
Abstract
Purpose
Motor mapping with direct cortical stimulation (DCS) is useful for motor function preservation. Nevertheless, many patients still experience postoperative motor dysfunction after motor mapping. This study aimed to provide a classification of gliomas involved in motor-related areas to help understand which types of gliomas are prone to induce postoperative motor impairments.
Methods
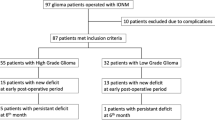
Sixty-four patients were retrospectively recruited. Based on tumor location, four types of gliomas were identified: (I) precentral gyrus; (II) premotor and/or supplementary motor areas but not invading pre-central gyrus; (III) adjacent to the posterior limb of the internal capsule; and (IV) other supra-tentorial area. The recovery of motor function was evaluated by muscle strength testing before surgery and 3 days, 7 days, 14 days, and 3 months after surgery.
Results
Half of the patients experienced postoperative transient motor impairment within a week. Six patients suffered from permanent motor dysfunction, and four of them had type III glioma. Compared with types I and IV, patients with type III gliomas took more than three times as long to recover. Furthermore, patients with types I and II gliomas were more susceptible to preoperative epilepsy than those with types III and IV. There was no difference in postoperative seizure control between the four types.
Conclusions
Our classification of gliomas involving motor-related eloquent areas was useful for predicting postoperative motor functional prognosis in patients who underwent motor mapping with DCS. Even if no positive sites were detected, a conservative strategy of tumor resection is recommended in cases that gliomas located close to the posterior limb of the internal capsule.




Similar content being viewed by others
Data availability
Anonymized data will be available on request.
References
Ostrom QT, Gittleman H, Liao P, Vecchione-Koval T, Wolinsky Y, Kruchko C, Barnholtz-Sloan JS (2017) CBTRUS Statistical Report: primary brain and other central nervous system tumors diagnosed in the United States in 2010–2014. Neuro-oncology 19:v1–v88. https://doi.org/10.1093/neuonc/nox158
Jiang T, Mao Y, Ma W, Mao Q, You Y, Yang X, Jiang C, Kang C, Li X, Chen L, Qiu X, Wang W, Li W, Yao Y, Li S, Li S, Wu A, Sai K, Bai H, Li G, Chen B, Yao K, Wei X, Liu X, Zhang Z, Dai Y, Lv S, Wang L, Lin Z, Dong J, Xu G, Ma X, Cai J, Zhang W, Wang H, Chen L, Zhang C, Yang P, Yan W, Liu Z, Hu H, Chen J, Liu Y, Yang Y, Wang Z, Wang Z, Wang Y, You G, Han L, Bao Z, Liu Y, Wang Y, Fan X, Liu S, Liu X, Wang Y, Wang Q, Chinese Glioma Cooperative Group (2016) CGCG clinical practice guidelines for the management of adult diffuse gliomas. Cancer Lett 375:263–273. https://doi.org/10.1016/j.canlet.2016.01.024
Hervey-Jumper SL, Li J, Lau D, Molinaro AM, Perry DW, Meng L, Berger MS (2015) Awake craniotomy to maximize glioma resection: methods and technical nuances over a 27-year period. J Neurosurg 123:325–339. https://doi.org/10.3171/2014.10.jns141520
Jakola AS, Myrmel KS, Kloster R, Torp SH, Lindal S, Unsgard G, Solheim O (2012) Comparison of a strategy favoring early surgical resection vs a strategy favoring watchful waiting in low-grade gliomas. JAMA 308:1881–1888. https://doi.org/10.1001/jama.2012.12807
McGirt MJ, Chaichana KL, Attenello FJ, Weingart JD, Than K, Burger PC, Olivi A, Brem H, Quinones-Hinojosa A (2008) Extent of surgical resection is independently associated with survival in patients with hemispheric infiltrating low-grade gliomas. Neurosurgery 63:700–707; author reply 707–708. https://doi.org/10.1227/01.NEU.0000325729.41085.73
Markert JM (2012) The role of early resection vs biopsy in the management of low-grade gliomas. JAMA 308:1918–1919. https://doi.org/10.1001/jama.2012.14523
Smith JS, Chang EF, Lamborn KR, Chang SM, Prados MD, Cha S, Tihan T, Vandenberg S, McDermott MW, Berger MS (2008) Role of extent of resection in the long-term outcome of low-grade hemispheric gliomas. J Clin Oncol 26:1338–1345. https://doi.org/10.1200/JCO.2007.13.9337
Eseonu CI, Rincon-Torroella J, ReFaey K, Lee YM, Nangiana J, Vivas-Buitrago T, Quinones-Hinojosa A (2017) Awake craniotomy vs craniotomy under general anesthesia for perirolandic gliomas: evaluating perioperative complications and extent of resection. Neurosurgery 81:481–489. https://doi.org/10.1093/neuros/nyx023
Sanai N, Berger MS (2009) Operative techniques for gliomas and the value of extent of resection. Neurotherapeutics 6:478–486. https://doi.org/10.1016/j.nurt.2009.04.005
Walker JA, Quinones-Hinojosa A, Berger MS (2004) Intraoperative speech mapping in 17 bilingual patients undergoing resection of a mass lesion. Neurosurgery 54:113–117; discussion 118. https://doi.org/10.1227/01.neu.0000097270.95721.3b
Neuloh G, Pechstein U, Schramm J (2007) Motor tract monitoring during insular glioma surgery. J Neurosurg 106:582–592. https://doi.org/10.3171/jns.2007.106.4.582
Prabhu SS, Gasco J, Tummala S, Weinberg JS, Rao G (2011) Intraoperative magnetic resonance imaging-guided tractography with integrated monopolar subcortical functional mapping for resection of brain tumors. Clinical article. J Neurosurg 114:719–726. https://doi.org/10.3171/2010.9.JNS10481
Duffau H, Peggy Gatignol ST, Mandonnet E, Capelle L, Taillandier L (2008) Intraoperative subcortical stimulation mapping of language pathways in a consecutive series of 115 patients with Grade II glioma in the left dominant hemisphere. J Neurosurg 109:461–471. https://doi.org/10.3171/JNS/2008/109/9/0461
Duffau H, Capelle L, Sichez J, Faillot T, Abdennour L, Law Koune JD, Dadoun S, Bitar A, Arthuis F, Van Effenterre R, Fohanno D (1999) Intra-operative direct electrical stimulations of the central nervous system: the Salpetriere experience with 60 patients. Acta Neurochir (Wien) 141:1157–1167. https://doi.org/10.1007/s007010050413
Duffau H, Capelle L, Lopes M, Faillot T, Sichez JP, Fohanno D (2000) The insular lobe: physiopathological and surgical considerations. Neurosurgery 47:801–810; discussion 801–810. https://doi.org/10.1097/00006123-200010000-00001
Guyotat J, Signorelli F, Bret P (2005) Usefulness of direct electrical stimulations during surgery for gliomas located within eloquent brain regions. Neurochirurgie 51:368–378
Carrabba G, Fava E, Giussani C, Acerbi F, Portaluri F, Songa V, Stocchetti N, Branca V, Gaini SM, Bello L (2007) Cortical and subcortical motor mapping in rolandic and perirolandic glioma surgery: impact on postoperative morbidity and extent of resection. J Neurosurg Sci 51:45–51
Vassal M, Charroud C, Deverdun J, Le Bars E, Molino F, Bonnetblanc F, Boyer A, Dutta A, Herbet G, Moritz-Gasser S, Bonafe A, Duffau H, de Champfleur NM (2016) Recovery of functional connectivity of the sensorimotor network after surgery for diffuse low-grade gliomas involving the supplementary motor area. J Neurosurg. https://doi.org/10.3171/2016.4.JNS152484
Herbet G, Maheu M, Costi E, Lafargue G, Duffau H (2016) Mapping neuroplastic potential in brain-damaged patients. Brain J Neurol 139:829–844. https://doi.org/10.1093/brain/awv394
Chaichana KL, Parker SL, Olivi A, Quinones-Hinojosa A (2009) Long-term seizure outcomes in adult patients undergoing primary resection of malignant brain astrocytomas. Clinical article. J Neurosurg 111:282–292. https://doi.org/10.3171/2009.2.JNS081132
Leone MA, Ivashynka AV, Tonini MC, Bogliun G, Montano V, Ravetti C, Gambaro P, Paladin F, Beghi E, ARES Study Group (2011) Risk factors for a first epileptic seizure symptomatic of brain tumour or brain vascular malformation. A case control study. Swiss Med Wkly 141:w13155. https://doi.org/10.4414/smw.2011.13155
Sacko O, Lauwers-Cances V, Brauge D, Sesay M, Brenner A, Roux FE (2011) Awake craniotomy vs surgery under general anesthesia for resection of supratentorial lesions. Neurosurgery 68:1192–1198; discussion 1198–1199. https://doi.org/10.1227/NEU.0b013e31820c02a3
Englot DJ, Han SJ, Berger MS, Barbaro NM, Chang EF (2012) Extent of surgical resection predicts seizure freedom in low-grade temporal lobe brain tumors. Neurosurgery 70:921–928; discussion 928. https://doi.org/10.1227/NEU.0b013e31823c3a30
Acknowledgements
This study has received funding by the National High Technology Research and Development Program of China (863 Program, 2015AA020504), the National Basic Research Program of China (2015CB755500), and the National Natural Science Foundation of China (81601452).
Author information
Authors and Affiliations
Contributions
Study concept and design: FSY and LYM. Data acquisition and analysis: FSY and LYM. Statistics/verified analytical method: FSY, LYM, ZZ, and WYY. Writing the first draft: FSY, LYM, and WYY. Supervision: ZZ, WYY, and JT. Read and approved final version: all authors.
Corresponding authors
Ethics declarations
Conflicts of interest
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Ethics approval
Ethical approval for this retrospective study was received from the Local Institutional Review Board
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Dr. Yinyan Wang, Zhong Zhang and Tao Jiang were equal corresponding to this manuscript.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Fang, S., Li, Y., Wang, Y. et al. Awake craniotomy for gliomas involving motor-related areas: classification and function recovery. J Neurooncol 148, 317–325 (2020). https://doi.org/10.1007/s11060-020-03520-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-020-03520-w