
Abstract
Purpose
Non-small cell lung cancer (NSCLC) brain metastases are associated with substantial morbidity and mortality. During recent years, accompanying dramatic improvements in systemic disease control, NSCLC brain metastases have emerged as an increasingly relevant clinical problem. However, optimal surveillance practices remain poorly defined. This purpose of this study was to further characterize the natural history, clinical course and risk factors associated with earlier development of subsequent NSCLC brain metastases to better inform clinical practice and help guide survivorship care.
Methods
We retrospectively reviewed all institutional NSCLC brain metastasis cases treated with radiotherapy between 1997 and 2015. Exclusion criteria included presence of brain metastases at initial NSCLC diagnosis and incomplete staging information. Interval time to brain metastases and subsequent survival were characterized using Kaplan–Meier and multivariate Cox regression analyses.
Results
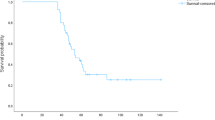
Among 105 patients within this cohort, median interval time to development of brain metastases was 16 months. Median interval times were 29, 19, 16 and 13 months for Stage I–IV patients, respectively (P = 0.016). Additional independent predictors for earlier development of NSCLC brain metastases included non-adenocarcinomatous histopathology (HR 3.036, P < 0.001), no prior surgical resection (HR 1.609, P = 0.036) and no prior systemic therapy (HR 3.560, P = 0.004). Median survival following intracranial progression was 16 months. Delayed development of brain metastases was associated with better prognosis (HR 0.970, P < 0.001) but not survival following intracranial disease onset.
Conclusions
Collectively, our results provide valuable insights into the natural history of NSCLC brain metastases. NSCLC stage, histology, prior surgical resection and prior systemic therapy emerged as independent predictors for interval time to brain metastases.

Similar content being viewed by others

References
Barnholtz-Sloan JS, Sloan AE, Davis FG, Vigneau FD, Lai P, Sawaya RE (2014) Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the metropolitan detroit cancer surveillance system. J Clin Oncol 22(14):2865–2872. https://doi.org/10.1200/JCO.2004.12.149
Wen PY, Loeffler JS (1999) Management of brain metastases. Oncol (willist Park 13(7):941–961
Lassman AB, DeAngelis LM (2003) Brain metastases. Neurol Clin N Am 21:1–23
Ostrom QT, Wright CH, Barnholtz-Sloan JS (2018) Brain metastases: epidemiology. Elsevier, Amsterdam. https://doi.org/10.1016/B978-0-12-811161-1.00002-5
Davis FG, Dolecek TA, Mccarthy BJ, Villano JL (2012) Toward determining the lifetime occurrence of metastatic brain tumors estimated from 2007 United States cancer incidence data. Neuro Oncol 14(9):1171–1177
Schouten LJ, Rooten J, Huveneers HAM, Twijnstra A (2002) Incidence of brain metastases in a cohort of patients with carcinoma of the breast, colon, kidney, and lung and melanoma. Cancer 94(10):2698–2705. https://doi.org/10.1002/cncr.10541
Sorensen BJB, Hansen HH, Hansen M, Dombernowsky P (1988) Brain metastases in adenocarcinoma of the lung: frequency, risk groups, and prognosis. J Clin Oncol 6(9):1474–1480
Gomez DR Jr, Lee GRB, et al (2016) Local consolidative therapy versus maintenance therapy or observation for patients with oligometastatic non-small-cell lung cancer without progression after first-line systemic therapy: a multicentre, randomised, controlled, phase 2 study. Lancet Oncol 17(12):1672–1682. https://doi.org/10.1016/S1470-2045(16)30532-0
Stephens SJ, Moravan MJ, Salama JK (2018) Managing patients with oligometastatic non-small-cell lung cancer POPULAR. J Oncol Pract 14(1):23–31. https://doi.org/10.1200/JOP.2017.026500
Hu C, Chang EL, Hassenbusch SJ et al (2006) Nonsmall cell lung cancer presenting with synchronous solitary brain metastasis. Cancer. https://doi.org/10.1002/cncr.21818
Sheehan JP, Sun M-H, Kondziolka D, Flickinger JC, Lunsford LD (2002) Radiosurgery for non-small cell lung carcinoma metastatic to the brain: long-term outcomes and prognostic factors influencing patient survival time and local tumor control. J Neurosurg 97:1276–1281
Goncalves PH, Peterson SL, Vigneau FD et al (2016) Risk of brain metastases in patients with nonmetastatic lung cancer: analysis of the metropolitan detroit Surveillance, Epidemiology, and End Results (SEER) data. Cancer June:1921–1927. https://doi.org/10.1002/cncr.30000
Rusthoven CG (2018) Prophylactic cranial irradiation in non-small-cell lung cancer: the costs outweigh the benefits. J Clin Oncol 36(34):3433–3435. https://doi.org/10.1200/JCO.18.00732
Addeo A, Caparrotti F, Picardi C, Dietrich P-Y (2018) Prophylactic cranial irradiation in stage III non-small-cell lung cancer: overall survival should not necessarily be the final end point. J Clin Oncol 36(34):25–26. https://doi.org/10.1200/JCO.18.00461
Zeng H, Yuan S, Yu J (2018) Prophylactic cranial irradiation in non-small-cell lung cancer: hope or hype? J Clin Oncol 36(34):3431–3433. https://doi.org/10.1200/JCO.18.00617
Hubbs JL, Boyd JA, Hollis D, Chino JP, Saynak M, Kelsey CR (2010) Factors associated with the development of brain metastases. Cancer. https://doi.org/10.1002/cncr.25254
Figlin RA, Piantadosi S, Feld R, Group TLCS (1988) Intracranial recurrence of carcinoma after complete surgical resection of stage I, II and III non-small cell lung cancer. N Engl J Med 318(20):1300–1305
Ceresoli GL, Reni M, Chiesa G et al (2002) Brain metastases in locally advanced nonsmall cell lung carcinoma after multimodality treatment risk factors analysis. Cancer 95(3):605–612. https://doi.org/10.1002/cncr.10687
Gaspar LE, Chansky K, Albain KS et al (2005) Time from treatment to subsequent diagnosis of brain metastases in stage III non-small-cell lung cancer: a retrospective review by the Southwest Oncology Group. J Clin Oncol 23(13):2955–2961. https://doi.org/10.1200/JCO.2005.08.026
Carolan H, Sun AY, Bezjak A et al (2003) Does the incidence and outcome of brain metastases in locally advanced non-small cell lung cancer justify prophylactic cranial irradiation or early detection? Lung Cancer. https://doi.org/10.1016/j.lungcan.2004.12.004
Mamon HJ, Yeap BY, Ja PA (2005) High risk of brain metastases in surgically staged III A non-small-cell lung cancer patients treated with surgery, chemotherapy, and radiation. J Clin Oncol 23(7):1530–1537. https://doi.org/10.1200/JCO.2005.04.123
Chang EL, Wefel JS, Ph D, Ph D, Allen PK, Ph D (2007) A pilot study of neurocognitive function in patients with one to three brain metastases initially treated with stereotactic radiosurgery alone. Neurosurgery 60(2):277–284. https://doi.org/10.1227/01.NEU.0000249272.64439.B1
Mehta MP, Rodrigus P, Terhaard CHJ et al (2003) Survival and neurologic outcomes in a randomized trial of motexafin gadolinium and whole-brain radiation therapy in brain metastases. J Clin Oncol 21(13):2529–2536. https://doi.org/10.1200/JCO.2003.12.122
Cordes M, Scherwath A, Ahmad T et al (2014) Distress, anxiety and depression in patients with brain metastases before and after radiotherapy. BMC Cancer 14(731):1–11
Peters S, Bexelius C, Munk V, Leighl N (2016) The impact of brain metastasis on quality of life, resource utilization and survival in patients with non-small-cell lung cancer. Cancer Treat Rev 45:139–162. https://doi.org/10.1016/j.ctrv.2016.03.009
Walker MS, Wong W, Ravelo A, Miller PJE, Schwartzberg LS (2018) Effect of brain metastasis on patient-reported outcomes in advanced NSCLC treated in real-world community oncology settings. Clin Lung Cancer 19(2):139–147. https://doi.org/10.1016/j.cllc.2017.10.003
Guerin A, Sasane M, Dea K, Zhang J, Culver K, Nitulescu R (2016) The economic burden of brain metastasis among lung cancer patients in the United States. J Med Econ 19(5):526–536
DeRuysscher D, Dingemans AC, Praag J et al (2018) Prophylactic cranial irradiation versus observation in radically treated stage III Non-small-cell lung cancer: a randomized phase III NVALT-11/DLCRG-02 study. J Clin Oncol. https://doi.org/10.1200/JCO.2017.77.5817
Palma DA, Olson RA, Harrow S et al (2018) Stereotactic ablative radiation therapy for the comprehensive treatment of oligometastatic tumors (SABR-COMET): results of a randomized trial. Int J Radiat Oncol Biol Phys 102(3):S3–S4. https://doi.org/10.1016/j.ijrobp.2018.06.105
Robnett TJ, Machtay M, Stevenson JP, Algazy KM, Hahn SM (2001) Factors affecting the risk of brain metastases after definitive chemoradiation for locally advanced non-small-cell lung carcinoma. J Clin Oncol 19(5):1344–1349
Bajard A, Westeel V, Dubiez A et al (2004) Multivariate analysis of factors predictive of brain metastases in localised non-small cell lung carcinoma. Lung Cancer 45:317–323. https://doi.org/10.1016/j.lungcan.2004.01.025
Chen AM, Jahan TM, Jablons DM, Garcia J, Larson DA (2007) Risk of cerebral metastases and neurological death after pathological complete response to neoadjuvant therapy for locally advanced. Cancer 109(8):1668–1675. https://doi.org/10.1002/cncr.22565
Sperduto PW, Kased N, Roberge D et al (2012) Summary report on the graded prognostic assessment: an accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J Clin Oncol 30(4):419–425. https://doi.org/10.1200/JCO.2011.38.0527
Ding X, Dai H, Hui Z et al (2012) Risk factors of brain metastases in completely resected pathological stage IIIA-N2 non-small cell lung cancer. Radiat Oncol 7(119):1–10
Chang W, Wu Y, Su P, Yang S, Lin C (2018) The impact of EGFR mutations on the incidence and survival of stages I to III NSCLC patients with subsequent brain metastasis. PLoS ONE 13:1–16
Ji Z, Bi N, Wang J et al (2014) Risk factors for brain metastases in locally advanced non-small cell lung cancer with definitive chest radiation. Radiat Oncol Biol 89(2):330–337. https://doi.org/10.1016/j.ijrobp.2014.02.025
Andre F, Grunenwald D, Pujol JL, Girard P, Dujon A, Brichon PY (2001) Patterns of relapse of N2 nonsmall-cell lung carcinoma patients treated with preoperative chemotherapy should prophylactic cranial irradiation be reconsidered? Cancer 91(12):2394–2400
Won Y, Joo J, Yun T et al (2015) Lung Cancer A nomogram to predict brain metastasis as the first relapse in curatively resected non-small cell lung cancer patients. Lung Cancer 88(2):201–207. https://doi.org/10.1016/j.lungcan.2015.02.006
Zhang F, Zheng W, Ying L, Wu J, Wu S (2016) A Nomogram to Predict Brain Metastases of Resected Non-Small Cell Lung Cancer Patients. Ann Surg Oncol 23:3033–3039. https://doi.org/10.1245/s10434-016-5206-3
An N, Jing W, Wang H et al (2018) Risk factors for brain metastases in patients with non-small cell lung cancer. Cancer Med. https://doi.org/10.1002/cam4.1865
Albain KS, Swann RS, Rusch VW et al (2009) Radiotherapy plus chemotherapy with or without surgical resection for stage III non-small-cell lung cancer: a phase III randomised controlled trial. Lancet 374(9687):379–386. https://doi.org/10.1016/S0140-6736(09)60737-6
Meerbeeck JP, Van Kramer GWPM, Schil PEY, Van et al (2007) randomized controlled trial of resection versus radiotherapy after induction chemotherapy in stage IIIA-N2 non-small-cell lung cancer. JNCI. https://doi.org/10.1093/jnci/djk093
Chamberlain MC, Baik CS, Gadi VK, Bhatia S, Chow LQM (2017) Systemic therapy of brain metastases: non-small cell lung cancer, breast cancer and melanoma. Neuro Oncol 19(1):1–24. https://doi.org/10.1093/neuonc/now197
Sperduto PW, Yang TJ, Beal K et al (2016) The effect of gene alterations and tyrosine kinase inhibition on survival and cause of death in patients with adenocarcinoma of the lung and brain metastases. Int J Radiat Oncol Biol Phys 96(2):406–413. https://doi.org/10.1016/j.ijrobp.2016.06.006
Sperduto PW, Yang TJ, Beal K et al (2017) Estimating survival in patients with lung cancer and brain metastases an update of the graded prognostic assessment for lung cancer using molecular markers (Lung-molGPA). JAMA Oncol 55387:827–831. https://doi.org/10.1001/jamaoncol.2016.3834
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Wang reports personal fees and non-financial support from AbbVie, non-financial support from Merck, personal fees from AstraZeneca, personal fees from Doximity, personal fees and non-financial support from Novocure, personal fees and non-financial support from Elekta and personal fees from Wolters Kluwer, outside the submitted work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Smith, D.R., Bian, Y., Wu, CC. et al. Natural history, clinical course and predictors of interval time from initial diagnosis to development of subsequent NSCLC brain metastases. J Neurooncol 143, 145–155 (2019). https://doi.org/10.1007/s11060-019-03149-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-019-03149-4