
Abstract
Purpose
To compare titer reduction and delivery rate of active anti-tuberculosis bacteriophage (phage) D29 with three inhalation devices.
Methods
Phage D29 lysate was amplified to a titer of 11.8 ± 0.3 log10(pfu/mL) and diluted 1:100 in isotonic saline. Filters captured the aerosolized saline D29 preparation emitted from three types of inhalation devices: 1) vibrating mesh nebulizer; 2) jet nebulizer; 3) soft mist inhaler. Full-plate plaque assays, performed in triplicate at multiple dilution levels with the surrogate host Mycobacterium smegmatis, were used to quantify phage titer.
Results
Respective titer reductions for the vibrating mesh nebulizer, jet nebulizer, and soft mist inhaler were 0.4 ± 0.1, 3.7 ± 0.1, and 0.6 ± 0.3 log10(pfu/mL). Active phage delivery rate was significantly greater (p < 0.01) for the vibrating mesh nebulizer (3.3x108 ± 0.8x108 pfu/min) than for the jet nebulizer (5.4x104 ± 1.3x104 pfu/min). The soft mist inhaler delivered 4.6x106 ± 2.0x106 pfu per 11.6 ± 1.6 μL ex-actuator dose.
Conclusions
Delivering active phage requires a prudent choice of inhalation device. The jet nebulizer was not a good choice for aerosolizing phage D29 under the tested conditions, due to substantial titer reduction likely occurring during droplet production. The vibrating mesh nebulizer is recommended for animal inhalation studies requiring large amounts of D29 aerosol, whereas the soft mist inhaler may be useful for self-administration of D29 aerosol.






Similar content being viewed by others

Abbreviations
- g:
-
Gravitational acceleration
- i:
-
Nebulization cycle count
- log10 :
-
Base 10 logarithm
- MDR-TB:
-
Multidrug-resistant tuberculosis
- MOI:
-
Multiplicity of infection
- n:
-
Number of plates
- pfu:
-
Plaque-forming unit
- Phage:
-
Bacteriophage
- TB:
-
Tuberculosis
- TEM:
-
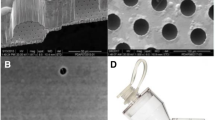
Transmission electron micrograph
- XDR-TB:
-
Extensively drug-resistant tuberculosis
References
Ventola CL. The antibiotic resistance crisis. Part 1: causes and threats. PT. 2015;40(4):277–83.
World Health Organization. Multidrug-resistant tuberculosis (MDR-TB): 2016 Update. 2016 Available from: http://www.who.int/tb/challenges/mdr/mdr_tb_factsheet.pdf . Accessed 21 Feb 2017.
Udwadia ZF, Amale RA, Ajbani KK, Rodrigues C. Totally drug-resistant tuberculosis in India. Clin Infect Dis. 2012;54(4):579–81.
World Health Organization. Drug-resistant TB: Totally drug-resistant TB FAQ. 2017 Available from: http://www.who.int/tb/areas-of-work/drug-resistant-tb/totally-drug-resistant-tb-faq/en/. Accessed 21 Feb 2017.
Abedon ST, Kuhl SJ, Blasdel BG, Kutter EM. Phage treatment of human infections. Bacteriophage. 2011;1(2):66–85.
Kutateladze M, Adamia R. Bacteriophages as potential new therapeutics to replace or supplement antibiotics. Trends Biotechnol. 2010;28(12):591–5.
Verbeken G, Huys I, Pirnay J-P, Jennes S, Chanishvili N, Scheres J, et al. Taking bacteriophage therapy seriously: a moral argument. Biomed Res Int. 2014;2014:621316.
Hatfull GF, Vehring R. Respirable bacteriophage aerosols for the prevention and treatment of tuberculosis. In: Hickey AJ, Misra A, Fourie PB, editors. Drug delivery systems for tuberculosis prevention and treatment. Chichester: John Wiley & Sons, Ltd.; 2016. p. 277–92.
Loc-Carrillo C, Abedon ST. Pros and cons of phage therapy. Bacteriophage. 2011;1(2):111–4.
Kutter E, Sulakvelidze A. Bacteriophages: biology and applications. Boca Raton: CRC Press; 2005.
Hoe S, Semler DD, Goudie AD, Lynch KH, Matinkhoo S, Finlay WH, et al. Respirable bacteriophages for the treatment of bacterial lung infections. J Aerosol Med Pulm Drug Deliv. 2013;26(6):317–35.
Kutter E, de Vos D, Gvasalia G, Alavidze Z, Gogokhia L, Kuhl S, et al. Phage therapy in clinical practice: treatment of human infections. Curr Pharm Biotechnol. 2010;11(1):69–86.
Hoe S, Boraey MA, Ivey JW, Finlay WH, Vehring R. Manufacturing and device options for the delivery of biotherapeutics. J Aerosol Med Pulm Drug Deliv. 2014;27(5):315–28.
Golshahi L, Seed KD, Dennis JJ, Finlay WH. Toward modern inhalational bacteriophage therapy: nebulization of bacteriophages of Burkholderia cepacia complex. J Aerosol Med Pulm Drug Deliv. 2008;21(4):351–60.
Matinkhoo S, Lynch KH, Dennis JJ, Finlay WH, Vehring R. Spray-dried respirable powders containing bacteriophages for the treatment of pulmonary infections. J Pharm Sci. 2011;100(12):5197–205.
Leung SY, Parumasivam T, Gao FG, Carrigy NB, Vehring R, Finlay WH, et al. Production of inhalation phage powders using spray freeze drying and spray drying techniques for treatment of respiratory infections. Pharm Res. 2016;33(6):1486–96.
Golshahi L, Lynch KH, Dennis JJ, Finlay WH. In vitro lung delivery of bacteriophages KS4-M and ɸKZ using dry powder inhalers for treatment of Burkholderia cepacia complex and Pseudomonas Aeruginosa infections in cystic fibrosis. J Appl Microbiol. 2011;110(1):106–17.
Parracho HMRT, Burrowes BH, Enright MC, McConville ML, Harper DR. The role of regulated clinical trials in the development of bacteriophage therapeutics. J Mol Genet Med. 2012;6:279–86.
Verbeken G, Pirnay J-P, de Vos D, Jennes S, Zizi M, Lavigne R, et al. Optimizing the European regulatory framework for sustainable bacteriophage therapy in human medicine. Arch Immunol Ther Exp. 2012;60(3):161–72.
Abedon ST. Phage therapy of pulmonary infections. Bacteriophage. 2015;5(1):1–13.
Semler DD, Goudie AD, Finlay WH, Dennis JJ. Aerosol phage therapy efficacy in Burkholderia cepacia complex respiratory infections. Antimicrob Agents Chemother. 2014;58(7):4005–13.
Liu K-Y, Yang W-H, Dong X-K, Cong L-M, Li N, Li Y, et al. Inhalation study of mycobacteriophage D29 aerosol for mice by endotracheal route and nose-only exposure. J Aerosol Med Pulm Drug Deliv. 2016;29(5):393–405.
Cooper CJ, Denyer SP, Maillard J-Y. Stability and purity of a bacteriophage cocktail preparation for nebulizer delivery. Lett Appl Microbiol. 2013;58(2):118–22.
Sahota JS, Smith CM, Radhakrishnan P, Winstanley C, Goderdzishvili M, Chanishvili N, et al. Bacteriophage delivery by nebulization and efficacy against phenotypically diverse Pseudomonas Aeruginosa from cystic fibrosis patients. J Aerosol Med Pulm Drug Deliv. 2015;28(5):353–60.
Froman S, Will DW, Bogen E. Bacteriophage active against virulent mycobacterium tuberculosis I. Isolation and activity. Am J Public Health Nations Health. 1954;44(10):1326–33.
phagesDB.org. Phage hunting procedure & protocols. 2016 December 2. Available from: phagesdb.org/workflow/.
Engel M, Heinrichs S. Use of tiotropium salts in the treatment of moderate persistent asthma. 2015. Patent US 20150224090 A1.
Dalby R, Spallek M, Voshaar T. A review of the development of Respimat soft mist inhaler. Int J Pharm. 2004;283(1–2):1–9.
Dalby R, Eicher J, Zierenberg B. Development of Respimat® Soft Mist™ Inhaler and its clinical utility in respiratory disorders. Med Devices (Auckl). 2011;4:145–55.
Finlay WH. The mechanics of inhaled pharmaceutical aerosols: an introduction. San Diego: Academic Press; 2001.
Fink JB. New technology offers new opportunities: continuous bronchodilator therapy during mechanical ventilation. Available from: https://www.aerogen.com/uploads/Publications/Continuous%20Bronchodilator%20Therapy%20During%20Mechanical%20Ventilation%20Jim%20Fink.pdf. Accessed 22 Feb 2017.
May KR. The collison nebulizer: description, performance and application. J Aerosol Sci. 1973;4(3):235–43.
Lentz YK, Worden LR, Anchordoquy TJ, Lengsfeld CS. Effect of jet nebulization on DNA: identifying the dominant degradation mechanism and mitigation methods. J Aerosol Sci. 2005;36(8):973–90.
Liu K, Wen Z, Yang W, Wang J, Hu L, Dong X, et al. Impact of relative humidity and collection media on mycobacteriophage D29 aerosol. Appl Environ Microbiol. 2012;78(5):1466–72.
Arulmuthu ER, Williams DJ, Baldascini H, Versteeg HK, Hoare M. Studies on aerosol delivery of plasmid DNA using a mesh nebulizer. Biotechnol Bioeng. 2007;98(5):939–55.
Sidler-Moix A-L, Di Paolo ER, Dolci U, Berger-Gryllaki M, Cotting J, Pannatier A. Physicochemical aspects and efficiency of albuterol nebulization: comparison of three aerosol types in an in vitro pediatric model. Respir Care. 2015;60(1):38–46.
Fédération Antadir Commission Medico-Technique & Sociale. Fiche de synthese du dispositif: Pari Boy SX / Pari LC® Sprint SP. 2007 Available from: http://www.antadir.com/uploads/product/95/pdf/synthese-pari-lc-sprint-v4-inter.pdf. Accessed 12 May 2017.
Wachtel H, Ziegler J. Improved assessment of inhaler device performance using laser diffraction. Respiratory Drug Deliv VIII. 2002;2:379–81.
Carrigy NB, Martin AR, Finlay WH. Use of extrathoracic deposition models for patient-specific dose estimation during inhaler design. Curr Pharm Des. 2015;21(27):3984–92.
Vandal OH, Nathan CF, Ehrt S. Acid resistance in mycobacterium tuberculosis. J Bacteriol. 2009;191(15):4714–21.
Xiong X, Zhang HM, Wu TT, Xu L, Gan YL, Jiang LS, et al. Titer dynamic analysis of D29 within MTB-infected macrophages and effect on immune function of macrophages. Exp Lung Res. 2014;40(2):86–98.
Basra SK. The isolation and characterization of phages with lytic activity against Mycobacterium avium subspecies paratuberculosis, and their application using Bioluminescent assay in real-time Loop-mediated isothermal amplification assay for rapid detection. Master of Science Thesis. Department of Food Science, University of Guelph. 2013. Guelph, ON, Canada.
Darch SE, Kragh KN, Abbott EA, Bjarnsholt T, Bull JJ, Whiteley M. Phage inhibiting pathogen dissemination by targeting bacterial migrants in a chronic infected model. mBio. 2017;8(2):e00240–17.
Abedon ST. Bacteriophages and biofilms: ecology, phage therapy, plaques. New York: Nova Science Publishers, Inc.; 2011.
Drulis-Kawa Z, Majkowska-Skrobek G, Maciejewska B, Delattre A-S, Lavigne R. Learning from bacteriophages – advantages and limitations of phage and phage-encoded protein applications. Curr Protein Pept Sci. 2012;13(8):699–722.
Lu TK, Collins JJ. Dispersing biofilms with engineered enzymatic bacteriophage. PNAS. 2007;104(27):11197–202.
Kolodkin-Gal I, Romero D, Cao S, Clardy J, Kolter R, Losick R. D-amino acids trigger biofilm disassembly. Science. 2010;328(5978):627–9.
Nadithe V, Rahamatalla M, Finlay WH, Mercer JR, Samuel J. Evaluation of nose-only aerosol inhalation chamber and comparison of experimental results with mathematical simulation of aerosol deposition in mouse lungs. J Pharm Sci. 2003;92(5):1066–76.
Acknowledgments and Disclosures
NC gratefully thanks the Natural Sciences and Engineering Research Council of Canada, Alberta Innovates, and the University of Alberta for scholarship funding. This includes a Michael Smith Foreign Study Supplement and an Education Abroad Individual Award allowing him to perform research in Sydney, Australia. The authors thank Arlene Oatway for help with the transmission electron micrograph and Jim Fink for providing Aerogen nebulizers and equipment. This work was financially supported in part by the Australian Research Council (Discovery Project DP150103953).
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Appendix Notation
- C d , p , i :
-
mass concentration of solute in the solvent droplets both exiting the mouthpiece and returning to the reservoir in the i th nebulization cycle, assumed to be equal
- C e , p , i :
-
mass concentration of solute in the solvent droplets exiting the mouthpiece in the i th nebulization cycle
- C n , p , i :
-
mass concentration of solute in the solvent exiting the nozzle in the i th nebulization cycle
- C p :
-
mass concentration of solute in the solvent
- C p , 0 :
-
mass concentration of solute in the solvent initially input to the reservoir
- C r , p , i :
-
mass concentration of solute in the solvent droplets returning to the reservoir in the i th nebulization cycle
- Cu(f e , i ):
-
fraction of the initial number of phage input to the jet nebulizer which have cumulatively exited the mouthpiece over i nebulization cycles
- Cu(i*X i ):
-
average number of nebulization cycles phage which exited the mouthpiece underwent
- f e , i :
-
fraction of the number of phage initially input to the reservoir, which exit the mouthpiece in the i th nebulization cycle
- i :
-
nebulization cycle count
- j :
-
a summation index for i in Cu(f e , i )
- k :
-
a summation index for i in X i
- L :
-
a summation index for i in Cu(i ∗ X i )
- \( {\dot{m}}_{e, s} \) :
-
mass flow rate of solvent in droplets exiting the mouthpiece
- \( {\dot{m}}_{h, s} \) :
-
mass flow rate of solvent exiting due to humidification of air supplied by the compressor
- \( {\dot{m}}_{n, s} \) :
-
mass flow rate of solvent exiting the nozzle
- \( {\dot{m}}_p \) :
-
mass flow rate of solute
- \( {\dot{m}}_{r, s} \) :
-
mass flow rate of solvent returning to the reservoir
- \( {\dot{m}}_s \) :
-
mass flow rate of solvent
- m 1p :
-
mass of a single phage
- N :
-
total number of nebulization cycles to complete aerosolization
- n e , p , i :
-
number of phage, either active or inactive, exiting the mouthpiece in the i th nebulization cycle
- n p , 0 :
-
number of phage initially input to the reservoir
- ρ s :
-
mass density of the solvent
- Q e , s :
-
volumetric flow rate of solvent in droplets exiting the mouthpiece
- Q h , s :
-
volumetric flow rate of solvent exiting due to humidification of air supplied by the compressor
- Q n , s :
-
volumetric flow rate of solvent exiting the nozzle
- Q r , s :
-
volumetric flow rate of solvent returning to the reservoir
- Q s :
-
volumetric flow rate of solvent
- t i :
-
time to complete the i th nebulization cycle
- V e , s , i :
-
volume of solvent in droplets exiting the mouthpiece in the i th nebulization cycle
- V F :
-
volume of solvent initially input to the reservoir, termed fill volume
- V h , s , i :
-
equivalent liquid volume of solvent exiting the device due to humidification of air supplied by the compressor in the i th nebulization cycle
- V n , s , i :
-
volume of solvent exiting the nozzle in the i th nebulization cycle
- V r , s , i :
-
volume of solvent returning to the reservoir in the i th nebulization cycle
- X i :
-
fraction of the cumulative number of phage which have exited the mouthpiece after aerosolization is complete, which exited the mouthpiece in the i th nebulization cycle
Nebulization Cycle Count Mathematical Model
A mathematical model was developed to estimate the average number of times that phage exited the nozzle and impacted the primary baffle of the jet nebulizer prior to exiting the mouthpiece.
The solvent, water in this study, can follow three paths after exiting the nozzle: 1) humidify the air supplied by the compressor and exit the nebulizer as vapor; 2) exit the mouthpiece as aerosol droplets; 3) impact the interior of the device and return (drip back) to the reservoir. By assuming no mixing between the reservoir fluid and returning fluid in the same nebulization cycle, conservation of mass for the solvent gives
where \( {\dot{m}}_{n, s} \) is the mass flow rate of the solvent exiting the nozzle, \( {\dot{m}}_{h, s} \) is the mass flow rate of solvent which will exit the device via humidification of the air supplied by the compressor, \( {\dot{m}}_{e, s} \) is the mass flow rate of solvent which will exit the mouthpiece of the device as aerosol droplets, and \( {\dot{m}}_{r, s} \) is the mass flow rate of solvent which will return to the reservoir to exit the nozzle in the next nebulization cycle.
The solvent mass flow rate is related to volumetric flow rate by
For water, ρ s can be considered constant during jet nebulization. Eq. (1) can thus be rewritten in terms of flow rates:
The flow rate exiting the nozzle, Q n , s , was determined experimentally using Tryptophan tracer assay, to be 17.64 mL/min. The flow rate exiting the mouthpiece of the device, Q e , s , was determined to be 0.12 mL/min from the mass captured on the filter during phage experiments. The flow rate lost to humidification, Q h , s , was calculated as the difference in flow rate determined based on mass loss from the nebulizer and mass captured on the outlet filter during phage experiments, and found to be 0.06 mL/min. This matched the theoretical amount of water required to fully humidify the air supplied by the compressor. The flow rate returning to the reservoir, Q r , s , was thus calculated using Eq. (3), to be 17.46 mL/min.
It is assumed that solute does not exit the inhaler via humidification losses. Mass conservation for the solute (phage) is then given by
The solute concentration in the solvent, C p , is related to the mass flow rate by
Assuming the solute remains in the droplets and reservoir fluid, Eqs. (4) and (5) can be combined to give
It is assumed that the humidification of the air supplied by the compressor occurs by evaporation of the droplets exiting the nozzle, which have a high air-liquid surface area to volume ratio, rather than from the liquid in the reservoir. The humidification due to evaporation of the primary and secondary droplets increases the solute concentration in the droplets. Let us assume that the increase in concentration in the droplets that exit the mouthpiece and that return to the reservoir is equal. Then, we can define the droplet concentration, C d , p , as
With each nebulization cycle, i, the concentration of the solute in the reservoir will increase. The concentration of solute in the reservoir in a specific cycle, i, is the same as the concentration of solute in the droplets in the previous cycle, i − 1, as we have assumed no mixing between the reservoir fluid and returning fluid in the same cycle:
Let us define
where C p , 0 is the input mass concentration of solute in solvent. Here, C n , p , 1 represents the concentration of solute in solvent exiting the nozzle during the first nebulization cycle, when i = 1.
By combining Eqs. (6) and (7), and assuming that the respective volumetric flow rates are independent of nebulization cycle,
and rearranging Eq. (11) gives
The value of \( \frac{Q_{n, s}}{\left({Q}_{e, s}+{Q}_{r, s}\right)} \) is a constant, equal to 1.0034 in the present study. This value quantifies the increase in concentration of solute in the droplets emitted from the nozzle with each nebulization cycle, due to loss of solvent associated with humidification of the air supplied by the compressor.
When i = 1, using Eqs. (8), (9), and (11), one finds that
For i = 2, Eq. (12) gives
Combining Eqs. (13) and (14), one finds that
One can continue to show that in general
This equation demonstrates how the solute concentration in the droplets of a specific nebulization cycle, i, is related to the initial solute concentration in the reservoir.
In order to estimate the number of phage exiting the mouthpiece in a specific nebulization cycle, volumes are evaluated for each nebulization cycle. The volume returned to the nebulizer, V r , s , in a specific cycle is equal to the volume exiting the nozzle, V n , s , in the following cycle:
Eq. (17) is valid for i = 2 → N. For i = 1, the volume exiting the nozzle is assumed to be equal to the fill volume, V F :
The time for a nebulization cycle to complete, t i , is specified by
The following volumes can then be obtained using t i and the known flow rates:
where V h , s , i is the equivalent liquid volume exiting the device due to humification in a specific nebulization cycle, V e , s , i is the volume exiting the mouthpiece of the device as droplets in a specific nebulization cycle, and V r , s , i is the volume returned to the reservoir in a specific nebulization cycle.
The number of phage, either active or inactive, exiting the mouthpiece in a specific nebulization cycle, n e , p , i , can be found according to
where m 1p is the mass of a single phage.
Similarly, the number of phage initially in the reservoir is
The fraction of the number of phage initially input to the reservoir that has exited the mouthpiece in a specific nebulization cycle, f e , i , can therefore be found using Eqs. (16), (23), and (24), as
The fraction of the number of phage initially input to the reservoir that have cumulatively exited the mouthpiece of the device over i nebulization cycles, Cu(f e , i ), is given by
where j is a summation index. To solve Eq. (26), for example, when i = 3,
The curve in Figure 4 represents the solution to Eq. (26) for every i from i = 1 to i = N, where N represents the number of nebulization cycles when V r , s , i is equal to the residual volume of the nebulizer after aerosolization is complete, which was experimentally determined to be 0.5 mL during phage measurements in this study. The fraction was converted to a percentage in the plot.
Also given in Figure 4 is the average number of nebulization cycles phage that exited the mouthpiece underwent. To determine this value, one must consider that some phage are left in the residual volume of the nebulizer after aerosolization is complete.
The fraction of the cumulative number of phage that have exited the mouthpiece after N nebulization cycles, that exited the mouthpiece in the specific nebulization cycle i, is termed X i , and is given by:
where k is a summation index.
It can be shown that the average number of nebulization cycles phage underwent prior to exiting the mouthpiece of the jet nebulizer, Cu(i ∗ X i ), is given by
where L is a summation index.
The average number of nebulization cycles the phage underwent prior to exiting the mouthpiece of the jet nebulizer was thus determined to be 96 in the present study, with the final phage exiting the mouthpiece having undergone N=269 nebulization cycles. Assuming that every time a phage exits the nozzle it impacts the primary baffle, the nebulization cycle count i corresponds to the number of baffle impactions the phage underwent.
Other parameters such as total nebulization time and total volumes lost to humidification and exiting the mouthpiece can also be obtained using summations from 1 to N.
Rights and permissions
About this article

Cite this article
Carrigy, N.B., Chang, R.Y., Leung, S.S.Y. et al. Anti-Tuberculosis Bacteriophage D29 Delivery with a Vibrating Mesh Nebulizer, Jet Nebulizer, and Soft Mist Inhaler. Pharm Res 34, 2084–2096 (2017). https://doi.org/10.1007/s11095-017-2213-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11095-017-2213-4