC, Adams CB, Wass JA (1999) Outcome of transphenoidal surgery for acromegaly and its relationship to surgical experience. Clin Endocrinol 50(5):561–567
Buchfelder M, Schlaffer S (2009) Surgical treatment of pituitary tumours. Best Pract Res Clin Endocrinol Metab 23(5):677–692
Gittoes NJ, Sheppard MC, Johnson AP, Stewart PM (1999) Outcome of surgery for acromegaly–the experience of a dedicated pituitary surgeon. QJM 92(12):741–745
Beck-Peccoz P, Brucker-Davis F, Persani L, Smallridge RC, Weintraub BD (1996) Thyrotropin-secreting pituitary tumors. Endocr Rev 17(6):610–638
Luini A, Lewis D, Guild S, Schofield G, Weight F (1986) Somatostatin, an inhibitor of ACTH secretion, decreases cytosolic free calcium and voltage-dependent calcium current in a pituitary cell line. J Neurosci 6(11):3128–3132
Shimon I (2003) Somatostatin receptors in pituitary and development of somatostatin receptor subtype-selective analogs. Endocrine 20(3):265–269
Mazziotti G, Giustina A (2013) Glucocorticoids and the regulation of growth hormone secretion. Nat Rev Endocrinol 9(5):265–276
Giustina A, Veldhuis JD (1998) Pathophysiology of the neuroregulation of growth hormone secretion in experimental animals and the human. Endocr Rev 19(6):717–797
Agha A, Monson JP (2007) Modulation of glucocorticoid metabolism by the growth hormone–IGF-1 axis. Clin Endocrinol 66(4):459–465
Moore JS, Monson JP, Kaltsas G, Putignano P, Wood PJ, Sheppard MC, Besser GM, Taylor NF, Stewart PM (1999) Modulation of 11beta-hydroxysteroid dehydrogenase isozymes by growth hormone and insulin-like growth factor: in vivo and in vitro studies. J Clin Endocrinol Metab 84(11):4172–4177
Stewart PM, Toogood AA, Tomlinson JW (2001) Growth hormone, insulin-like growth factor-I and the cortisol-cortisone shuttle. Horm Res 56(Suppl.):11–16
Conflict of interest
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Yedinak, C., Hameed, N., Gassner, M. et al. Recovery rate of adrenal function after surgery in patients with acromegaly is higher than in those with non-functioning pituitary tumors: a large single center study. Pituitary 18, 701–709 (2015). https://doi.org/10.1007/s11102-015-0643-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-015-0643-8