
Abstract
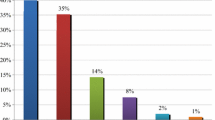
Objective The aim of this study was to clarify the number and type of discrepancies between four medication sources as well as their potential clinical significance to the patient. Method The study was conducted as a cross-sectional study comprising all patients hospitalised with hip fractures in the Orthopaedic Surgery Ward at Amager Hospital. Data were collected from four sources. All information was counted, and the potential clinical significance of discrepancies was evaluated on a five-point scale. The four sources are: patients, the Personal Electronic Medication Profile (PEM), the general practitioner (GP) and the in-home care provider. A discrepancy was defined as any disagreement or omission of information between the four sources concerning name, form, strength and dose for each drug with which the patient was being treated. Main outcome measure The number of discrepancies between the data sources. Results A total of 69 medications were registered for nine patients or an average of 7.7 medications per patient. 10.1 discrepancies per patient and 1.3 discrepancies per drug were registered. Two discrepancies were assessed as having potentially lethal clinical significance. Forty-one discrepancies were assessed as clinically significant, while 36 discrepancies were assessed as possessing minor clinical significance. The PEM added nine prescription drugs that no other sources mentioned. The addition of these medicines was largely clinically significant. Conclusion A total of 91 discrepancies were registered for nine patients. Two of these discrepancies were fatal and 41 were clinically significant.


Similar content being viewed by others

References
Foss S, Schmidt JR, Andersen T, Rasmussen JJ, Damsgaard J, Schaefer K, Munck LK. Congruence on medication between patients and physicians involved in patient course. Eur J Clin Pharmacol. 2004;59:841–7.
Rabøl R, Arroe GR, Folke F, Madsen KR, Langergaard MT, Larsen AH, Budek T, Andersen JR. Uoverensstemmelser mellem medicinoplysninger fra patienter og egen læge. [Discrepancy between physicians’ medication records and information given by patients. In Danish]. Ugeskr Laeger. 2006;168:1307–10.
Folli HL, Poole RL, Benitz WE, Russo JC. Medication error prevention by clinical pharmacists in two children’s hospitals. Paediatrics. 1987;79(5):718–22.
Tam VC, Knowlea SR, Cornish PL, Fine N, Marchesano R, Etchells EE. Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. JAMC. 2005;173(5):510–5.
Cornish PL, Knowles SR, Marchesano R, Tam V, Shadowitz S, Juurlink DN, Etchells EE. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165:424–9.
Glintborg B, Andersen SE, Dalhoff K. Insufficient communication about medication use at the interface between hospital and primary care. Qual Saf Health Care. 2007;16:34–9.
Barat I, Andreasen F, Damsgaard EM. Drug therapy in the elderly: what doctors believe and patients actually do. Br J Clin Pharmacol. 2001;51:615–22.
Andersen SE, Pedersen AB, Bach KF. Medication history on internal medicine wards: assessment of extra information collected from second drug interviews and GP lists. Pharmacoepidemiol Drug Saf. 2003;12:491–8.
Lau HS, Florax C, Porsius AJ, Boer A. The completeness of medication histories in hospital medical records of patients admitted to general internal medicine wards. Br J Clin Pharmacol. 2000;49:597–603.
Larsen MD, Nielsen LP, Jeffery L, Stæhr ME. Medicineringsfejl ved indlæggelse påsygehus [Medication errors in conjunction with hospitalisation. In Danish] Ugeskr Læger. 2006;168(35):2887–90.
Beers MH, Munekata M, Storrie M. The accuracy of medication histories in the hospital medical records of elderly persons. JAGS. 1990;38:1183–7.
Caskie GIL, Willis SL. Congruence of self-reported medications with pharmacy prescription records in low-income older adults. The Gerontologist. 2004;44(2):176–85.
Glintborg B, Hillestrøm PR, Olsen LH, Dalhoff K, Poulsen HE. Are patients reliable when self-reporting medication use? Validation of structured drug interviews and home visits by drug analysis and prescription data in acutely hospitalized persons. J Clin Pharmacol. 2007;47(11):1440–9.
Glintborg B, Poulsen HE, Dalhoff K. The use of nation-wide online prescription records improves the drug history in hospitalized patients. Br J Clin Pharmacol. 2007;65(2):265–9.
Overhage JM, Lukes A. Practical, reliable, comprehensive method for characterizing pharmacists’ clinical activities. Am J Health-Syst Pharm. 1999;56:2444–50.
Lisby M, Nielsen LP, Mainz J. Error in the medication process: frequency, type, and potential. Int J Qual Health Care. 2005;17(1):15–22.
Price D, Cooke J, Singleton S, Feely M. Doctors’ unawareness of the drugs their patients are taking: a major cause of overprescribing? BMJ. 1986;292:99–100.
Burda SA, Hobson D, Pronovost PJ. What is the patient really taking? Discrepancies between surgery and anaesthesiology preoperative medication histories. Qual Saf Health Care. 2005;14:414–6.
Baum C, Forbes MB, Kennedy DL, Jones JK. Patient drug profiles and medical records as sources of hospital drug-use information. Am J Hosp Pharm. 1983;40(12):2191–3.
Eggers AH. Fælles Medicinkort på vej [Common medicine cards on the way. In Danish]. Farmaci 2008;11:10–11.
Lægemiddelstyrelsen—Faktablad. Det fælles medicinkort [The Danish Medicines Agency—Fact sheet. The common medicine card. In Danish]. 2008 (http://admin.laegemiddelstyrelsen.dk/db/filarkiv/7675/FFlles%20medicinkort%20-%20medicinbruger_Medicin-IT.pdf).
Acknowledgements
The authors thank Jan Andersen, Chief Physician, at the Orthopaedic Surgery Ward at Amager Hospital, Anders Peter Balslev-Clausen, Resident, at the Orthopaedic Surgery Ward at Amager Hospital and Louise G. Gammelgaard, Clinical Pharmacist, at Amager Hospital for their help in the evaluation of the detected discrepancies. We would also like to thank participating staff for their help in finding eligible patients.
Funding
There has been no funding for this study.
Conflicts of interest
None declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Karkov, L.L., Schytte-Hansen, S. & Haugbølle, L.S. Discrepancies between sources providing the medication histories of acutely hospitalised patients. Pharm World Sci 32, 449–454 (2010). https://doi.org/10.1007/s11096-010-9390-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11096-010-9390-0