
Abstract
Introduction
Radiation therapy is an important therapy for patients with Cushing’s disease who are not in remission or relapse after transsphenoidal pituitary surgery and are not considered surgical candidates. The development of stereotactic radiation therapy, using gamma knife, linear accelerators or proton beam based methods, has enabled selective radiation delivery to the target while minimizing exposure of healthy tissues. In patients whose tumors are sufficiently distant from the optic apparatus, stereotactic radiation therapy can be delivered in a single session, a procedure termed radiosurgery, which significantly improves patient convenience.
Methods
Original articles on radiation therapy in Cushing's disease, published during the past 12 months (2013–2014), were identified and pertinent data extracted.
Results
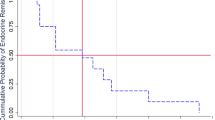
Recent studies have reported on the outcomes of patients with Cushing’s disease who received mostly stereotactic radiation therapy. While tumor control has been excellent, biochemical remission was less consistently achieved. Some studies suggested that stereotactic radiation may lead to biochemical remission faster than conventional radiation therapy. In addition, retrospective data have suggested that withdrawing medical therapy around the time stereotactic radiation therapy is administered might lead to a faster biochemical response. Regardless of the radiation therapy method, biochemical recurrences may develop and these patients are at long-term risk of developing anterior hypopituitarism and require lifelong periodic endocrine follow-up. Other, less frequent complications may include cranial neuropathies, secondary tumor formation or temporal lobe necrosis. It is plausible that complications may be less frequent after stereotactic radiation therapy, but this requires confirmation.
Conclusions
Radiation therapy is an effective second line therapy in patients with Cushing’s disease. Ongoing refinements in delivery of radiation therapy are anticipated to lead to improved patient outcomes, but long-term follow-up data, including adequate control groups, are needed to fully investigate this possibility.

Similar content being viewed by others


References
Biller BM, Grossman AB, Stewart PM, Melmed S, Bertagna X, Bertherat J, Buchfelder M, Colao A, Hermus AR, Hofland LJ, Klibanski A, Lacroix A, Lindsay JR, Newell-Price J, Nieman LK, Petersenn S, Sonino N, Stalla GK, Swearingen B, Vance ML, Wass JA, Boscaro M (2008) Treatment of adrenocorticotropin-dependent Cushing’s syndrome: a consensus statement. J Clin Endocrinol Metab 93:2454–2462
Swearingen B, Biller BM, Barker FG 2nd, Katznelson L, Grinspoon S, Klibanski A, Zervas NT (1999) Long-term mortality after transsphenoidal surgery for Cushing disease. Ann Intern Med 130:821–824
Tritos NA, Biller BM (2014) Cushing’s disease. Handb Clin Neurol 124:221–234
Tritos NA, Biller BM, Swearingen B (2011) Management of Cushing disease. Nat Rev Endocrinol 7:279–289
Loeffler JS, Shih HA (2011) Radiation therapy in the management of pituitary adenomas. J Clin Endocrinol Metab 96:1992–2003
Sheehan JP, Xu Z, Salvetti DJ, Schmitt PJ, Vance ML (2013) Results of gamma knife surgery for Cushing’s disease. J Neurosurg 119:1486–1492
Budyal S, Lila AR, Jalali R, Gupta T, Kasliwal R, Jagtap VS, Bandgar T, Menon P, Shah NS (2014) Encouraging efficacy of modern conformal fractionated radiotherapy in patients with uncured Cushing’s disease. Pituitary 17:60–67
Grant RA, Whicker M, Lleva R, Knisely JP, Inzucchi SE, Chiang VL (2014) Efficacy and safety of higher dose stereotactic radiosurgery for functional pituitary adenomas: a preliminary report. World Neurosurg 82:195–201
Wilson PJ, Williams JR, Smee RI (2014) Cushing’s disease: a single centre’s experience using the linear accelerator (LINAC) for stereotactic radiosurgery and fractionated stereotactic radiotherapy. J Clin Neurosci 21:100–106
Wattson DA, Tanguturi SK, Spiegel DY, Niemierko A, Biller BM, Nachtigall LB, Bussiere MR, Swearingen B, Chapman PH, Loeffler JS, Shih HA (2014) Outcomes of proton therapy for patients with functional pituitary adenomas. Int J Radiat Oncol Biol Phys 90:532–539
Mehta GU, Sheehan JP, Vance ML (2013) Effect of stereotactic radiosurgery before bilateral adrenalectomy for Cushing’s disease on the incidence of Nelson’s syndrome. J Neurosurg 119:1493–1497
Assie G, Bahurel H, Coste J, Silvera S, Kujas M, Dugue MA, Karray F, Dousset B, Bertherat J, Legmann P, Bertagna X (2007) Corticotroph tumor progression after adrenalectomy in Cushing’s disease: a reappraisal of Nelson’s syndrome. J Clin Endocrinol Metab 92:172–179
Wilson PJ, Williams JR, Smee RI (2014) Nelson’s syndrome: single centre experience using the linear accelerator (LINAC) for stereotactic radiosurgery and fractionated stereotactic radiotherapy. J Clin Neurosci 21:1520–1524
Conflict of interest
Dr. Tritos has served as the PI of research grants to MGH from Ipsen and Pfizer and has received occasional consulting honoraria from Pfizer and Corcept. Dr. Biller has served as the PI of research grants to MGH from Novartis and Cortendo and received occasional consulting honoraria from Novartis and Cortendo.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tritos, N.A., Biller, B.M.K. Update on radiation therapy in patients with Cushing’s disease. Pituitary 18, 263–268 (2015). https://doi.org/10.1007/s11102-014-0615-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-014-0615-4