
Abstract
Purpose
To determine the efficacious cefazolin prophylactic dose for bariatric surgery using free subcutaneous concentrations accessed by microdialysis after 2 g or 3 g i.v. bolus dosing to morbidly obese women and POPPK modeling.
Methods
A POPPK model with variable plasma and subcutaneous tissue protein binding was developed to simultaneously describe plasma and tissue data sets. The outcomes was predicted for common surgical site infection (SSI) bacteria over 3, 4, 5 and 6 h periods postdose, as probability of target attainment (PTA) using Monte Carlo simulation.
Results
CFZ 2 g warrant up to 5 h SSI prophylaxis for bacteria with MICs ≤1 mg/L such as Escherichia coli and Staphylococcus aureus. For species such as Klebsiella pneumoniae, which present MIC distribution frequency of 2 mg/L, the maintenance of PTA ≥ 90% occurs with a 3 g dose for surgeries lasting up to 5 h, and 2 g dose provide an adequate response up to 4 h (PTA of 89%).
Conclusions
Effectiveness of CFZ 2 g is similar to 3 g against bacteria with a MIC up to 2 mg/L, especially if the surgery does not last for more than 4 h.




Similar content being viewed by others

Abbreviations
- ASHP:
-
American society of health-system pharmacists
- AUCplasma,free :
-
Area under curve of unbound plasma concentration
- AUCplasma,total :
-
Area under curve of total plasma concentration
- AUCsubcutaneous,free :
-
Area under curve of unbound subcutaneous tissue concentration
- AUCsubcutaneous,total :
-
Area under curve of total subcutaneous tissue concentration
- Bmax(p) :
-
Maximal binding capacity of CFZ to plasma albumin
- Bmax(t) :
-
Maximal binding capacity of CFZ to tissue albumin
- BMI:
-
Body mass index
- CFZ:
-
Cefazolin
- CL:
-
Total body clearance
- Cplasma,total :
-
Total plasma cefazolin concentration
- DFtissue :
-
Tissue distribution factor
- dp:
-
Dilution factor of albumin concentration in interstitial space fluid
- fT > MIC:
-
Unbound tissue CFZ concentration above the minimum inhibitory concentration
- FuP:
-
Unbound plasma fraction
- FuT:
-
Unbound subcutaneous tissue fraction
- HNSC:
-
Nossa Senhora da Conceição Hospital
- HPLC:
-
High-performance liquid chromatography
- Kdp :
-
Dissociation constant for CFZ binding to plasma albumin
- Kdt :
-
Dissociation constant for CFZ binding to tissue albumin
- MIC:
-
Minimum inhibitory concentration
- NCA:
-
Non-compartmental pharmacokinetic analysis
- POPPK:
-
Populational pharmacokinetics
- PTA:
-
Probability of target attainment
- Q:
-
Inter-compartmental clearance
- SSI:
-
Surgical site infection
- V1:
-
Volume of distribution of the central compartment
- V2:
-
Volume of distribution of the subcutaneous tissue compartment
- VPC:
-
Visual predictive check
References
Flegal KM, Kruszon-Moran D, Carroll MD, Fryar CD, Ogden CL. Trends in obesity among adults in the United States, 2005 to 2014. Jama [Internet]. 2016;315(21):2284–91. Available from: https://doi.org/10.1001/jama.2016.6458
BRASIL. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância de Doenças e Agravos não Transmissíveis e Promoção da Saúde. Vigitel Brazil 2016: surveillance of risk and protective factors for chronic diseases by telephone survey: estimates of sociodemographic frequency and distribution of risk and protective factors for chronic diseases in the capitals of the 26 Brazilian sta [Internet]. Brasília: Ministério da Saúde; 2017. Available from: http://portalarquivos.saude.gov.br/images/pdf/2017/junho/07/vigitel_2016_jun17.pdf
De Oliveira ML, Santos LMP, Silvada EN. Direct healthcare cost of obesity in Brazil: an application of the cost-of-illness method from the perspective of the public health system in 2011. PLoS One. 2015;10(4):1–15.
Santos LMP, De Oliveira IV, Peters LR, Conde WL. Trends in morbid obesity and in bariatric surgeries covered by the Brazilian public health system. Obes Surg. 2010;20(7):943–8.
Maggard MA, Shugarman LR, Suttorp M, Maglione M, Sugerman HJ, Livingston EH, et al. Clinical guidelines meta-Analysis : surgical treatment of obesity. Clin Guidel. 2005;142(7):547–59.
Colquitt JL, Pickett K, Loveman E, Frampton GK. Surgery for weight loss in adults (review). Cochrane Database Syst Rev. 2014;8(8):1–241.
Johnson EE, Simpson AN, Harvey JB, Simpson KN. Bariatric surgery implementation trends in the USA from 2002 to. Implement Sci [Internet]. 2012;2016:1–9. Available from: https://doi.org/10.1186/s13012-016-0382-x
Winfield RD, Reese S, Bochicchio K, Mazuski JE, Obesity BGV. The risk for surgical site infection in abdominal surgery. Am Surg. 2016;82(4):331–6.
Topaloglu S, Avsar FM, Ozel H, Babacan M, Berkem H, Yildiz Y, et al. Comparison of bariatric and non-bariatric elective operations in morbidly obese patients on the basis of wound infection. Obes Surg. 2005;15(9):1271–6.
Bratzler DW, Dellinger EP, Olsen KM, Perl TM, Auwaerter PG, Bolon MK, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am J Heal Pharm. 2013;70(3):195–283.
Brill MJE, Houwink API, Schmidt S, Van dongen EPA, Hazebroek EJ, Van ramshorst B, et al. Reduced subcutaneous tissue distribution of cefazolin in morbidly obese versus non-obese patients determined using clinical microdialysis. J Antimicrob Chemother. 2014;69(3):715–23.
Edmiston CE, Krepel C, Kelly H, Larson J, Andris D, Hennen C, et al. Perioperative antibiotic prophylaxis in the gastric bypass patient: do we achieve therapeutic levels? Surgery. 2004;136(4):738–47.
Anlicoara R, Ferraz ÁAB, Da P, Coelho K, De Lima Filho JL, Siqueira LT, et al. Antibiotic prophylaxis in bariatric surgery with continuous infusion of cefazolin: determination of concentration in adipose tissue. Obes Surg. 2014;24(9):1487–91.
Fischer MI, Dias C, Tetelbom Stein A, Guardiola Meinhardt N, Heineck I. Antibiotic prophylaxis in obese patients submitted to bariatric surgery. A systematic review. Acta Cir Bras. 2014;29(3):209–17.
Chen X, Brathwaite CEM, Barkan A, Hall K, Chu G, Cherasard P, et al. Optimal cefazolin prophylactic dosing for bariatric Surgery : no need for higher doses or intraoperative Redosing. Obes Surg [Internet]. 2017;27(3):626–9. Available from: https://doi.org/10.1007/s11695-016-2331-9
van Kralingen S, Taks M, Diepstraten J, Van De Garde EM, Van Dongen EP, Wiezer MJ, et al. Pharmacokinetics and protein binding of cefazolin in morbidly obese patients. Eur J Clin Pharmacol. 2011;67(10):985–92.
Alves IA, Staudt KJ, Silva C de M, Lock G de A, Costa TD, Verlindo B, et al. Influence of experimental Cryptococcal meningitis in Wistar rats on Voriconazole brain penetration assessed by Microdialysis. Antimicrob Agents Chemother 2017;61(7).
Palma EC, Araújo BV de, Laureano JV, Meinhardt NG, Stein AT, Dalla Costa T. Fast and sensitive HPLC/UV method for cefazolin quantification in plasma and subcutaneous tissue microdialysate of humans and rodents applied to pharmacokinetic studies in obese individuals. Biomed Chromatogr. 2018. (Under revision).
Moine P, Fish DN. Pharmacodynamic modelling of intravenous antibiotic prophylaxis in elective colorectal surgery. Int J Antimicrob Agents [Internet]. 2013;41(2):167–73. Available from: https://doi.org/10.1016/j.ijantimicag.2012.09.017
The European Committee on Antimicrobial Susceptibility Testing - EUCAST 2017. EUCAST MIC distributions [Internet]. MIC distributions and ECOFFs. 2013 [cited 2017 Mar 1]. Available from: http://www.eucast.org/mic_distributions/
De Cock RFW, Smits A, Allegaert K, de Hoon J, Saegeman V, Danhof M, et al. Population pharmacokinetic modelling of total and unbound cefazolin plasma concentrations as a guide for dosing in preterm and term neonates. J Antimicrob Chemother. 2014;69(5):1330–8.
Berezhkovskiy LM. On the Accuracy of Determination of Unbound Drug Fraction in Tissue Using Diluted Tissue Homogenate. 2012;101(5):1909–1916.
Berezhkovskiy LM. On the Accuracy of Estimation of Basic Pharmacokinetic Parameters by the Traditional Noncompartmental Equations and the Prediction of the Steady-State Volume of Distribution in Obese Patients Based Upon Data Derived from Normal Subjects. J Pharm Sci [Internet]. 2011 [cited 2017 Mar 30];100(6):2482–97. Available from: http://www.sciencedirect.com/science/article/pii/S0022354915321079
Young OM, Shaik IH, Twedt R, Binstock A, Althouse AD, Venkataramanan R, et al. Pharmacokinetics of cefazolin prophylaxis in obese gravidae at time of cesarean delivery. Am J Obstet Gynecol 2015;213(4):541.e1–541541.e7.
Grupper M, Kuti JL, Swank ML, Maggio L, Hughes BL, Nicolau DP. Population pharmacokinetics of cefazolin in serum and adipose tissue from overweight and obese women undergoing cesarean delivery. J Clin Pharmacol. 2016;0(November):1–8.
Vella-Brincat JWA, Begg EJ, Kirkpatrick CMJ, Zhang M, Chambers ST, Gallagher K. Protein binding of cefazolin is saturable in vivo both between and within patients. Br J Clin Pharmacol. 2007;63(6):753–7.
Smits A, Roberts JA, Vella-Brincat JWA, Allegaert K. Cefazolin plasma protein binding in different human populations: more than cefazolin-albumin interaction. Int J Antimicrob Agents. 2014;43(2):199–200.
Tetsuya T, Norishige I, Kazunoru N, Akira T. Age-related change of cefazolin binding to rat serum proteins and its relation to the molar ratio of free fatty acid to serum albumin. Aust J Pharm. 1986;9:81–7.
Tsuji A, Yoshikawa T, Nishide K, Minami H, Kimura M, Nakashima E, et al. Physiologically based pharmacokinetic model for β-lactam antibiotics I: tissue distribution and Elimanation rates. J Pharm Sci [Internet]. 1983;72(11):1239–52. Available from: http://linkinghub.elsevier.com/retrieve/pii/S0022354915448543
Housman ST, Sutherland CA, Nicolau DP. Pharmacodynamic profile of commonly utilised parenteral therapies against meticillin-susceptible and meticillin-resistant Staphylococcus aureus collected from US hospitals. Int J Antimicrob Agents [Internet]. 2014;44(3):235–41. Available from: https://doi.org/10.1016/j.ijantimicag.2014.05.012
Ho VP, Nicolau DP, Dakin GF, Pomp A, Rich BS, Towe CW, et al. Cefazolin dosing for surgical prophylaxis in morbidly obese patients. Surg Infect. 2012;13(1):33–7.
Peppard WJ, Eberle DG, Kugler NW, Mabrey DM, Weigelt JA. Association between pre-operative cefazolin dose and surgical site infection in obese patients. Surg Infect (Larchmt) [Internet]. 2016;18(0):1–6. Available from: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=medp&NEWS=N&AN=27906601
Allegranzi B, Zayed B, Bischoff P, Kubilay NZ, de Jonge S, de Vries F, et al. New WHO recommendations on intraoperative and postoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis [Internet]. 2016;16(12):e288–303. Available from: https://doi.org/10.1016/S1473-3099(16)30402-9
Allegranzi B, Bischoff P, de Jonge S, Kubilay NZ, Zayed B, Gomes SM, et al. New WHO recommendations on preoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis [Internet]. 2016;16(12):e276–87. Available from: https://doi.org/10.1016/S1473-3099(16)30398-X
Funding
This work was supported by the PPSUS/FAPERGS, Rio Grande do Sul, Brazil [#1298–255/13–8].
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of Interest
The authors declare that they have no conflict of interest.
Electronic Supplementary Material
Supplementary Figure S1
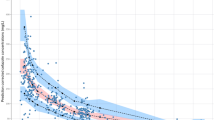
Individual and population fitted total (upper panel), free plasma (middle panel) and free subcutaneous tissue (lower panel) profiles using nonlinear mixed-effect modeling approach. Patients received a single 2 g (1–4) or 3 g (5–6) intravenous bolus dose of CFZ. Black dots: observations; solid line: individual model predictions; dashed line: population model. (GIF 54 kb)
Rights and permissions
About this article

Cite this article
Palma, E.C., Meinhardt, N.G., Stein, A.T. et al. Efficacious Cefazolin Prophylactic Dose for Morbidly Obese Women Undergoing Bariatric Surgery Based on Evidence from Subcutaneous Microdialysis and Populational Pharmacokinetic Modeling. Pharm Res 35, 116 (2018). https://doi.org/10.1007/s11095-018-2394-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11095-018-2394-5