
Abstract
The ventilators involved in mechanical ventilation are usually equipped with pneumatic sensor detecting patient’s own respiratory effort in order to assist spontaneous breathing. However, the interface of the mask with the patient promotes air leaks that affect the measurement of pneumatic variables and hence induces patient–ventilator asynchrony. In this paper we describe a new method and apparatus for continuous monitoring of the respiration based on the measurement of chest wall movements. The proposed solution uses a long-period fibre grating sensor attached to patient’s thorax and a simple and cost-effective monochromatic measurement scheme. On a set of healthy volunteers, we have established the linear correlation between the change in local torso curvature and the tidal volume during clinically relevant breathing patterns. The chest-wall movement measured by the grating advances with respect to the air-flow signal by about 200 ms, indicating the possibility to lead to more confidence triggering decision. The proposed scheme is non-invasive, simple, low-cost, and immune to air-leaks and drifts that are limiting factors in the currently standard pneumatic measurement techniques.
Similar content being viewed by others


1 Introduction
In medicine, mechanical ventilation represents a method to mechanically assist or replace spontaneous breathing when there is a noticeable discrepancy between the level of respiratory effort required to maintain proper gas exchange and the performance capacity of the respiratory system. Non-invasive ventilation (NIV) is a standard of care for treatment of acute and chronic respiratory failure of various etiologies, and is commonly used with pulmonary, neuromuscular and chest wall diseases, obstructive sleep apnea, and in postoperative care (Robert and Make 2010). NIV provides the ventilatory support through the patient’s upper airways by delivering the air via facemask or helmet. Thus the airways are left intact, which preserves the airway defence mechanisms, reduces patient discomfort, and avoids the complications caused by intubation (Mehta and Hill 2001; Baudouin 2002).
Mechanical ventilators are usually equipped with a pneumatic (flow, pressure or volume) sensor for detecting the patient’s own respiratory effort, the signals of which are used to control the volume and timing of the air pumped in and out. However, the interface of the mask with the patient promotes air leaks that affect the measurement of pneumatic variables and hence induces patient–ventilator asynchrony. Non-optimal patient–ventilator interaction may occur in up to 25 % of patients, causing discomfort, higher use of sedation, development of delirium, ventilator-induced lung injury, prolonged mechanical ventilation, reduction of patient tolerance to NIV, and ultimately contribute to increased mortality (Verbrugghe and Jorens 2011; Epstein 2011).
The patient–ventilator asynchrony may be divided into a flow and timing asynchrony (Verbrugghe and Jorens 2011). The flow asynchrony can occur when the inspiratory flow rate or the amplitude is insufficient to meet the patient’s ventilatory demand. Therefore, continuous monitoring of respiratory volumes is necessary. Due to the errors in the flow or volume measurement, regular monitoring by a clinician is required. As this is time consuming, costly and subjective (Mehta and Hill 2001; Baudouin 2002), there is a need for more accurate flow and volume monitoring. Most devices constructed for this purpose [respiratory inductance plethysmography (Watson 1980), transthoracic impedance pneumography (Drummond et al. 1996), fiber-optic respiratory plethysmography (Davis et al. 1997), optoelectronic plethysmography (Aliverti 2000) and plethysmography based on LPG sensors (Allsop 2007)] have been based on the discovery of Konno and Mead who have shown the correlation between the volume of the inhaled air and thoracic and abdominal movements caused by breathing (Konno and Mead 1967). However, each of the proposed devices has a disadvantage that has prevented its use in clinical practice (Petrovic 2014).
The timing asynchrony refers to a mismatch between the patient and ventilator respiratory cycles. The dominant source of most common asynchronies (the failure to trigger the ventilator, auto-triggering without patient’s effort, delayed triggering, premature cycle or a prolonged cycling (Epstein 2011)) is the delay with which the respiratory effort is detected. Theoretically, the delay of initiation of inspiratory flow with respect to the neural activity detectable invasively by neurally adjusted ventilatory assist (NAVA) is about 20 ms in healthy individuals (Verbrugghe and Jorens 2011). However, due to the time that air takes to flow to/from the mask, triggering delays of mechanical ventilators applied to patients reach 250–550 ms (Spahija 2010).
In this paper we describe a new method and apparatus for continuous monitoring of the respiration during NIV, based on the measurement of chest-wall movements. The proposed solution uses a long-period fibre grating (LPG) sensor attached to the patient’s thorax and a simple and cost-effective monochromatic measurement scheme. We test the hypothesis that the volume of the inhaled air is proportional to the change in a local torso curvature in an area with stiff underlying tissues and investigate a possibility to use outward/inward movements of the torso as a more confident trigger compared to commonly used pneumatic trigger.
The paper is structured as follows. Section 2 describes the working principle of LPG sensors and the monochromatic interrogation scheme for recording LPG signals. The measurement protocol for respiratory volume measurement and results obtained on a set of 18 healthy volunteers are shown in Sect. 3. These results provide a proof of the linear correlation between chest wall movement and change in tidal volume. Section 4 describes the determination of the time relationship between the signals generated by the chest movement and air-flow. The results that show about 200 ms latency of the air-flow signal with respect to the torso curvature signal are also presented therein. Conclusions and directions of future work are given in Sect. 5.
2 Methods
2.1 LPG curvature sensor
The curvature sensor utilize a long-period fiber grating (LPG) as a sensing element. The LPG consists of a periodic perturbation of the optical fibre properties, commonly of the refractive index of the core. These gratings have a period of several hundred microns which enables coupling of the light from the fundamental core mode to the lossy co-propagating cladding modes. The resulting transmission spectrum consists of a series of attenuation bands centered at distinct wavelengths. Each attenuation band corresponds to a different cladding mode and is characterized by a resonant wavelength \(\lambda\) given by the phase-matching condition
where \(n^{eff}_{co}\) is the effective index of the core mode, \(^{\nu }n^{eff}_{cl}\) the effective index of the \(\nu\)th cladding mode, and \(\varLambda\) the grating period. The magnitude of an attenuation band depends on the grating length and mode-coupling strength, while its width depends also on the fibre and the grating dispersion (Erdogan 1997; Kashyap 2010). Both the resonant wavelength and spectral profile of the attenuation band are sensitive to the force applied to the fiber (strain, bending, load) and the changes in the local environmental conditions (temperature, refractive index of surrounding material; James and Tatam 2003; Othonos and Kalli 1999).
Changes in the thorax curvature during breathing are sensed as bending of an LPG sensor attached to the subject’s thorax. Bending modifies the density across the fiber, which causes a change in refractive index profile of the fiber via strain-optic effect. The bend-induced index change directly influences the propagation of the modes, in particular cladding modes who sense the refractive index change along the entire fiber cross section. Spectrum alternation due to the bending can be observed as changes in position, shape and amplitude of the attenuation band in transmission spectrum (James and Tatam 2003).
Special care was taken to solve the problem of the cross-sensitivity to other parameters. The grating cross-sensitivity to the refractive index of surrounding material has been avoided by fabricating LPG in progressive three-layered fibre whose second cladding served as an isolator (Allsop et al. 2003).
2.2 Measurement scheme
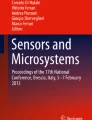
The full grating characterization can be obtained by using broadband light source and optical spectrum analyzer (OSA). Whereas convenient in laboratory, this approach is impractical for clinical measurements due to the high cost and low data rate of OSA. Instead, we use a simple monochromatic interrogation scheme that relies on the transmitted power measurement by a photodiode (Fig. 1a). As a source, we employ a fiber-coupled narrowband temperature- and current-stabilized DFB laser diode with a central wavelength 1470.73 nm and a tuning range of 5 nm (Petrovic 2014; Petrovic et al. 2013). The thorax motion is detected using the lateral filtering interrogation technique. It employs measurement of the change in power transmitted through the LPG sensor at specified wavelength (green vertical line in the inset of Fig. 1b) caused by the spectral shift due to the bending of the fibre. As the measurements described here last a few minutes at their maximum, the drift of the baseline power of around 100 ml/min (less than 15 ml/breath) on average, is negligible and a reference signal is not needed.

a Sensing scheme b Power sensitivity of the LPG to bending measured by the interrogator. The working region is shadowed. Inset Spectral sensitivity of the LPG to bending measured by OSA (Agilent 86142b)
For the grating characterization we used a specially designed three-point gauge (Petrovic 2013). The sensitivity (the smallest change in curvature that the sensor can detect) was 0.02 m\(^{-1}\). Since we measure the curvature changes around a preset curvature, we want to position the working point (WP) so that the sensor characteristic around it is monotonic and, if possible, linear in the whole breathing range (Fig 1b). To achieve this, we tune the grating into the resonance with the laser by judicious positioning of the sensor on a subject’s thorax.
3 Respiratory volume measurements
3.1 Measurement protocol and data analysis
The study protocol was approved by ethics committee of the Vinca Institute of Nuclear Sciences, University of Belgrade. The 18 healthy volunteers (9 females and 9 males), aged between 25 and 51 years (\(33 \pm 8\) years), and with BMI ranging from 18.4 to 39.2 kg/m\(^2\) (\(24 \pm 5\) kg/m\(^2\)) were involved in the measurements (Petrovic 2014).
During all measurements the subjects were in supine position. The sensor (encapsulated in 8 cm long silicon rubber) was placed on the surface in the zone of ribs 7–9 with the stiff underlying tissues on the right side of thorax. The right side of the rib cage was selected in order to reduce the impact of the heart beat on the signal. Sensor was fixed by an elastic bandage that goes around subject’s thorax and over the sensor.
The measurement protocol consists of two steps, calibration and test measurements. As a reference instrument we used spirometer (SpiroTube, Thor Medical, Budapest). After eliminating the spirometer drift, the calibration function was calculated by fitting with polynomials of different orders. Finally, the linear scaling was chosen as optimal regarding robustness and accuracy. The calibration function was used for calculation of the respiratory volumes in all test measurements performed on the same subject under the same conditions. For the test measurements, subjects were asked to perform 1 min of natural and 1 min of shallow breathing (approximately half the tidal volume of natural breathing). These two types of breathing are clinically most significant since the patients on mechanical ventilation are breathing with lower tidal volumes and as their condition improves the tidal volume approaches its natural value. We defined three parameters for the performance metric: the uncertainty \(\Delta\) (radius of the region around the calibration curve that contains 68 % of all measured values), the mean tidal volume error (mean relative error of tidal volumes over a number of respiratory cycles) and the minute volume error (relative error of the minute volumes; Petrovic 2014).
3.2 Results and discussion
All data are expressed as (mean ± SD), i.e. as the mean and the standard deviation of a set.

a, b Scatter plot (dots) and the calibration function (inner line) and \(\Delta\) region (outer lines) in calibration and test step, respectively, c calibrated sensor output, d tidal volume extracted from c
Figure 2 shows a set of the calibration and test results. Although the statistics was calculated for the clinically relevant natural and shallow breathing only, here we chose to show the test performed as a combination of deep, natural and shallow breathing in order to demonstrate the sensors ability to follow transitions between different types of breathing. Scatter plots (a) and (b) show linear correlation between the change of the local torso curvature and change in tidal volume measured by spirometer. A linear correlation was observed in each subject. The calibration uncertainty \(\Delta _{calib}\) of the whole statistical group (\(7.0\, \pm \,2.2\)) % and the test uncertainty \(\Delta _{test}\) of (\(7.8 \,\pm \,2.4\)) % for natural and (\(11.3 \,\pm \,2.8\)) % for shallow breathing validate the linear fit (Petrovic 2014). The coefficient of proportionality, i.e. the slope of a regression line in the scatter plot, was patient dependent.
Comparison of the volumes calculated by a calibrated sensor and volumes measured by the spirometer in the test phase gives the mean minute volume error on the whole set of (\(8.7 \,\pm \,4.4\)) % for natural breathing and (\(10.1 \,\pm \,5.8\)) % for shallow breathing (Petrovic 2014). The obtained results indicate that the LPG curvature sensors could be used in NIV since the accuracy to within 10 % represent the acceptable level for clinical use (Wechowski et al. 1990).
The mean tidal volume error on the whole group was (\(10.5 \pm 3.8\)) % for natural breathing and (\(15.0 \pm 4.8\)) % for shallow breathing (Petrovic 2014). The accuracy of the tidal volume measurement was limited by the unwanted detection of the heart beat signal to 60 ml, which is good enough for clinical utilization in NIV.
When compared to other measurement methods based on the discovery of Konno and Mead, the proposed method for respiratory volume monitoring by using a single LPG curvature sensor is simpler, easier to implement and less susceptible to signal distortion. Additionally, it does not require subject cooperation for calibration, does not suffer from large baseline drift, and exhibits good calibration and/or measurement accuracy for clinical use (Petrovic 2014). Its main disadvantage is a necessity for recalibration after a change in position or posture due to the displacement of the previously found WP and susceptibility to the body movements not originating from respiration. This can be largely corrected by automatic finding of the sensor WP (by tuning the laser into the resonance with the grating) and its correction upon the movement of the subject, advanced signal postprocessing and better sensor fixation to the body.
4 Measurement of the latency time between chest wall motion and flow signal
4.1 Measurement protocol and data analysis
The study protocol was approved by ethics committee of the School of Medicine, University of Belgrade, and the University Clinical Hospital Center Zemun where the study was carried out. The 25 healthy volunteers (12 females and 13 males), aged between 19 and 62 years (\(38 \pm 12\) years), and with BMI ranging from 18.5 to 29.1 kg/m\(^2\) (\(23.8 \pm 2.8\) kg/m\(^2\)) participated in the study (Ivanovic et al. 2015). Again during all the measurements the subjects were in supine position and the sensor was placed on the thorax stiff area and fixed by an elastic bandage as in the previously described study of respiratory volumes.
In this study the key task was to determine the time delay between the volume signals measured by the LPG sensor and pneumotachograph built into a mechanical ventilator Hamilton C3 (Part no. 155362), as a reference metric. The pneumotachograph was placed as normal in a tube extension of an oronasal mask and connected to the ventilator. To secure that the chest wall movements of the subjects will be conducted only by their efforts, in all our measurements the ventilator was not set in any of its modes and the inspiratory and expiratory tubes of the ventilator were not connected to the subjects. The synchronization of the signals from pneumotachograph and LPG sensor was provided by directly leading the analogue electronic signals from these two sensors to the same external analogue-to-digital converter (NI USB6008). In that manner we avoided delays that may occur due to the electronic data processing by the ventilator software. Both signals were sampled with the frequency of 100 Hz, thus limiting the delay-measurement sensitivity to 10 ms (Ivanovic et al. 2015; Ivanovic 2014).
Subjects were asked to breathe naturally for 100 s and three sets of measurements were recorded on each subject. The volume signal from the pneumotachograph was calculated by integrating the flow signal. The LPG volume signal was obtained by the calibration procedure described in the previous section. The drift was eliminated in both signals by setting the minima of all respiratory cycles to zero.
4.2 Results and discussion
A typical example of delayed metrics performed on one signal is depicted in Fig. 3 in which the sensor signal was calibrated by a scaling factor. We have decided to use one relative (10 %) and one absolute measure (100 ml) since the absolute measure is dependent on the goodness of the curvature-to-volume calibration. The cross-correlation on the whole signal was used to gain an insight which phenomenon (torso movement or air flow) occurs first. Obviously, the cross-correlation cannot discriminate between asynchrony caused by triggering or cycling, hence it cannot be used for triggering.

An example of delay metric on one pair of signals with marked 10 % thresholds in inspiratory phase
The results obtained on the whole set are shown in Table 1. The latency is expressed as delay of the LPG with respect to the pneumotachograph signal. The results show that the curvature signal registered by the LPG sensor precedes the volume signal measured by pneumotachograph by more than 200 ms on average with a large standard deviation of nearly 100 %. We suppose that the large deviation around the mean values observed in all defined measures is due to a large variation in the torso movement in different people during breathing and the errors induced by the heart beat registered in the LPG signal. Similarity of results obtained for inspiratory and expiratory phases shows that torso movements precede the airway flow signal during the whole cycle. This conclusion is logical since the torso movements are further upstream the neuro-ventilatory control sequence (Verbrugghe and Jorens 2011). In the analyzed group we have only one non-responder in which LPG signal had a positive delay. This person has BMI of 18.5 kg/m\(^2\) (smallest BMI in the group) and a pronounced heart-beat signal.
The most accurate breath triggering can be achieved by NAVA, which captures the electrical activity of the diaphragm by using a special catheter placed into the patient’s esophagus (Spahija 2010; Cordioli et al. 2013; Navalesi 2012; Verbrugghe and Jorens 2011). However, the invasiveness of NAVA technology (draining gastric content, placing gastric catheter, etc.) is a significant drawback that prevents its use in a number of cases. The solution offered here has the delays between NAVA and air-flow sensors and the advantages of being non-invasive and immune to leaks, which puts it forward as a good candidate for an improved respiratory monitoring during mechanical ventilation. A further comprehensive clinical study on patients during NIV is required to precisely determine limitations of the proposed method.
5 Conclusion
We have investigated the possibility to use a single LPG curvature sensor attached to the subject’s thorax for respiration monitoring. On a set of healthy volunteers, we have established the linear correlation between the change in local torso curvature and the tidal volume during clinically relevant breathing patterns. Statistical analysis of the volume signals shows that the chest-wall movement measured by the LPG advances with respect to the air-flow signal by about 200 ms, indicating that the LPG scheme may lead to more confidence triggering decision. The proposed scheme is non-invasive, simple, low-cost, and immune to air-leaks and drifts that are limiting factors in the currently standard air-flow measurement techniques. The major source of errors in the proposed scheme is its sensitivity to the body movements not associated with breathing, including the heart beat. Future work will be directed towards elimination of these errors.
References
Aliverti, A., et al.: Optoelectronic plethysmography in intensive care patients. Am. J. Respir. Crit. Care Med. 161(5), 1546–1552 (2000)
Allsop, T., Webb, D.J., Bennion, I.: Investigations of the spectral sensitivity of long period gratings fabricated in 3-layered optical fiber. J. Lightwave Technol. 21, 264–268 (2003)
Allsop, T., et al.: Application of long-period-grating sensors to respiratory plethysmography. J. Biomed. Opt. 12(6), 064003 (2007)
Baudouin, S., et al.: British Thoracic Society Standards of Care Committee: non-invasive ventilation in acute respiratory failure. Thorax 57(3), 192–211 (2002)
Cordioli, R.L., Akoumianaki, E., Brochard, L.: Nonconventional ventilation techniques. Curr. Opin. Crit. Care 19(1), 31–37 (2013)
Davis, C., Mazzolini, A., Murphy, D.: A new fibre optic sensor for respiratory monitoring. Australas. Phys. Eng. Sci. Med. 20(4), 214–219 (1997)
Drummond, G.B., Nimmo, A.F., Elton, R.A.: Thoracic impedance used for measuring chest wall movement in postoperative patients. Br. J. Anaesth. 77(3), 327–332 (1996)
Epstein, S.K.: How often does patient–ventilator asynchrony occur and what are the consequences? Respir. Care 56(1), 25–38 (2011)
Erdogan, T.: Cladding-mode resonances in short- and long-period fiber grating filters. J. Opt. Soc. Am. A 14, 1760–1773 (1997)
Ivanovic, M., et al.: Rib-Cage-movement measurements as a potential new trigger signal in non-invasive mechanical ventilation. In: Conf. Proc. IEEE Eng. Med. Biol. Soc. 2015, Milan, Italy, pp. 4511–4514 (2015)
Ivanovic, M.: An optical fiber-grating device for measuring cardiovascular and respiratory pulsations, PhD thesis, University of Belgrade (2014)
James, S.W., Tatam, R.P.: Optical fibre long-period grating sensors: characteristics and application. Meas. Sci. Technol. 14, R49–R61 (2003)
Kashyap, R.: Fiber bragg gratings. Academic Press, Elsevier, Burlington, MA (2010)
Konno, K., Mead, J.: Measurement of the separate volume changes of rib cage and abdomen during breathing. J. Appl. Physiol. 22(3), 407–422 (1967)
Mehta, S., Hill, N.S.: Noninvasive ventilation. Am. J. Respir. Crit. Care Med. 163(2), 540–577 (2001)
Navalesi, P., et al.: Neurally adjusted ventilatory assist. In: Ferrer, M., Pelosi, P. (eds.) 8th Chapter in New Developments in Mechanical Ventilation. Eur. Respir. Mon. vol. 55, pp. 116–123 (2012)
Othonos, A., Kalli, K.: Fibre Bragg Gratings: Fundamentals and Applications in Telecommunications and Sensing. Artech House, Boston (1999)
Petrovic, M., et al.: A new method for respiratory-volume monitoring based on long-period fibre gratings. In: Conf. Proc. IEEE Eng. Med. Biol. Soc. 2013, Osaka, Japan, pp. 2660–2663 (2013)
Petrovic, M.D., et al.: Fibre-grating sensors for the measurement of physiological pulsations. Phys. Scr. T157, 014022 (2013)
Petrovic, M.D., et al.: Non-invasive respiratory monitoring using long-period fiber grating sensors. Biomed. Opt. Express 5(4), 1136–1144 (2014)
Robert, D., Make, B.: Non-invasive ventilation: from the past to the present. In: Elliott, M., Nava, S., Schnhofer, B. (eds.) Non-invasive Ventilation and Weaning: Principles and Practice. Hachette, UK (2010)
Spahija, J., et al.: Patient–ventilator interaction during pressure support ventilation and neurally adjusted ventilatory assist. Crit. Care Med. 38(2), 518–526 (2010)
Verbrugghe, W., Jorens, P.G.: Neurally adjusted ventilatory assist: a ventilation tool or a ventilation toy? Respir. Care 56(3), 327–335 (2011)
Watson, H.: The technology of respiratory inductance plethysmography. In: ISAM Proceedings of the 3rd International Symposium Ambulatory Monitoring, p. 537 (1980)
Wechowski, J.L., Sanders, M.H., Constantino, J.P., Sciurba, F.C., Rogers, R.M.: Inductance plethysmograph measurement of CPAP-induced changes in end-expiratory lung volume. J. Appl. Physiol. 68, 1732–1738 (1990)
Acknowledgments
We acknowledge financial support from the Ministry of Education, Science and Technological Development of Serbia (Project No. III45010) and thank colleagues from the Vinca Institute and the School of Medicine, University of Belgrade, Serbia and Aston Institute of Photonic Technologies, UK for collaboration and their contributions to this work.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Advances in the Science of Light.
Guest Edited by Jelena Radovanovic, Milutin Stepic, Mikhail Sumetsky, Mauro Pereira and Dragan Indjin.
Rights and permissions
About this article

Cite this article
Ivanovic, M.D., Petrovic, J. A long-period fibre grating monitor of respiratory volumes for the use in non-invasive mechanical ventilation. Opt Quant Electron 48, 346 (2016). https://doi.org/10.1007/s11082-016-0613-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11082-016-0613-z