
Abstract
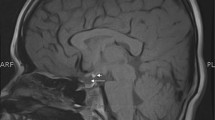
The pituitary stalk transection syndrome was characterized after introducing the MRI scan in the evaluation of children with hypopituitarism. Its prevalence and natural history into adulthood have not been clearly established. We present 4 cases of stalk transection syndrome diagnosed by the adult endocrinologist that reflect its pleiotropic manifestations. In all cases, MRI showed pathognomonic findings with small anterior pituitary, diminutive or absent infundibulum and ectopic posterior pituitary at the median eminence. Clinical presentation occurred in childhood or the second decade of life. The hormonal deficits were variable in severity and onset, with adrenal insufficiency diagnosed in the second and forth decade in three patients, and absent in another. Growth hormone deficiency was diagnosed before age 10 in three cases and at age 20 in one case with normal spontaneous linear growth. Hypothyroidism had onset in the first or second decade of life and hypogonadism was diagnosed during work-up for lack of pubertal development in all cases. The pituitary stalk transection syndrome should be considered in patients who were previously thought to have idiopathic GH deficiency or multiple pituitary hormone deficiencies. Presence of MRI characteristics compatible with the pituitary stalk transection syndrome should prompt a full pituitary hormonal evaluation. Long-term follow-up by the adult endocrinologist is warranted as new hormone deficiencies might appear later in life.

Similar content being viewed by others


References
Melmed S (2003) Mechanisms for pituitary tumorigenesis: the plastic pituitary. J Clin Invest 112(11):1603–1618
Struthers RS, Vale WW, Arias C, Sawchenko PE, Montminy MR (1991) Somatotroph hypoplasia and dwarfism in transgenic mice expressing a non-phosphorylatable CREB mutant. Nature 350(6319):622–624
Fujisawa I, Kikuchi K, Nishimura K, Togashi K, Itoh K, Noma S, Minami S, Sagoh T, Hiraoka T, Momoi T et al (1987) Transection of the pituitary stalk: development of an ectopic posterior lobe assessed with MR imaging. Radiology 165(2):487–489
Fernandez-Rodriguez E, Quinteiro C, Barreiro J, Marazuela M, Pereiro I, Peino R, Cabezas-Agricola JM, Dominguez F, Casanueva FF, Bernabeu I (2011) Pituitary stalk dysgenesis-induced hypopituitarism in adult patients: prevalence, evolution of hormone dysfunction and genetic analysis. Neuroendocrinology 93(3):181–188
Abrahams JJ, Trefelner E, Boulware SD (1991) Idiopathic growth hormone deficiency: MR findings in 35 patients. AJNR Am J Neuroradiol 12(1):155–160
Patkar D, Patankar T, Krishnan A, Prasad S, Shah J, Limdi J (1999) MR imaging in children with ectopic pituitary gland and anterior hypopituitarism. J Postgrad Med 45(3):81–83
Chen S, Leger J, Garel C, Hassan M, Czernichow P (1999) Growth hormone deficiency with ectopic neurohypophysis: anatomical variations and relationship between the visibility of the pituitary stalk asserted by magnetic resonance imaging and anterior pituitary function. J Clin Endocrinol Metab 84(7):2408–2413
Genovese E, Maghnie M, Beluffi G, Villa A, Sammarchi L, Severi F, Campani R (1997) Hypothalamic-pituitary vascularization in pituitary stalk transection syndrome: is the pituitary stalk really transected? The role of gadolinium-DTPA with spin-echo T1 imaging and turbo-FLASH technique. Pediatr Radiol 27(1):48–53
Deladoey J, Fluck C, Buyukgebiz A, Kuhlmann BV, Eble A, Hindmarsh PC, Wu W, Mullis PE (1999) Hot spot in the PROP1 gene responsible for combined pituitary hormone deficiency. J Clin Endocrinol Metab 84(5):1645–1650
Vallette-Kasic S, Barlier A, Teinturier C, Diaz A, Manavela M, Berthezene F, Bouchard P, Chaussain JL, Brauner R, Pellegrini-Bouiller I et al (2001) PROP1 gene screening in patients with multiple pituitary hormone deficiency reveals two sites of hypermutability and a high incidence of corticotroph deficiency. J Clin Endocrinol Metab 86(9):4529–4535
Irie Y, Tatsumi K, Kusuda S, Kawawaki H, Boyages SC, Nose O, Ichiba Y, Katsumata N, Amino N (1995) Screening for PIT1 abnormality by PCR direct sequencing method. Thyroid 5(3):207–211
Kelberman D, Dattani MT (2007) Hypopituitarism oddities: congenital causes. Horm Res 68(Suppl 5):138–144
Arifa N, Leger J, Garel C, Czernichow P, Hassan M (1999) Cerebral anomalies associated with growth hormone insufficiency in children: major markers for diagnosis? Arch Pediatr 6(1):14–21
Hamilton J, Blaser S, Daneman D (1998) MR imaging in idiopathic growth hormone deficiency. AJNR Am J Neuroradiol 19(9):1609–1615
Melmed S, Kleinberg D (2002) In: Williams textbook of endocrinology, 10th edn. Elsevier, Amsterdam, Holland, p 178
Kikuchi K, Fujisawa I, Momoi T, Yamanaka C, Kaji M, Nakano Y, Konishi J, Mikawa H, Sudo M (1988) Hypothalamic-pituitary function in growth hormone-deficient patients with pituitary stalk transection. J Clin Endocrinol Metab 67(4):817–823
Barbeau C, Jouret B, Gallegos D, Sevely A, Manelfe C, Oliver I, Pienkowski C, Tauber MT, Rochiccioli P (1998) Pituitary stalk transection syndrome. Arch Pediatr 5(3):274–279
Maghnie M, Larizza D, Triulzi F, Sampaolo P, Scotti G, Severi F (1991) Hypopituitarism and stalk agenesis: a congenital syndrome worsened by breech delivery? Horm Res 35(3–4):104–108
Badawy SZ, Pisarska MD, Wasenko JJ, Buran JJ (1994) Congenital hypopituitarism as part of suprasellar dysplasia. A case report. J Reprod Med 39(8):643–648
Den Ouden DT, Kroon M, Hoogland PH, Geelhoed-Duijvestijn PH, Wit JM (2002) A 43-year-old male with untreated panhypopituitarism due to absence of the pituitary stalk: from dwarf to giant. J Clin Endocrinol Metab 87(12):5430–5434
Kageyama K, Watanobe H, Nasushita R, Nishie M, Horiba N, Suda T (1998) A hypopituitary patient who attained tall stature without growth hormone. Intern Med 37(5):472–475
Papastathopoulou L, Tzanela M, Vlassopoulou V, Vassiliadi D, Thalassinos N (2006) Untreated hypopituitarism due to absence of the pituitary stalk with normal adult height: report of two cases. Endocrine 29(1):175–179
Wada S, Minagawa A, Imamaki K, Suda S, Yamanaka K, Iitaka M, Katayama S (2000) A patient of hypogonadotropic hypogonadism accompanied by growth hormone deficiency and decreased bone mineral density who attained normal growth. Intern Med 39(8):641–645
Kornreich L, Horev G, Lazar L, Schwarz M, Sulkes J, Pertzelan A (1998) MR findings in growth hormone deficiency: correlation with severity of hypopituitarism. AJNR Am J Neuroradiol 19(8):1495–1499
Leger J, Danner S, Simon D, Garel C, Czernichow P (2005) Do all patients with childhood-onset growth hormone deficiency (GHD) and ectopic neurohypophysis have persistent GHD in adulthood? J Clin Endocrinol Metab 90(2):650–656
Gotyo N, Doi M, Izumiyama H, Hirata Y (2007) Secondary adrenal insufficiency caused by adult development of pituitary stalk transection. Intern Med 46(20):1711–1715
Pentimone F, Riccioni S, Del Corso L (1999) Congenital hypopituitarism in a 48-year old adult. Natural course, hormonal study and MRI evidence. Panminerva Med 41(4):351–354
Lamesch C, Neumann S, Pfaffle R, Kiess W, Paschke R (2002) Adrenocorticotrope deficiency with clinical evidence for late onset in combined pituitary hormone deficiency caused by a homozygous 301–302delAG mutation of the PROP1 gene. Pituitary 5(3):163–168
Hakkaart-van Roijen L, Beckers A, Stevenaert A, Rutten FF (1998) The burden of illness of hypopituitary adults with growth hormone deficiency. Pharmacoeconomics 14(4):395–403
Sherlock M, Ayuk J, Tomlinson JW, Toogood AA, Aragon-Alonso A, Sheppard MC, Bates AS, Stewart PM (2010) Mortality in patients with pituitary disease. Endocr Rev 31(3):301–342
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ioachimescu, A.G., Hamrahian, A.H., Stevens, M. et al. The pituitary stalk transection syndrome: multifaceted presentation in adulthood. Pituitary 15, 405–411 (2012). https://doi.org/10.1007/s11102-011-0337-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-011-0337-9