
Abstract
Xeroderma pigmentosum (XP) is a rare autosomal recessive disease that is associated with a severe deficiency in nucleotide excision repair. Genetic polymorphisms in XP genes may be associated with a change in DNA repair capacity, which could be associated with colorectal cancer development. We assessed the association between 94 single nucleotide polymorphisms (SNPs) within seven XP genes (XPA–XPG) and the colorectal cancer risk in the Polish population. We genotyped 758 unselected patients with colorectal cancer and 1,841 healthy adults. We found that a significantly decreased risk of colorectal cancer was associated with XPC polymorphism rs2228000_CT genotype (OR 0.59; p < 0.0001) and the rs2228000_TT genotype (OR 0.29; p < 0.0001) compared to the reference genotype (CC). And an increased disease risk was associated with the XPD SNP, rs1799793_AG genotype (OR 1.44, p = 0.018) and rs1799793_AA genotype (OR 3.31, p < 0.0001) compared to the reference genotype. Haplotype analysis within XPC, XPD and XPG revealed haplotypes associated with an altered colorectal cancer risk. Stratified analysis by gender showed differences between the association of three SNPs: XPC rs2228000, XPD rs1799793 and XPD rs238406 in females and males. Association analysis between age of disease onset and polymorphisms in XPD (rs1799793) and XPC (rs2228000) revealed differences in the prevalence of these variants in patients under and over 50 years of age. Our results confirmed that polymorphisms in XPC and XPD may be associated with the risk of colorectal cancer.
Similar content being viewed by others

Introduction
Colorectal cancer was second most commonly reported malignancy in 2010 in Poland. It represented 12.4 % of all diagnosed male and 10.1 % female malignancies, respectively [1]. Worldwide colorectal carcinoma was the third most frequently diagnosed cancer in 2009 [2] yet it is preventable if diagnosed early. Colorectal cancer risk is attributable to rare germline and or somatic mutations in a variety of tumor suppressor genes, that include APC [3, 4], TP53 [5]; proto-oncogenes, KRAS, BRAF, CTNNB1/beta-catenin, PIK3CA, SRC [4]; cell cycle regulatory genes FBXW7 [4]; DNA mismatch repair genes MLH1, MSH2, MSH6, PMS2 [6], DNA base excision repair genes OGG1 [7], MUTYH [8]; and many other common, low-penetrant genetic variants, which together may be associated with colorectal cancer development [9].
Nucleotide excision repair (NER) genes play a crucial role in the maintenance of genomic integrity by removing UV-light-induced DNA lesions [10] as well as those that are a result of UV-mimetic agents. Given the environmental exposure of the colon and rectum to a variety of genotoxic agents any change in the fidelity of this process may influence the risk of disease development. Numerous polymorphisms of NER genes have been identified and individually or in combination may adversely affect NER fidelity, which could contribute to the risk of colorectal cancer. A number of studies have examined whether there is a correlation between NER gene polymorphisms and colorectal cancer risk. The results to date, however, remain inconclusive and do not provide any clear direction concerning their involvement in CRC. Several reports suggest an association between NER genes and colorectal cancer risk [11–16] whereas others have indicated no correlation with disease [17–23].
The aim of this study was to examine associations between genetic variants in DNA repair genes and colorectal cancer risk in the Polish population-based case–control data set. A total of 15 SNPs (selected from a panel of 94 polymorphisms as described previously [24] ) were examined in 758 unselected patients with colorectal cancer and their frequency compared to that found in 1,841 healthy adults. Logistic regression and haplotype analysis was undertaken to assess the impact of these polymorphisms on CRC genetic susceptibility.
Patients and methods
Patients
For this study a group of 758 unselected colorectal cancer patients were invited to participate in this research: There were 355 women (mean age at diagnosis, 62.61 years) and 403 men (mean age at diagnosis, 63.34 years) from Poland. The minimum age at onset was 23 years among men and 27 among women and the maximum age at onset was 92 in both male and female. An early-onset CRC (<50) was present in 17.3 % cases (men : 16.6 %; women: 17.7 %). Data on cancer location was available for 625 cases. Of the 625 cases, 118 individuals were diagnosed with right-sided CRC, 467 were diagnosed with left-sided cancer and 40 cases had tumors in an unspecified location of the colon. Tumors from the cecum through the transverse colon were classified as right-sided colon cancers, tumors from the splenic flexure to rectum were considered to be left side colon cancers. Patients were diagnosed between the years 2005 and 2008 at the Surgical Oncology Clinic, Pomeranian Medical University, Szczecin. The registries used to identify patients captures over 95 % of all diagnosed cancers within the geographical region of Szczecin.
The control group consisted of 1,841 healthy adults: 860 women (mean age, 64 years) and 981 men (mean age, 67 years). These healthy adults had a negative cancer family history for first- and second-degree relatives defined by answering a questionnaire about their family’s medical history. This was part of a population-based study of the 1.5 million residents of West Pomerania aimed at identifying familial aggregations of malignancies performed recently by our center. During the interview, the goals of the study were explained, informed consent was obtained, genetic counseling was given and a blood sample taken for DNA analysis. Individuals affected with any malignancy or with cancers diagnosed among first- or second- degree relatives were excluded from the study.
Informed consent was obtained from all participants prior to the collection of a blood sample for DNA isolation. The study was approved by the institutional review board of the Pomeranian Medical University.
Methods
SNPs selection
The 94 SNPs located in the seven DNA repair genes (XPA: 8 SNPs, XPB: 10 SNPs, XPC: 16 SNPs, XPD: 11 SNPs, XPE: 5 SNPs, XPF: 16 SNPs XPG: 28 SNPs) were selected in a previous study from http://snpper.chip.org/ [25] (for details see [24]). All single-nucleotide polymorphisms were non-synonymous or present within the exon/intron boundaries of the respective gene or located in the 5′-UTR and 3′-UTR sequences. The minimum threshold for minor allele genotype frequency was set at 5 %. Out of 94 SNPs present within the 7 genes 15 were eligible for detailed analysis (Table 1).
Genotyping
Genotyping was performed using DNA isolated from peripheral blood samples taken from colorectal cancer patients and healthy controls according to the method of Miller et al. (1986) [26]. Molecular analysis was performed using a combination of real-time PCR (LightCycler 480, Roche, Penzberg, Germany) and MassARRAY MALDI-TOF MS analysis (Sequenom Inc., San Diego, CA, USA). For real-time PCR TaqMan probes were used (Applied Biosystems, Foster City, CA). MALDI-TOF analysis was based on a primer extension reaction to detect and determine the SNP allele. Reactions were performed according to the manufacturer’s instructions.
Sequencing
Random DNA samples were sequenced to verify the results of the MassARRAY genotyping and real-time PCR analysis (data not shown). Sequencing was conducted using universal primers in combination with the ABI PRISM BigDye Terminator Cycle kit (Applied Biosystems, Foster City, CA). The sequencing was performed in the 3130 Genetic Analyzer (Applied Biosystems, Foster City, CA).
Statistics
Possible deviation of the allele frequencies from those expected under Hardy–Weinberg equilibrium (HWE) was also assessed using the Chi square analysis [27]. Genotype frequency differences, the odds ratio (OR) and 95 % confidence intervals (95 % Cl) were estimated using regression analysis for additive model of inheritance. Logistic regression analysis was performed using R software environment version 2.15.0 [28].
Haplotype frequencies and their potential association with disease risk were estimated using the haplo.stats CRAN package (version 1.5.5) by Sinnwell and Schaid for an R environment [29].
Linkage disequilibrium between SNPs for a given haplotype was calculated using the software JLIN by Carter et al. [30] as described in a previous study [24].
Bonferroni correction for multiple testing was applied to all results that demonstrated a significant difference between the cases and controls.
Results
All SNPs tested were in Hardy–Weinberg Equilibrium within the control and CRC populations under study. This indicates that any differences observed in the study population are a result of differences attributable to those SNPs that are significantly different in frequency between the control and the colorectal cancer population.
A number of SNPs were found to be in linkage disequilibrium (LD). These were in XPC: rs2228001, G1475A, G2061A, rs2228000 and rs3731062 that we have previously observed [24].
From the 15 SNPs analyzed, logistic regression revealed one SNP in XPC and one in XPD was associated with colorectal cancer risk. A significantly decreased colorectal cancer risk was identified for the XPC rs2228000 (Ala499Val) CT genotype (OR 0.59; p < 0.0001) and for TT genotype (OR 0.29; p < 0.0001) compared to the reference genotype (CC). And an increased risk of disease was associated with the XPD SNP, rs1799793 (Asp312Asn-) AG genotype (OR 1.44; p = 0.018) and for AA genotype (OR 3.31; p < 0.0001) compared to the control population. These results all remained significant after Bonferroni Correction (see Table 1). None of the other SNPs were found to be associated with colorectal cancer risk.
Gender and colorectal cancer risk
XPC gene
Gender stratification analysis revealed differences in the association of the rs2228000_TT genotype in females compared to males (Table 2). Women who were heterozygous for this SNP appeared to have a significantly reduced risk of colorectal cancer compared to the control population (OR 0.2; 95 % CI 0.15–0.28) which was further reduced in the homozygous state (OR 0.1; 95 % CI = 0.06–0.17) whereas in males there was no association in the heterozygous state but a similar reduced risk if homozygous (OR 0.44; 95 % CI 0.26–0.75).
XPD gene
The polymorphisms in XPD (rs1799793, rs238406) were both associated with colorectal cancer development. Both AA and AG genotypes in XPD rs1799793 were strongly associated with increasing cancer risk in males (OR 6.92, 95 % CI 4.61–10.36; OR 1.92, 95 % CI 1.42–2.62), whereas in females there appeared to be an association with homozygosity but no relationship with heterozygosity. After Bonferroni correction, the association with males and risk remained but became non-significant in females. For XPD rs238406_AA was significantly associated with cancer development in women (OR 2.02, p = 0.006) but not in men. The opposite tendency was observed in male CRC patients, where the XPD rs238406_AA and AC genotypes were associated with a decreased risk of disease (OR 0.69, CI 0.47–0.99; and OR 0.51, CI 0.38–0.68, respectively). After Bonferroni correction only males that were heterozygous for the rs238406 SNP were associated with a decrease in cancer risk.
Age and colorectal cancer risk
Dichotomizing the patients into two groups (those under 50 years of age and those equal to or above 50 years of age) revealed an association of the 2 SNPs within XPC and XPD genes with colorectal cancer risk (Table 3).
Both XPC rs2228000_TT and CT genotypes decreased cancer risk only in patients over 50 years of age (OR 0.27 CI 0.18–0.40; OR 0.59 CI 0.47–0.73, respectively). The significance remained after Bonferroni correction.
For XPD rs1799793 disease risk did not appear to differ between the two age groups for patients homozygous for the SNP, for patients <50 years of age OR 3.64 CI 2.01–6.61) and patients ≥50 years of age (OR 3.23 CI 3.23–4.38) among patients having homozygotes variant AA at XPD rs1799793. Patients who were heterozygous for this SNP, there appeared to be a tendency, which was in the same direction of the causal SNP, of an increased risk of disease. For patients over 50 years of age, there was a statistically significant increase in disease risk although the effect size was somewhat modest. For patients under 50 years of age, a tendency towards an association was observed but it was not statistically significant.
Haplotype analysis
XPC
Using the Haplo.stats CRAN package (version 1.5.5) [29] we undertook haplotype analysis for XPC. The analysis revealed three haplotypes that were associated with a significantly decreased disease risk and one that significantly increased colorectal cancer risk compared to the reference haplotype: GCGCC (see Table 4). Moreover, the haplotype GAGCC appeared to be associated with a significant increase in disease risk (OR 2.56 CI 1.94–3.39). For the remaining haplotypes, no significant differences in disease risk between cases and controls were identified (Table 4).
XPD
Haplotype analysis of XPD revealed two protective haplotypes and three that were associated with an increase in disease risk (Table 4).
XPG
Differences in the haplotype structure revealed two that were protective against colorectal cancer and two that were linked to an enhanced risk of disease (Table 4).
Discussion
In this case–control study that included 758 patients with colorectal cancer and 1,841 healthy adults, we found that the XPC rs2228000 (Ala499Val) and the XPD rs1799793 (Asp312Asn-) polymorphisms were significantly associated with an altered colorectal cancer risk.
Logistic regression revealed that the XPC rs2228000_CT or _TT genotype was significantly associated with a decreased colorectal cancer risk. Gender stratification demonstrated that this correlation is more evident among women than men. Haplotype analysis of the XPC gene suggested that there are 3 protective XPC alleles. We found no association between the remaining variants of XPC and colorectal cancer risk.
To the best of our knowledge, only a few studies have investigated the role of XPC in colorectal cancer and the published data remains inconclusive. None of these studies demonstrated a clear association rs2228000 polymorphisms with colorectal cancer risk. Huang et al. examined 772 patients with distal colon cancer and 777 controls and suggested no correlation between all examined XPC polymorphisms (Arg492His, Ala499Val, Lys939Gln) and colorectal cancer risk, however they suggested that the smoking-associated risk in CRC was modified by haplotypes containing the XPC 499Val variant [21]. Wu et al. assessed the correlation between XPC polymorphisms and colorectal cancer development among 421 CRC patients and 845 controls. The study showed no significant association between Ala499Val and CRC risk, but a significant decrease risk of rectal cancer correlated with CT and TT genotypes [12]. Berndt et al. examined 5 SNPs in XPC among 250 colorectal cancer patients and 2,228 controls, authors suggested increased risk of colorectal cancer among patients having at least one 492His allele of the XPC Arg492His (rs2227999) and no association of the remaining SNPs (including rs2228001 and rs2228000) with colorectal cancer [13].
A meta-analysis focused on the role of XPC in carcinogenesis, which revealed two SNPs in XPC (rs2228001 and rs2228000) that were significantly associated with overall cancer risk. A meta-analysis that included 6 studies examined XPC rs2228001 as a risk factor for colorectal cancer (2,751 cases and 3,607 controls) but failed to include studies examining the role of XPC rs2228000. This report did, however, show that rs2228001 was associated with colorectal cancer risk [14].
Similar conclusions have been drawn from reports from Liu et al. [11] and Wu, et al. (2011) [12]. In Liu et al., after evaluation of 1028 CRC cases and 1,085 controls they found that the Lys939Gln (AC or CC genotype) was associated with an increased risk of colorectal cancer [11]. In the other study, which evaluated 421 colorectal cancer patients and 845 healthy individuals the results suggested that the CC genotype in the Lys939Gln and PAT +/+ genotype in an intronic biallelic poly(AT) insertion/deletion polymorphism in XPC increased CRC risk [14]. Our results of XPC suggested no association between Lys939Gln with colorectal cancer risk and confirmed the conclusions from two previous reports [18, 23].
Logistic regression analysis of XPD genotypes in our study revealed an association with XPD rs1799793 (Asp312Asn-) AG and AA genotypes with an increased colorectal cancer risk. This association appeared greater in men. Previously published data focusing on the correlation between XPD gene polymorphisms and the risk of colorectal cancer development were inconclusive. Some reports have suggested an association of XPD polymorphisms with CRC [15, 16, 32] whereas others have not observed any such correlation [13, 16, 19, 21, 23, 31].
There have been eight previous reports examining relationship between Asp312Asn polymorphism and CRC and most have failed to detect any association [13, 16, 19, 21, 23, 31]. Only Jelonek et al. examined 153 CRC cases and 507 controls from the Polish population and found that the AA genotype in XPD Asp312Asn- was overrepresented in the colorectal cancer group [32].
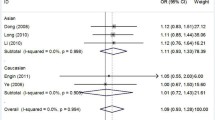
Most of the reports are concentrated on assessing the impact of Lys751Gln polymorphism on CRC risk. The results from the present study revealed a lack of association between XPD Lys751Gln and colorectal cancer risk, which confirmed several previous reports [17, 18, 33]. Likewise, another Polish report utilizing 100 cases and 100 controls suggested that the XPD Lys751Gln did not appear to contribute significantly to disease risk in the Polish population [34]. In contrast to our findings, Jelonek et al. [32] found that XPD 751Gln (C allele) was more frequent in the cancer group but failed to reach statistical significance. Whereas Skjelbred et al. suggested that carriers of the variant genotype of XPD Lys751Gln had an increased risk of low-risk adenomas but not carcinomas [15]. Another Polish study (100 CRC cases and 100 controls) reported that XPD Lys751Gln was associated with decreased risk of CRC for individuals harboring at least one A allele [16]. All these studies were performed on relatively small samples size (less than 200 cases) and each suffered from a lack of power to detect small effect sizes.
A meta-analysis that included 15 studies (Lys751Gln) containing 3,042 CRC cases and 4,672 controls and seven studies (Asp312Asn) containing 1,581 cases and 2,846 controls, suggested that both polymorphisms in XPD are not significantly associated with CRC risk [19]. Similar findings were obtained by Stern et al. [20], Huang et al. [21], Moreno, et al. [22] and Hansen et al. [23]. In these studies the groups examined consisted of, 310 cases and 1,176 controls [20], 772 cases and 777 controls [21], 377 cases and 329 controls [22], 405 cases and 810 controls [23]. All reports failed to identify any correlation between these SNPs and the risk of colorectal cancer. Our observation confirm previous findings with respect to the XPD Lys751Gln polymorphism demonstrating it is not associated with colorectal cancer risk. We could not, however, explain the negative results of XPD Asp312Asn. This discrepancy and conflicting data may be a result of population stratification or the relatively small numbers of cases used in the study.
All SNPs in XPE, XPF, XPG that were examined in this study, did not appear to contribute significantly to disease risk in the Polish population, except for XPG rs17655 (Asp1104His). The heterozygous genotype CG of rs17655 was associated with an increased risk of colorectal cancer, which confirmed the findings of Liu et al. [11]. The analysis undertaken by Liu et al. [11] was performed on 1,557 CRC patients and 1,085 controls. Our results confirmed previous reports about the lack of any association between XPE, XPF, XPG polymorphisms with colorectal cancer risk [13, 16, 21, 22, 31, 35].
To our knowledge, there is little if any haplotype data available for the assessment of disease risk between NER genes and colorectal cancer. In this study we have examined several haplotypes in XPC, XPD and XPG. Many of the SNPs examined result in amino acid substitutions, which have the potential to alter the kinetic properties of the respective NER protein. When investigating XPG, no individual SNP was found to be associated with any change in CRC risk but we observed four haplotypes that were significant, two that increased risk and two that decreased risk. This provides some evidence to suggest that combinations of polymorphisms should be examined in more detail to reveal associations that are not immediately apparent.
In conclusion, this study suggests that XPC rs2228000 (Ala499Val) and the XPD rs1799793 (Asp312Asn-) polymorphisms are significantly associated with an alteration in colorectal cancer risk. However, it remains necessary to conduct additional larger studies taking into account environmental factors to assess gene environment interactions to fully understand the relationship between NER and colorectal cancer susceptibility. Future studies will result in a better understanding of the role of NER gene polymorphisms in colorectal cancer development.
References
Wojciechowska U, Didkowska J, Zatoński W (2012) Cancer in Poland in 2010. Polish National Cancer Registry, Department of Epidemiology and Cancer Prevention, Warsaw
Siegel R, Naishadham D, Jemal A (2013) Cancer statistics, 2013. CA Cancer J Clin 63(1):11–30
Leppert M, Burt R, Hughes JP, Samowitz W, Nakamura Y, Woodward S et al (1990) Genetic analysis of an inherited predisposition to colon cancer in a family with a variable number of adenomatous polyps. N Engl J Med 322(13):904–908
Roy S, Majumdar AP (2012) Cancer stem cells in colorectal cancer: genetic and epigenetic changes. J Stem Cell Res Ther. Suppl 7(6):10342
Yu XJ, Fang F, Xie J (2011) Relationship between TP73 polymorphism (G4C14-A4T14) and cancer risk: a meta-analysis based on literatures. Gene 484(1–2):42–46
Musulen E, Blanco I, Carrato C, Fernandez-Figueras MT, Pineda M, Capella G et al (2013) Usefulness of epithelial cell adhesion molecule expression in the algorithmic approach to Lynch syndrome identification. Hum Pathol 11:412–416
Su Y, Xu A, Zhu J (2013) The effect of oxoguanine glycosylase 1 rs1052133 polymorphism on colorectal cancer risk in Caucasian population. Tumour Biol 35(1):513–517
Al-Tassan N, Chmiel NH, Maynard J, Fleming N, Livingston AL, Williams GT et al (2002) Inherited variants of MYH associated with somatic G:C → T: a mutations in colorectal tumors. Nat Genet 30:227–232
Abuli A, Fernandez-Rozadilla C, Giraldwz MD, Muñoz J, Gonzalo V, Bessa X et al (2011) A two-phase case–control study for colorectal cancer genetic susceptibility: candidates genes from chromosomal regions 9q22 and 3q22. Br J Cancer 105(6):870–875
Cleaver JE (2002) Allelic variations of the XP genes. http://xpmutations.org/genes.html
Liu D, Wu H, Zhang Y, Kang H, Sun M, Wang E et al (2012) DNA repair genes XPC, XPG polymorphisms: relation to the risk of colorectal carcinoma and therapeutic outcome with oxaliplatin-base adjuvant chemotherapy. Mol Carcinog Suppl 1(51):e83–e93
Wu Y, Jin M, Liu B, Liang X, Yu Y, Li Q et al (2011) The association of XPC polymorphisms and tea drinking with colorectal cancer risk in a Chinese population. Mol Carcinog 50:189–198
Berndt SI, Platz EA, Fallin MD, Thuita LW, Hoffman SC, Helzlsouer KJ (2006) Genetic variation in the nucleotide excision repair pathway and colorectal cancer risk. Cancer Epidemiol Biomark Prev 15(11):2263–2269
He J, Shi TY, Zhu ML, Wang MY, Li QX, Wei QY (2013) Associations of Lys939Gln and Ala499Val polymorphisms of the XPC gene with cancer susceptibility: a meta-analysis. Int J Cancer 133(8):1765–1775
Skjelbred CF, Sæbø M, Wallin H, Andersen B, Nexø BA, Hagen PC et al (2006) Polymorphisms of the XRCC1, XRCC3 and XPD genes and risk of colorectal adenoma and carcinoma, in a Norwegian cohort: a case control study. BMC Cancer 6:67
Gil J, Ramsey D, Stembalska A, Karpiński P, Pesz KA, Laczmańska I et al (2012) The C/A polymorphism in intron 11 of the XPC gene play a crucial role in the modulation of an individual’s susceptibility to sporadic colorectal cancer. Mol Biol Rep 39:527–534
Yeh C, Hsieh L, Tang R, Chang-Chieh CR, Sung F (2005) MS-920: DNA repair gene polymorphisms, diet and colorectal cancer risk in Taiwan. Cancer Lett 224:279–288
Engin AB, Karahalil B, Engin A, Karakaya AE (2010) Oxidative stress, Helicobacter pylori, and OGG1 Ser326Cys, XPC Lys939Gln, and XPD Lys751Gln polymorphisms in a Turkish population with colorectal carcinoma. Genet Test Mol Biomark 14(4):559–564
Zhang Y, Ding D, Wang X, Zhu Z, Huang M, He X (2011) Lack of association between XPD Lys751Gln and Asp312Asn polymorphisms and colorectal cancer risk: a meta-analysis of case-control studies. Int J Colorectal Dis 26:1257–1264
Stern MC, Conti DV, Siegmund KD, Corral R, Yuan J, Koh W et al (2007) DNA repair single-nucleotide polymorphisms in colorectal cancer and their role as modifiers of the effect of cigarette smoking and alcohol in the Singapore Chinese Health Study. Cancer Epidemiol Biomark Prev 16(11):2363–2372
Huang WY, Berndt SI, Kang D, Chatterjee N, Chanock SJ, Yeager M et al (2006) Nucleotide excision repair polymorphisms and risk of advanced colorectal adenoma: XPC polymorphisms modify smoking-related risk. Cancer Epidemiol Biomark Prev 15(2):306–311
Moreno V, Gemignani F, Landi S, Gioia-Patricola L, Chabrier A, Blanco I et al (2006) Polymorphisms in genes of nucleotide and base excision repair: risk and prognosis of colorectal cancer. Clin Cancer Res 12(7):2101–2108
Hansen RD, Sorensen M, Tjonneland A, Overvad K, Wallin H, Raaschou-Nielsen O et al (2007) XPA A23G, XPC Lys939Gln, XPD Lys751Gln and XPD Asp312Asn polymorphisms, interactions with smoking, alcohol and dietary factors, and risk of colorectal cancer. Mutat Res 619:68–80
Paszkowska-Szczur K, Scott RJ, Serrano-Fernandez P, Mirecka A, Gapska P, Górski B et al (2013) Xeroderma pigmentosum genes and melanoma risk. Int J Cancer 133(5):1094–1100
Riva A (2006–2011) CHIP Bioinformatics Tools. URL: http://snpper.chip.org/. Accessed 11 Nov 2014
Miller SA, Dykes DD, Polesky HF (1988) A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res 16:1215
Ott J (1988) Utility programs for analysis of genetic linkage; Program HWE. Columbia University, New york
R Development Core Team (2010) R: a language and environment for statistical computing 2010. R Foundation for Statistical Computing, Vienna
Sinnwell JP, Schaid DJ (2012) Statistical analysis of haplotypes with traits and covariates when linkage phase is ambiguous. http://mayoresearch.mayo.edu/mayo/research/schaid_lab/software.cfm/. Accessed 11 Nov 2014
Carter KW, McCaskie PA, Palmer LJ (2006) JLIN: a java based linkage disequilibrium plotter. Biomed Chromatogr Bioinformatics 7:60
Joshi AD, Corral R, Siegmund KD, Haile RW, Marchand LL, Martinez ME et al (2009) Red meat and poultry intake, polymorphisms in the nucleotide excision repair and mismatch repair pathways and colorectal cancer risk. Carcinogenesis 3(30):472–479
Jelonek K, Gdowicz-Kłosok A, Pietrowska M, Borkowska M, Korfanty J, Rzeszowska-Wolny J et al (2010) Association between single-nucleotide polymorphisms of selected genes involved in the response to DNA damage and risk of colon, head and neck, and breast cancers in a Polish population. J Appl Genet 51(3):343–352
Yeh C, Sung F, Tang R, Chang-Chieh CR, Hsieh L (2005) Polymorphisms of the XRCC1, XRCC3, & XPD genes, and colorectal cancer risk: a case-control study in Taiwan. BMC Cancer 5:12
Śliwiński T, Krupa R, Wiśniewska-Jarosińska M, Pawłowska E, Lech J, Chojnacki J et al (2009) Common polymorphisms In the XPD and hOGG1 genes are not associated with the risk of colorectal cancer in Polish population. Tohoku J Exp Med 218:175–181
Mort R, Mo L, McEwan C, Melton DW (2003) Lack of involvement of nucleotide excision repair gene polymorphisms in colorectal cancer. Br J Cancer 89:333–337
Acknowledgments
The study was partially funded by the National Centre of Research and Development in Poland-EUROSTARS project E!4292 MCCGTP ‘Multi-platform Colorectal Cancer genetic testing Portfolio’ and part-financed by the Polish Ministry of Science and Higher Education (MNiSW)-project number MB-158-79/13.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article

Cite this article
Paszkowska-Szczur, K., Scott, R.J., Górski, B. et al. Polymorphisms in nucleotide excision repair genes and susceptibility to colorectal cancer in the Polish population. Mol Biol Rep 42, 755–764 (2015). https://doi.org/10.1007/s11033-014-3824-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11033-014-3824-z