
Abstract
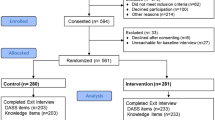
Background Although warfarin is highly effective, management of patients prescribed warfarin is complex due to its narrow therapeutic window. Objective To evaluate the impact of a formal warfarin discharge education program (WDEP) on hospital readmission and treatment costs in patients who received warfarin therapy. Setting Robert Wood Johnson University Hospital Somerset in Somerville, New Jersey, USA. Method In this interventional cohort study, patients were assigned to either the WDEP group or the usual care group. The effects of the WDEP on readmission within 90 days after discharge were analyzed using Cox proportional hazards models. Factors influencing treatment cost were identified using generalized linear model with log-link function and gamma distribution. Main outcome measure Hospital readmission within 90 days and treatment costs associated with hospital readmission. Results Among 692 eligible patients, 203 in each group were matched using propensity scores and there were no statistically significant differences in the patient baseline characteristics between two groups. The risk of all-cause readmission within 90 days was significantly lower in the WDEP group compared to the usual care group (relative risk = 0.46, 95% CI 0.28–0.76). The treatment costs associated with hospital readmission in the WDEP group were 19% lower than those in the usual care group after adjusting for the study variables. Conclusion A formal, individualized WDEP provided by pharmacists resulted in significant reduction of readmission and treatment costs. The economic burden of treatment costs associated with warfarin can be controlled if well-organized warfarin education is provided to patients who received warfarin therapy.


Similar content being viewed by others


References
Kimmel SE. Warfarin therapy: in need of improvement after all these years. Expert Opin Pharmacother. 2008;9(5):677–86.
Schwarz UI, Ritchie MD, Bradford Y, Li C, Dudek SM, Frye-Anderson A, et al. Genetic determinants of response to warfarin during initial anticoagulation. N Engl J Med. 2008;358(10):999–1008.
Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use—a prevalent adverse effect resulting in regulatory action. Arch Intern Med. 2007;167(13):1414–9.
The Joint Commission. National Patient Safety Goals: Hospital Accreditation Program. 2017. http://www.jointcommission.org/assets/1/6/NPSG_Chapter_HAP_Jan2017.pdf. Accessed 20 Dec 2017.
Daniel SB, Lovegrove MC, Shehab N, Richards CL. Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med. 2011;365(21):2002–12.
Kimmel SE, Chen Z, Price M, Parker CS, Metlay JP, Christie JD, et al. The influence of patient adherence on anticoagulation control with warfarin—results from the International Normalized Ratio Adherence and Genetics (IN-RANGE) Study. Arch Intern Med. 2007;167(3):229–35.
van Walraven C, Jennings A, Oake N, Fergusson D, Forster AJ. Effect of study setting on anticoagulation control—a systematic review and metaregression. Chest. 2006;129(5):1155–66.
Oden A, Fahlen M. Oral anticoagulation and risk of death: a medical record linkage study. Br Med J. 2002;325(7372):1073–5.
Kagansky N, Knobler H, Rimon E, Ozer Z, Levy S. Safety of anticoagulation therapy in well-informed older patients. Arch Intern Med. 2004;164(18):2044–50.
Beyth RJ, Landefeld CS. Learning the respective roles of warfarin and dabigatran to prevent stroke in patients with nonvalvular atrial fibrillation. Ann Intern Med. 2011;155(10):714–5 W218.
Hu A, Chow CM, Dao D, Errett L, Keith M. Factors influencing patient knowledge of warfarin therapy after mechanical heart valve replacement. J Cardiovasc Nurs. 2006;21(3):169–75.
Rosner B. Fundamentals of Biostatistics. 8th ed. Brooks: Cole Cengage Learning; 2015.
Dager WE, Branch JM, King JH, White RH, Quan RS, Musallam NA, et al. Optimization of inpatient warfarin therapy: impact of daily consultation by a pharmacist-managed anticoagulation service. Ann Pharmacother. 2000;34:567–72.
Rosenbaum PR, Rubin DD. Reducing bias in observational studies using subclassification on the propensity score. J Am Stat Assoc. 1984;79:516–24.
D’agostino RB. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat Med. 1998;17:2265–81.
Sturmer T, Joshi M, Glynn RJ, Avorn J, Rothman KJ, Schneeweiss S. A review of the application of propensity score methods yielded increasing use, advantages in specific settings, but not substantially different estimates compared with conventional multivariable methods. J Clin Epidemiol. 2006;59:437–47.
Gu XS, Rosenbaum PR. Comparison of multivariate matching methods: structures, distances, and algorithms. J Comput Graph Stat. 1993;2(4):405–20.
Hosmer DW, Lemeshow S. Applied logistic regression. 3rd ed. New York, NY: Wiley; 2013.
Efron B, Tibshirani RJ. An introduction to the bootstrap. Boca Raton, FL: Chapman & Hall/CRC; 1993.
Akaike H. Information theory and an extension of the maximum likelihood principle. In: Petrov BN, Caski F, editors. Proceedings of the second international symposium on information theory. Budapest: Akademiai Kiado; 1973:267–81.
Anderson DR, Burnham KP. Model selection and multimodel inference: a practical information-theoretic approach. New York: Springer; 2011.
White RH, Beyth RJ, Zhou H, Romano PS. Major bleeding after hospitalization for deep-venous thrombosis. Am J Med. 1999;107(5):414–24.
Wofford JL, Wells MD, Singh S. Best strategies for patient education about anticoagulation with warfarin: a systematic review. BMC Health Serv Res. 2008;8:40. https://doi.org/10.1186/472-6963-8-40.
Wilhelm SM, Petrovitch EA. Implementation of an inpatient anticoagulation teaching service: expanding the role of pharmacy students and residents in patient education. Am J Health Syst Pharm. 2011;68(21):2086–93.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–9.
Spyropoulos AC, Lin J. Direct medical costs of venous thromboembolism and subsequent hospital readmission rates: an administrative claims analysis from 30 managed care organizations. J Manag Care Pharm. 2007;13(6):475–86.
Nasir K, Lin ZQ, Bueno H, Normand SLT, Drye EE, Keenan PS, et al. Is same-hospital readmission rate a good surrogate for all-hospital readmission rate? Med Care. 2010;48(5):477–81.
Acknowledgements
We would like to thank Ms. Seyunghe Je and Mr. Sung-su Lee for their assiatance with searching articles and initial data entry.
Funding
This research was supported by Chung-Ang University Research Scholarship grants (Seoul, South Korea) awarded in 2016.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
All the authors declare that there is no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Brunetti, L., Lee, SM., Doherty, N. et al. Impact of warfarin discharge education program on hospital readmission and treatment costs. Int J Clin Pharm 40, 721–729 (2018). https://doi.org/10.1007/s11096-018-0631-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11096-018-0631-y