
Abstract
Background
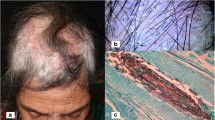
Novel treatments against for tinea capitis are needed, and the natural aminosterol squalamine is a potential topical antidermatophyte drug candidate.
Objectives
This phase II randomized double-blind placebo-controlled clinical trial aimed at testing the efficacy and safety of a three-week squalamine ointment regimen for the treatment of tinea capitis.
Patients
Males aged 6–15 years presenting with tinea capitis were treated with either topical squalamine ointment or placebo for 3 weeks. The primary endpoint was complete clinical cure. The secondary endpoints were the occurrence of local and/or systemic adverse events, mycological cure, and partial clinical response. Prospective follow-up of clinical adverse events was performed daily.
Results
Five patients were treated with 1 % squalamine ointment and 15 with placebo. No complete cure was observed. No clinical or biological adverse event was recorded. A significantly (p = 0.03) better hair-growth score, indicating a partial clinical improvement of the tinea capitis lesion, was observed in the patients treated with squalamine compared to those treated with placebo.
Conclusion
This three-week squalamine ointment regimen was well tolerated and showed an encouraging partial clinical activity for the treatment of tinea capitis. Further studies are needed to evaluate the efficacy of topical squalamine alone against tinea corporis or in combination with a systemic antidermatophyte drug against tinea capitis.

Similar content being viewed by others


References
Mohrenschlager M, Seidl HP, Ring J, Abeck D. Pediatric tinea capitis: recognition and management. Am J Clin Dermatol. 2005;6:203–13.
Blaithin M, Roderick H, Racheal M. The diagnosis and management of tinea. BMJ. 2012;10(345):e4380. doi:10.1136/bmj.e4380.
Sharma V, Hall JC, Knapp JF, Sarai S, Galloway D, Babel DE. Scalp colonization by Trichophyton tonsurans in an urban pediatric clinic. Asymptomatic carrier state? Arch Dermatol. 1988;124:1511–3.
Abdel-Rahman SM, Farrand N, Schuenemann E, Stering TK, Preuett B, Magie R, Campbell A. The prevalence of infections with Trichophyton tonsurans in schoolchildren: the CAPITIS study. Pediatrics. 2010;125:966–73.
Coulibaly O, Thera MA, Djimde AA, Ranque S. Dermatomycoses in rural and peri-urban schoolchildren in Mali. Mycoses. 2011;54:68.
Sanguinettti M, Posteraro B, Romano L, Battaglia F, Lopizzo T, De Carolis E, Fadda G. In vitro activity of Citrus bergamia (bergamot) oil against clinical isolates of dermatophytes. J Antimicrob Chemother. 2007;59:305–8.
Coulibaly O, Alhanout K, L’Ollivier C, Brunel JM, Thera MA, Djimdé AA, Doumbo OK, Piarroux R, Ranque S. In vitro activity of aminosterols against dermatophytes. Med Mycol. 2013;51:309–12.
Alhanout K, Brunel JM, Ranque S, Rolain JM. In vitro antifungal activity of aminosterols against mould isolates from cystic fibrosis patients. J Antimicrob Chemother. 2010;65:1307–9.
Brunel JM, Salmi C, Loncle C, Vidal N, Letourneux Y. Squalamine: a polyvalent drug of the future? Curr Cancer Drug Targets. 2005;5:267–72.
Chan YC, Friedlander SF. New treatments for tinea capitis. Curr Opin Infect Dis. 2004;17:97–103.
Greer DL. Successful treatment of tinea capitis with 2 % ketoconazole shampoo. Int J Dermatol. 2000;39:302–4.
Bookstaver PB, Watson HJ, Winters SD, Carlson AL, Schulz RM. Prophylactic ketoconazole shampoo for tinea capitis in a high-risk pediatric population. J Pediatr Pharmacol Ther. 2011;16:199–203.
Djouhri-Bouktab L, Alhanout K, Andrieu V, Raoult D, Rolain JM, Brunel JM. Squalamine ointment for Staphylococcus aureus skin decolonization in a mouse model. J Antimicrob Chemother. 2011;66:1306–10.
Paugam A, L’ollivier C, Viguié C, Anaya L, Mary C, de Ponfilly G, Ranque S. Comparison of real-time PCR with conventional methods to detect dermatophytes in samples from patients with suspected dermatophytosis. J Microbiol Methods. 2013;95:218–22.
Alhanout K, Di Giorgio C, De Méo M, Brunel JM. Non-genotoxic assessment of a natural antimicrobial agent: squalamine. Anti-Infective Agents. 2014;12:75–79.
Herbst RS, Hammond LA, Carbone DP, Tran HT, Holroyd KJ, Desai A, Williams JI, Bekele BN, Hait H, Allgood V, Solomon S, Schiller JH. A phase I/IIA trial of continuous five-day infusion of squalamine lactate (MSI-1256F) plus carboplatin and paclitaxel in patients with advanced non-small cell lung cancer. Clin Cancer Res. 2003;15:4108–15.
Bennett ML, Fleischer AB, Loveless JW, Feldman SR. Oral griseofulvin remains the treatment of choice for tinea capitis in children. Pediatr Dermatol. 2000;17:304–9.
Lipozencic J, Skerlev M, Orofino-Costa R, Zaitz VC, Horvath A, Chouela E, Romero G, Gourmala N, Paul C, Tinea Capitis Study Group. A randomized double-blind, parallel group, duration funding study of oral terbinafine and open-label, high-dose griseofulvin in children with tinea capitis due to Microsporum species. Br J Dermatol. 2002;146:816–23.
Grover C, Arora P, Manchanda V. Comparative evaluation of griseofulvin, terbinafine, and fluconazole in the treatment of tinea capitis. Int J Dermatol. 2012;51:455–8.
Acknowledgments
We would like to thank the school principal Jean-André Douyon for his help.
Conflict of interest
None to declare.
Author information
Authors and Affiliations
Corresponding author
Additional information
Trial registration: www.pactr.orgPACTR201306000522355.
Rights and permissions
About this article

Cite this article
Coulibaly, O., Thera, M.A., Koné, A.K. et al. A Double-Blind Randomized Placebo-Controlled Clinical Trial of Squalamine Ointment for tinea capitis Treatment. Mycopathologia 179, 187–193 (2015). https://doi.org/10.1007/s11046-014-9849-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11046-014-9849-y