
Abstract
Purpose
Exon 3-deleted GH receptor variant (d3-GHR) is associated with increased responsiveness to exogenous GH. The aim of this study was to determine the effect of d3-GHR polymorphism on the GH/IGF-1 relationship, clinical parameters, and comorbidity in acromegalic patients.
Methods
The study included 118 acromegalic patients (61 female and 57 male; mean age: 50.3 ± 12.2 years) and 108 healthy controls (94 female and 14 male: mean age: 41.1 ± 11.1 years). The prevalence of GHR genotypes was evaluated via PCR.
Results
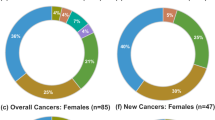
In all, 71 (60.2 %) patients had the fl/fl-GHR genotype, 40 (33.9 %) were heterozygous for the fl/d3-GHR genotype, and 7 (5.9 %) were homozygous for the d3/d3-GHR genotype. The prevalence of fl/fl-GHR, fl/d3-GHR, and d3/d3-GHR genotypes in the control group was 57.4, 29.6, and 13.0 %, respectively—similar prevalences as in the patient group. Patients that were heterozygous and homozygous for the d3 allele were subgrouped (d3-GHR subgroup), and were compared to those with the fl/fl-GHR genotype (fl/fl-GHR subgroup). Anthropometric measures, features of pituitary adenoma, and baseline GH and IGF-1 levels were similar in both subgroups. The prevalence of coronary artery disease, hypertension, hyperlipidemia, type 2 diabetes mellitus, and multinodular goiter did not differ between patient subgroups. In total, 24 (20.3 %) of the patients had cancer and the prevalence of cancer was similar in the d3-GHR (14.9 %) and fl/fl-GHR (23.9 %) subgroups (P = 0.23). More of the acromegalic patients that were d3 carriers had discordant GH and IGF-1 levels at baseline and post surgery, but the difference was not significant. A significant correlation between basal GH and IGF-1 levels was observed only in the patients with the fl/fl-GHR genotype (R2 = 0.227, P < 0.001).
Conclusion
The d3-GHR variant genotype did not have an effect on clinical features or comorbidity in acromegalic patients, but it might play a role in GH/IGF-1 level discordance in acromegaly.

Similar content being viewed by others

References
Colao A, Ferone D, Marzullo P, Lombardi G (2004) Systemic complications of acromegaly: epidemiology, pathogenesis, and management. Endocr Rev 25(1):102–152
Dogan S, Atmaca A, Dagdelen S, Erbas B, Erbas T (2013) Evaluation of thyroid diseases and differentiated thyroid cancer in acromegalic patients. Endocrine. doi:10.1007/s12020-013-9981-3
Beckers A, Aaltonen LA, Daly AF, Karhu A (2013) Familial isolated pituitary adenomas (FIPA) and the pituitary adenoma predisposition due to mutations in the aryl hydrocarbon receptor interacting protein (AIP) gene. Endocr Rev 34(2):239–277. doi:10.1210/er.2012-1013
Cannavo S, Ferrau F, Ragonese M, Curto L, Torre ML, Magistri M, Marchese A, Alibrandi A, Trimarchi F (2010) Increased prevalence of acromegaly in a highly polluted area. Eur J Endocrinol 163(4):509–513. doi:10.1530/EJE-10-0465
Leung DW, Spencer SA, Cachianes G, Hammonds RG, Collins C, Henzel WJ, Barnard R, Waters MJ, Wood WI (1987) Growth hormone receptor and serum binding protein: purification, cloning and expression. Nature 330(6148):537–543. doi:10.1038/330537a0
Pantel J, Machinis K, Sobrier ML, Duquesnoy P, Goossens M, Amselem S (2000) Species-specific alternative splice mimicry at the growth hormone receptor locus revealed by the lineage of retroelements during primate evolution. J Biol Chem 275(25):18664–18669. doi:10.1074/jbc.M001615200
Dos Santos C, Essioux L, Teinturier C, Tauber M, Goffin V, Bougneres P (2004) A common polymorphism of the growth hormone receptor is associated with increased responsiveness to growth hormone. Nat Genet 36(7):720–724. doi:10.1038/ng1379
Audi L, Esteban C, Carrascosa A, Espadero R, Perez-Arroyo A, Arjona R, Clemente M, Wollmann H, Fryklund L, Parodi LA (2006) Exon 3-deleted/full-length growth hormone receptor polymorphism genotype frequencies in Spanish short small-for-gestational-age (SGA) children and adolescents (n = 247) and in an adult control population (n = 289) show increased fl/fl in short SGA. J Clin Endocrinol Metab 91(12):5038–5043. doi:10.1210/jc.2006-0828
Sobrier ML, Duquesnoy P, Duriez B, Amselem S, Goossens M (1993) Expression and binding properties of two isoforms of the human growth hormone receptor. FEBS Lett 319(1–2):16–20
Binder G, Baur F, Schweizer R, Ranke MB (2006) The d3-growth hormone (GH) receptor polymorphism is associated with increased responsiveness to GH in Turner syndrome and short small-for-gestational-age children. J Clin Endocrinol Metab 91(2):659–664. doi:10.1210/jc.2005-1581
Wickelgren RB, Landin KL, Ohlsson C, Carlsson LM (1995) Expression of exon 3-retaining and exon 3 excluding isoforms of the human growth hormone-receptor is regulated in an interindividual, rather than a tissue specific, manner. J Clin Endocrinol Metab 80(7):2154–2157
Jorge AA, Marchisotti FG, Montenegro LR, Carvalho LR, Mendonca BB, Arnhold IJ (2006) Growth hormone (GH) pharmacogenetics: influence of GH receptor exon 3 retention or deletion on first-year growth response and final height in patients with severe GH deficiency. J Clin Endocrinol Metab 91(3):1076–1080. doi:10.1210/jc.2005-2005
Carrascosa A, Esteban C, Espadero R, Fernandez-Cancio M, Andaluz P, Clemente M, Audi L, Wollmann H, Fryklund L, Parodi L (2006) The d3/fl-growth hormone (GH) receptor polymorphism does not influence the effect of GH treatment (66 microg/kg per day) or the spontaneous growth in short non-GH deficient small-for-gestational-age children: results from a two-year controlled prospective study in 170 Spanish, patients. J Clin Endocrinol Metab 91(9):3281–3286. doi:10.1210/jc.2006-0685
Blum WF, Machinis K, Shavrikova EP, Keller A, Stobbe H, Pfaeffle RW, Amselem S (2006) The growth response to growth hormone (GH) treatment in children with isolated GH deficiency is independent of the presence of the exon 3-minus isoform of the GH receptor. J Clin Endocrinol Metab 91(10):4171–4174. doi:10.1210/jc.2006-0063
van der Klaauw AA, van der Straaten T, Baak-Pablo R, Biermasz NR, Guchelaar HJ, Pereira AM, Smit JW, Romijn JA (2008) Influence of the d3-growth hormone (GH) receptor isoform on short-term and long term treatment response to GH replacement in GH-deficient adults. J Clin Endocrinol Metab 93(7):2828–2834. doi:10.1210/jc.2007-2728
Moyes VJ, Walker DM, Owusu-Antwi S, Maher KT, Metherell L, Akker SA, Monson JP, Clark AJ, Drake WM (2010) d3-GHR genotype does not explain heterogeneity in GH responsiveness in hypopituitary adults. Clin Endocrinol (Oxf) 72(6):807–813. doi:10.1111/j.1365-2265.2009.03768.x
Barbosa EJ, Palming J, Glad CA, Filipsson H, Koranyi J, Bengtsson BA, Carlsson LM, Boguszewski CL, Johannsson G (2009) Influence of the exon 3-deleted/full-length growth hormone (GH) receptor polymorphism on the response to GH replacement therapy in adults with severe GH deficiency. J Clin Endocrinol Metab 94(2):639–644. doi:10.1210/jc.2008-0323
Adetunji OR, MacFarlane IA, Javadpour M, Alfirevic A, Pirmohamed M, Blair JC (2009) The d3/fl-GH receptor gene polymorphism does not influence quality of life and body composition in GH-deficient adults receiving GH replacement therapy. Eur J Endocrinol 161(4):541–546. doi:10.1530/EJE-09-0405
Sorensen K, Aksglaede L, Munch-Andersen T, Aachmann-Andersen NJ, Leffers H, Helge JW, Hilsted L, Juul A (2009) Impact of the growth hormone receptor exon 3 deletion gene polymorphism on glucose metabolism, lipids, and insulin-like growth factor-I levels during puberty. J Clin Endocrinol Metab 94(8):2966–2969. doi:10.1210/jc.2009-0313
Strawbridge RJ, Karvestedt L, Li C, Efendic S, Ostenson CG, Gu HF, Brismar K (2007) GHR exon 3 polymorphism: association with type 2 diabetes mellitus and metabolic disorder. Growth Horm IGF Res 17(5):392–398. doi:10.1016/j.ghir.2007.04.005
Horan M, Newsway V, Lewis MD, Easter TE, Rees DA, Mahto A, Millar DS, Procter AM, Scanlon MF, Wilkinson IB, Hall IP, Wheatley A, Blakey J, Bath PM, Cockcroft JR, Krawczak M, Cooper DN (2006) Genetic variation at the growth hormone (GH1) and growth hormone receptor (GHR) loci as a risk factor for hypertension and stroke. Hum Genet 119(5):527–540. doi:10.1007/s00439-006-0166-5
Audi L, Carrascosa A, Esteban C, Fernandez-Cancio M, Andaluz P, Yeste D, Espadero R, Granada ML, Wollmann H, Fryklund L (2008) The exon 3-deleted/full-length growth hormone receptor polymorphism does not influence the effect of puberty or growth hormone therapy on glucose homeostasis in short non-growth hormone-deficient small-for-gestational-age children: results from a two-year controlled prospective study. J Clin Endocrinol Metab 93(7):2709–2715. doi:10.1210/jc.2008-0150
Mercado M, Gonzalez B, Sandoval C, Esquenazi Y, Mier F, Vargas G, de los Monteros AL, Sosa E (2008) Clinical and biochemical impact of the d3 growth hormone receptor genotype in acromegaly. J Clin Endocrinol Metab 93(9):3411–3415. doi:10.1210/jc.2008-0391
Schmid C, Krayenbuehl PA, Bernays RL, Zwimpfer C, Maly FE, Wiesli P (2007) Growth hormone (GH) receptor isoform in acromegaly: lower concentrations of GH but not insulin-like growth factor-1 in patients with a genomic deletion of exon 3 in the GH receptor gene. Clin Chem 53(8):1484–1488. doi:10.1373/clinchem.2007.085712
Montefusco L, Filopanti M, Ronchi CL, Olgiati L, La-Porta C, Losa M, Epaminonda P, Coletti F, Beck-Peccoz P, Spada A, Lania AG, Arosio M (2010) d3-Growth hormone receptor polymorphism in acromegaly: effects on metabolic phenotype. Clin Endocrinol (Oxf) 72(5):661–667. doi:10.1111/j.13652265.2009.03703.x
Wassenaar MJ, Biermasz NR, Pereira AM, van der Klaauw AA, Smit JW, Roelfsema F, van der Straaten T, Cazemier M, Hommes DW, Kroon HM, Kloppenburg M, Guchelaar HJ, Romijn JA (2009) The exon-3 deleted growth hormone receptor polymorphism predisposes to long-term complications of acromegaly. J Clin Endocrinol Metab 94(12):4671–4678. doi:10.1210/jc.2009-1172
Turgut S, Akin F, Ayada C, Topsakal S, Yerlikaya E, Turgut G (2012) The growth hormone receptor polymorphism in patients with acromegaly: relationship to BMI and glucose metabolism. Pituitary 15(3):374–379. doi:10.1007/s11102-011-0329-9
Brzana JA, Yedinak CG, Delashaw JB, Gultelkin HS, Cook D, Fleseriu M (2012) Discordant growth hormone and IGF-1 levels post pituitary surgery in patients with acromegaly naive to medical therapy and radiation: what to follow, GH or IGF-1 values? Pituitary 15(4):562–570. doi:10.1007/s11102-011-0369-1
Alexopoulou O, Bex M, Abs R, T’Sjoen G, Velkeniers B, Maiter D (2008) Divergence between growth hormone and insulin-like growth factor-i concentrations in the follow-up of acromegaly. J Clin Endocrinol Metab 93(4):1324–1330. doi:10.1210/jc.2007-2104
Melmed S, Jackson I, Kleinberg D, Klibanski A (1998) Current treatment guidelines for acromegaly. J Clin Endocrinol Metab 83(8):2646–2652
Giustina A, Barkan A, Casanueva FF, Cavagnini F, Frohman L, Ho K, Veldhuis J, Wass J, Von Werder K, Melmed S (2000) Criteria for cure of acromegaly: a consensus statement. J Clin Endocrinol Metab 85(2):526–529. doi:10.1210/jcem.85.2.6363
Tiryakioglu O, Kadiolgu P, Canerolgu NU, Hatemi H (2003) Age dependency of serum insulin: like growth factor (IGF)-1 in healthy Turkish adolescents and adults. Indian J Med Sci 57(12):543–548
Mercado M, Espinosa de los Monteros AL, Sosa E, Cheng S, Mendoza V, Hernandez I, Sandoval C, Guinto G, Molina M (2004) Clinical-biochemical correlations in acromegaly at diagnosis and the real prevalence of biochemically discordant disease. Horm Res 62(6):293–299. doi:10.1159/000082032
Bianchi A, Giustina A, Cimino V, Pola R, Angelini F, Pontecorvi A, De Marinis L (2009) Influence of growth hormone receptor d3 and full-length isoforms on biochemical treatment outcomes in acromegaly. J Clin Endocrinol Metab 94(6):2015–2022. doi:10.1210/jc.2008-1337
Kamenicky P, Dos Santos C, Espinosa C, Salenave S, Galland F, Le Bouc Y, Maison P, Bougneres P, Chanson P (2009) D3 GH receptor polymorphism is not associated with IGF1 levels in untreated acromegaly. Eur J Endocrinol 161(2):231–235. doi:10.1530/EJE-09-0053
Filopanti M, Olgiati L, Mantovani G, Corbetta S, Arosio M, Gasco V, De Marinis L, Martini C, Bogazzi F, Cannavo S, Colao A, Ferone D, Arnaldi G, Pigliaru F, Peri A, Angeletti G, Jaffrain-Rea ML, Lania AG, Spada A (2012) Growth hormone receptor variants and response to pegvisomant in monotherapy or in combination with somatostatin analogs in acromegalic patients: a multicenter study. J Clin Endocrinol Metab 97(2):E165–E172. doi:10.1210/jc.2011-1769
Dagdelen S, Cinar N, Erbas T (2013) Increased thyroid cancer risk in acromegaly. Pituitary. doi:10.1007/s11102-013-0501-5
Wagner K, Hemminki K, Grzybowska E, Bermejo JL, Butkiewicz D, Pamula J, Pekala W, Forsti A (2006) Polymorphisms in the growth hormone receptor: a case-control study in breast cancer. Int J Cancer 118(11):2903–2906. doi:10.1002/ijc.21703
Acknowledgments
We thank the Damagen Genetic Research and Diagnostic Co. for their help in genetic analysis. The study was funded by Hacettepe University Scientific Research Projects Coordination Unit (Project number: 010D09101002).
Conflict of interest
The authors have nothing to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cinar, N., Dagdelen, S., Yorgun, H. et al. The clinical and cardiometabolic effects of d3-growth hormone receptor polymorphism in acromegaly. Pituitary 18, 116–125 (2015). https://doi.org/10.1007/s11102-014-0564-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-014-0564-y