
Abstract
Spirituality and religion are well-documented components of prevention, treatment and recovery of substance use disorders. Faith communities are in a distinct position to support recovery and resilience regarding substance use disorders—not only in times of crisis, but every day. We conducted an exploratory study of congregational (i.e., organizational) “levers” that can drive change readiness in implementing recovery and resilience programming for substance use disorders within faith communities. Findings point to enhanced effectiveness post-intervention and the importance of developing awareness of resources to help with someone who has an alcohol or other drug problem.
Similar content being viewed by others


Background and Study Purpose
Spirituality and religion are well-documented and essential components of prevention, treatment, and recovery of substance use disorders (Beraldo et al., 2019; Grim & Grim, 2019; Walton-Moss et al., 2013). Religious beliefs, affiliation, and valuing spirituality are associated with lower propensity to engage in substance use across a range of studies and populations (e.g., Brown et al., 2013; Gorsuch, 1995; Leigh et al., 2005; Marsiglia et al., 2005). Among those in recovery, Pardini et al. (2000) found that faith (i.e., behaviors and beliefs associated with religion or spirituality) was associated with positive outcomes—including enhanced coping, resilience, sense of optimism, and social support as well as decreased anxiety.
Yet, people can be at a greater risk of substance use disorders during times of economic crises and upheaval (Bruguera et al., 2018). Experts have warned that the coronavirus (COVID-19) pandemic creates additional burdens and new challenges for those already struggling with substance use disorders (Clay, 2020; Panchal et al., 2020). Although the link between substance use and the COVID-19 fallout will be studied for years to come, existing research offers a guide. For example, in a systematic review, Nagelhout et al. (2017) found an upsurge in drug use during recessions due to the psychological strain that comes with unemployment.
Faith communities are in a distinct position to help individuals, families, and communities in supporting recovery and resilience of substance use disorders—particularly in times of crisis. Grim and Grim (2019) argued: “In addition to the efficacious role of spirituality, congregations and faith-based institutions are particularly effective in community mobilization and timely response to crises. Faith communities are adept at facilitating quality group interactions focused on overcoming past negative experiences, which are often drivers of the emotional and spiritual despondency that feed mental illness and substance abuse” (p. 1737).
Interventions that integrate faith-based components, such as 12-step programs, are evidenced to support those on their resilience and recovery journey (Dermatis & Galanter, 2016; Hennessy & Fisher, 2015; Lyons et al., 2010). Grim and Grim (2019) found that 73% of programs focused on treatment of addictions in the US have an embedded dimension of spirituality. Hai’s et al. (2019) systematic review and meta-analyses of interventions with an underpinning focus on spirituality or religion (excluding AA or twelve-step programs) demonstrated programmatic efficacy in supporting those with substance use challenges.
Notably, faith communities can play a pivotal role as facilitators of change not only in prevention efforts but also in widespread community and policy change. As an example, the Uniting Church in Australia engaged 60 partnering organizations to advocate for macro-level drug laws focusing on evidence-based strategies and targeting marginalized groups who are “hurting the most” (Fair Treatment, n.d.; Smyth & Porter, 2018).
Likewise, congregational programs offering support to those within marginalized communities are a vital resource. In a focus group study of barriers and facilitators to the involvement of African American congregations in providing HIV services in the Boston area, Teti et al. (2011) reported that a facilitating factor was the presence of preexisting faith-based HIV services in the community.
But, challenges exist. There can be undesirable outcomes for those navigating substance use problems or disorders and seeking help from the faith community when their congregation is not prepared to support an individual or group in need. Fallot (2007) detailed some adverse ways religion or spirituality can relate to individual well-being—particularly in situations when people may feel conflicted about their beliefs, express anger, and blame or question God or a higher power. In other situations, people can feel shame and rejection from their faith community or experience dissatisfaction with their congregation’s leadership. Researchers also provide insight on how all forms of stigma create or exacerbate obstacles to seeking help for people with substance use problems (Livingston et al., 2012; Wogen & Restrepo, 2020). For example, Jozaghi et al. (2016) found that sense of shame alongside stigma are barriers to engaging in mental health-seeking behaviors in Muslim faith communities. In a study of African American churches representing a range of denominations, Wong et al. (2018) found that 50% of churches identified individual embarrassment to receiving treatment as a top barrier for securing support for substance use disorders. In part, stigma and prejudice persists because substance use problems can erroneously be perceived as a personal or moral failure (e.g., lack of individual responsibility or willpower) rather than a health or medical issue that needs supportive services (Gutierrez et al., 2020). In some cases, this stigma is internalized by health professionals—adding complexity to the stigmas associated with substance use problems (Gutierrez et al., 2020).
Absent training, resources, and organizational investments, faith communities may struggle to effectively implement programming to address the complexity of needs of those (individuals and their support networks) facing substance use disorders. To minimize undesirable outcomes, congregations must develop approaches to drive change readiness over the long haul. This requires systematic training, development, and capacity building at the organizational (congregational) level to support recovery and resilience among congregants. We posit that by bolstering organizational levers for change, faith communities will be more likely to support recovery and resilience efforts. For this study, organizational levers for change are conceptualized as mechanisms to bolster change readiness to engage in addictions resilience and recovery support programming. In the present article, the term “substance use disorder” refers to a person's use of alcohol or another substance (drug) leading to health issues or problems at work, school, or home.
Unfortunately, research is limited in how best to support faith communities at the organizational level in their undertaking of this critical work. A gap exists in knowledge of specific levers that drive change in congregational readiness to address substance use disorders over time. To help close this gap, we sought to the following:
-
1.
Conduct an exploratory study of organizational “levers” (i.e., “congregational support levers”), which can drive change readiness in implementing substance use disorder recovery and resilience programming within faith communities.
-
2.
Examine which among these congregational support levers are the most powerful predictors of change readiness over time.
-
3.
Offer practical implications for driving change at the congregational (organizational) level.
Study Context
To achieve study goals, we employed an exploratory study of seven congregations across the United States who participated in Faith Partners’ congregational leadership development and training program and provided pre–post assessments. Faith Partners, a non-profit organization, specializes in developing and delivering extensive leadership development training to enhance the capacity of congregations to address substance use disorder recovery and resilience. Participating congregations collaborated with and were supported by Faith Partners for 18–24 months to enhance their change readiness. The Faith Partners model focuses on the following strategies:
-
Advance congregational leadership development and investment within formal and informal governance structures.
-
Develop team capacity leading to general awareness, educational platforms, and recovery support to address addiction and other related issues.
-
Sustain the ministry through ongoing planning, evaluation, training, resource development and networking.
-
Create innovative programming based on congregational needs, receptivity, capacity, and missional focus (e.g., discipleship, health, teaching, social justice).
-
Build infrastructure to create accountability systems that help sustain progress and commitment over time.
Conceptual Framework
With nearly 20.3 million people impacted by substance use disorders in the United States in 2018 (SAMHSA, 2019), communities face a sense of urgency to act. Our focus on levers for congregational readiness offers promise for advancing understanding of strategies to successfully implement addictions resilience and recovery support programming overtime within faith communities. We define congregational readiness as “a faith community’s intention and preparedness to address and support recovery from substance use disorders” (Travis et al., 2012, p. 2).
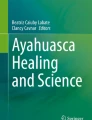
From a broad perspective, change processes are multi-layered, complex, and deemed a “critical precursor to successful implementation of complex changes in healthcare settings” (Weiner, 2009, para. 1). Figure 1 showcases our conceptual model—highlighting three congregational support levers that help drive congregational change readiness. We draw upon organizational and community change theories to inform this study’s conceptual model.

Congregational change readiness conceptual model
Unpacking Change Readiness
Diffusion of innovations theory (Rogers, 2003) provides a theoretical framework for congregational readiness because it explains the process of change from innovation through widespread adoption. Diffusion of innovation argues that full adoption of a change—particularly at the starting point of implementation—is a misnomer. Yet, people can expect 100% adoption. Instead, change takes time. Everyone will not adopt a change as soon it is implemented. By focusing solely on the lack of adoption, organizations will overlook clues or information about what works to drive change. Moreover, an ability to reinvent and adapt to a change requires a willingness to learn, assess failures, and collect ongoing feedback (Dearing & Cox, 2018). Through reinvention, change efforts are evaluated and progress is monitored. This allows opportunity to enhance the prospect of large-scale adoption over time. Adoptions are made by those implementing change who can gauge context and external environmental factors that can “make or break the sustained applicability of an innovation for improving health and health care” (Dearing & Cox, 2018, p. 188).
The Faith Partners Model embraces a diffusion approach in building readiness by centering congregational leadership development (i.e., innovators or early adopters) as a fundamental aspect of their intervention. Researchers have pointed to the critical role of leadership in change processes (Oetting et al., 2001; Thurman et al., 2003; Weiner, 2009). To expand adoption of the intervention, the program focuses on developing team capacity and sustaining the ministry. Lastly, programming and infrastructure are key focus areas. This process-based approach allows for learning from failures, seeking feedback, securing buy-in, and garnering support for widespread adoption over the long haul.
Proponents of the stages of change models tout that assessment is vital to ensuring a community or organization is sufficiently ready and equipped to institute a change effort (Oetting et al., 2001; Prochaska et al., 2001). Readiness assessments offer direction on the type of work ahead (Thurman et al., 2003). When not ready, Kostindinov et al. (2015) cautioned that organizations can run a risk of misdirecting or underutilizing its resources and capabilities. For example, Thurman et al. (2003, p. 29) shared that a “community may have a strong, stable program for drug abuse prevention, but…still be at the denial stage for utilizing the program or even accepting that they may need the program”, and in essence, setting the program up to fail or to not be utilized to its fullest capacity.
The Community Readiness Model (CRM)—Designed to address substance use prevention efforts (and since expanded to other types of interventions), CRM (Oetting et al., 2001; Thurman et al., 2003) involves tailoring an intervention to the needs, strengths, and challenges of a given community. Thurman et al. (2003) noted that to “increase an intervention’s chance of success, its introduction in a community must be consistent with the awareness of the problem and the level of readiness for change present [or existing] among members of that community” (p. 29). Hence, nine core CRM stages range from: (1) lack of awareness—current state is accepted as part of the status quo, (2) denial of a problem or a prevailing notion that change is not possible, (3) problem recognition exists but still limited motivation to change, (4) preplanning in which recognition of a problem is ignited, (5) preparation by exploring next steps, (6) initiation or implementation phases, (7) stabilization in which some efforts are up and running; (8) confirmation or expansion focuses on assessment of limitations and intervention refinement, and (9) professionalization or application of learnings to other community issues.
The Transtheoretical Model comprises five stages of change (Prochaska & DiClimente, 1986) applies to community (Oetting et al., 2001) and organizational settings (Prochaska et al., 2001). The basis of transtheoretical model focuses on movement from and among different stages–showcasing progression and helping change makers focus on how best to intervene along a continuum: (1) Precontemplation reflects an absence of inclination to change. (2) Contemplation is about knowing that change is needed but lacking a commitment to change. (3) Preparation comprises help-seeking processes. (4) Action involves taking steps toward implementing the change. (5) Lastly, maintenance involves stabilizing change. Although some noted challenges to transtheoretical model exist (West, 2005), critiques focus more so on individual behavioral change rather than organizational change.
What are Congregational Support Levers
Identifying congregational support levers as mechanisms to bolster change readiness is vital. Our model depicts three levers critical for a congregation’s readiness to engage in addictions resilience and recovery support programming:
-
VALUE: Ability to demonstrate the value or importance of engaging in efforts to addictions within its community.
-
RESOURCES: Ability to drive awareness of resources available for help.
-
COMMUNITY: Ability to create a supportive community and environment for addressing addictions.
The value or perceived importance of addressing addictions is a necessary condition to drive change readiness. Weiner (2009) suggested that the value placed on a change is, in part, derived from their change commitment or people’s emotional investment into implementing that change. Weiner also described the role of change valence—the extent to which people consider change is needed or valued—as core to change readiness. From a valence perspective, people must feel change is dire and that they can contribute. As a result, ensuring congregational members understand the importance of addressing addictions can be a key spark to enhance readiness. Evans and Loomis (2009) captured this sentiment, as follows:
Before any change effort can fully commence, there must be a clear recognition on the part of at least some key players that there is a local problem and that something should be done about it…This cannot happen when people have little to no awareness of the problem or deny that the problem even exists (p. 376).
Identifying and securing resources are common threads or aspects of change readiness. Anderson et al. (2002) defined community empowerment as an awareness-building process in which community members enhance their ability to collectively solve problems as well as gain understanding of their resources. This process is noted as particularly important in understanding and improving community health. In a similar vein, Al-Haddad and Kotnour (2015) posited that there are specific enablers of change which comprise organizational resources; knowledge, abilities, or competencies; and shared commitments. Batras et al. (2016) noted that resource identification and development are core to organizational capacity building—advancing the knowledge, support, or infrastructure needed for change implementation. Weiner (2009) discussed how the structure and resources embedded within an organization can help support change efficacy. Hence, the resources lever is key to movement within the stages of change. For example, generating awareness of resources available to help those in need may advance congregations from contemplation to preparation (Prochaska et al., 2001) or preplanning to preparation (Oetting et al., 2001).
Finally, having a supportive community or atmosphere for addressing addictions within a faith community is essential. This support can address social stigma barriers to progress in recovery. Persons in recovery may be negatively affected by stigma of a structural type as reflected in policies and practices that are barriers to participation in recovery programs, and by the language that is used to identify and characterize persons affected by substance use disorders (Wogen & Restrepo, 2020). A supportive community can help improve awareness of need for change given these types of stigma, which inhibit access and participation in services.
Chilenski et al. (2007) found that community attachment encourages people to collectively participate and get involved in realizing a goal. Evans and Loomis (2009) purported that a community’s shared belief and vision can contribute to creating change. This is because “communities possess capacity, skills, and assets that when recognized and utilized can serve as a springboard to action toward community change” (Anderson et al., 2002, p. 40).
Methods
Study Design
The current longitudinal study used mixed effects linear regression to examine predictors of seven U.S. faith-based congregations’ readiness to support recovery from substance use disorders. The Institutional Review Board at the University of Texas at Austin approved study protocols and procedures. The data were collected as part of a larger study evaluating the effectiveness of an 18- to 24-month leadership and congregation team ministry development program implemented by Faith Partners starting in 2007–2008 with a rolling enrollment. More information about the original study can be found in Travis et al. (2012).
Sampling and Data Collection
A convenience sample of congregations were surveyed over two time points—baseline and 24 months after participation in the Faith Partners program. Members from forty-five congregations completed the Congregational Readiness Questionnaire pretest survey (n = 3,649), while members at fourteen congregations completed the posttest survey (n = 1,284). Sixteen congregations also completed a detailed questionnaire about their program participation and engagement (i.e. project checklist). This study focused on the seven faith-based congregations where all three measures (i.e., pretest, posttest, and project checklist) were completed (n = 1205).
To protect the anonymity of members, personal identifying information was not collected on any congregation member. Because of the importance of anonymity for this population, members were not tracked from pre- to posttest. Thus, the data focus on congregations that have data for all three measures regardless if the same individuals completed the pre- and posttest. This limitation is given more attention in the discussion.
Surveys were distributed to participants upon the congregation’s enrollment into the program and after completion of the program using various methods. The most common methods included distribution during weekly worship services and small group activities, as well as distributed in membership mailings. Surveys were collected by the congregation and returned to the investigators at a university research center.
Description of Study Sample
Table 1 provides information on the demographics of the study sample. The seven congregations included in this study were of United Methodist, Episcopal, and Jewish faith tradition, with the majority (67%) being United Methodists. Three regions of the United States were represented: Western, Southeastern and South Central, with most of the representation from the South Central states (43%). The ages of congregation members varied, with almost a third (28%) of the sample being age 65 or older. The majority of respondents were women (57%). Fifty-nine percent of the sample chose not to provide information on their racial/ethnic background and among those that did provide this information, 35% were white (Table 2).
Instrumentation
The 24-item Congregational Readiness Questionnaire was developed specifically for this study as part of the Faith Partners’ program. The questionnaire was developed in consultation with experts from two university-based addictions research and behavioral health centers.
The pretest survey was originally used as a needs assessment to understand the perceptions of congregational members regarding the prevalence of substance use disorders and addiction problems; receptiveness to awareness, education and recovery support activities; and willingness to support or get involved with the ministry. The posttest survey was modified to capture further information on congregations’ recovery support activities.
Despite these shifts from pretest to posttest, both versions of the congregational survey includes congregation characteristics, member demographic characteristics, perception of congregation supportiveness of addiction-related problems, member experiences with addiction-related problems, and congregational readiness to help those with alcohol or drug problems.
Independent Variables
Demographic Variables
Faith tradition (United Methodist, Episcopal, and Jewish) and geographic region (Western, Southeastern and South Central) were collected for each congregation. More faith traditions and regions were targeted; however, the convenience sampling resulted in surveys from congregations belonging to these faith traditions and regions only.
Congregational Support Levers (CSLs)
Three variables captured at pre- and posttest were included as independent variables based on their alignment with understanding how various forms of congregational (or organizational-level) support (perceived importance, awareness of resources, supportive community) predict a congregations’ change in readiness to support recovery from substance use disorders. These variables are expressions of
-
1.
Perceived value or importance of the role of congregations in addressing addictions—The survey assessed members’ beliefs on the importance that the faith community helps those with addictions to alcohol and/or drugs. A scale was used to reflect the average of the following two items: “How important is it for the faith community to help those who may have problems with alcohol or drugs?” and “How important is it for our congregation to help those who may have problems with alcohol or drugs?” Response options included: 0, “I don’t know”; 1, “not at all”; 2, “not too important”; 3, “somewhat important”; and 4, “very important”. The Cronbach’s alpha on this scale was 0.86. The resulting variable (i.e., average of the two questions) will be referred to as VALUE.
-
2.
Knowledge of helpful resources—The survey captured members’ knowledge of supportive resources within the congregation or community with regard to handling addiction-related issues. This was captured using a dichotomous variable (yes, aware; no, unaware) based on answering yes to at least one of the following two questions: “Do you know who to go to in the congregation to get help for someone who has an alcohol, drug or other addiction?” and “Do you know who to go to in the community to get help for someone who has an alcohol, drug or other addiction?” The resulting variable (i.e., yes to at least one question) will be referred to as RESOURCES.
-
3.
Supportive Community—One’s perception of the supportiveness of their congregation’s environment with regard to handling addiction-related issues was captured using a seven-item scale specifically created for this survey. Each item asked respondents to indicate the extent to which one’s congregation engages in several activities geared toward creating a supportive environment for addressing alcohol and drug problems. Example items include: To what extent does our congregation…reach out to people who suffer from addiction, provide space for recovery support groups such as Alcoholics Anonymous, Al-anon, and Alateen, and sponsor programs to help spouses talk to one another about alcohol. Response choices were scored on a 5-point scale. Response options included: 0, “I don’t know”; 1, “to no extent”; 2, “to a lesser extent”; 3, “to some extent”; and 4, “to a great extent.” The scores for items were averaged to create one measure for knowledge of supportive resources. The Cronbach’s alpha on this scale was 0.92. The resulting variable (i.e., average of the seven items) will be referred to as COMMUNITY.
Dependent Variable
Congregational readiness was measured by a single question: “Overall, how ready is our congregation to help those who have alcohol or drug problems?” Response options included: 0, “I don’t know”; 1, “not at all ready”; 2, “not too ready”; 3, “somewhat ready”; and 4, “very ready.” This item was developed specifically for this project to assess organizational readiness for change in a faith community. The measurement of interest is the change in organizational readiness from time 1 to time 2 after participation in the Faith Partners program.
Data Analysis
First, descriptive statistics were computed for all demographics and major study variables (Table 1). Second, an independent samples t test was conducted to determine if there was an increase in congregational readiness from time 1 to time 2. Third, mixed effects linear regression, using a random intercept for congregation (level-2 factor), were fit to assess the unique role of the CSLs on change in readiness to support recovery from substance use disorders post-program participation. For the mixed effects linear regressions, we first tested a main effects model with readiness to support recovery from substance use disorders as the dependent variable, a time variable as a covariate to differentiate between pre- and posttest response, CSLs, and demographic variables in the model. Three separate follow-up analyses were conducted using the same main effects model as above, with the addition of a single interaction variable consisting of one CSL and the time variable. Interactions were probed by comparing marginal means (i.e., the values predicted from the models) for specific values of the independent variables (Aiken & West, 1991; Rogosa, 1980, 1981). For RESOURCES, the dichotomous CSL, the two possible values were 0 and 1. For the continuous CSLs, we followed recommendations from Cohen and Cohen (1983) and used values at 1 standard deviation above and below the mean for COMMUNITY and VALUE. For example, we examined the change in congregational readiness for people who felt that the congregation was offering a high (1 standard deviation above the mean) amount of addiction-related activities (COMMUNITY) at time 1 and 2, and separately we examined the change in congregational readiness for people who felt that the congregation was offering a low (1 standard deviation below the mean) amount of addiction related activities (COMMUNITY) at time 1 and 2. A p value < 0.05 was considered statistically significant. All statistical analyses were conducted using SPSS version 25.
Results
A t test indicated there was a significant difference in the scores for congregational readiness at time 1 (M = 1.59, SD = 1.42) and time 2 (M = 2.11, SD = 1.56); t(1098) = − 5.83, p < 0.001. Among those who completed the survey at time 1, almost 68% had knowledge of supportive resources in the congregation or community with regard to handling addiction-related issues (RESOURCES), compared to 72% among those at time 2. The mean score for perception of the supportiveness of the congregation’s environment with regard to handling addiction-related issues (COMMUNITY) and perception of the importance that the faith community help those with addictions to alcohol and/or drugs (VALUE) at time 1 was 1.47 (SD = 1.22) and 3.62 (SD = 0.68), respectively. The mean score for COMMUNITY and VALUE at time 2 was 1.90 (SD = 1.23) and 3.73 (SD = 0.55), respectively.
Main effects for the mixed effects linear regression model indicated that RESOURCES (B = 0.40, 95% CI: 0.23, 0.56), COMMUNITY (B = 0.64, 95% CI: 0.58, 0.71), and VALUE (B = 0.18, 95% CI: 0.06, 0.29) were significant predictors of higher congregational readiness score.
-
Answering yes to RESOURCES predicted a higher readiness score compared to those who answered no; on average, participants who said yes to having knowledge of supportive resources in the congregation or community with regard to handling addiction-related issues (RESOURCES) had a 0.40 higher congregational readiness score, compared to those who said no, controlling for all other variables.
-
A higher COMMUNITY score predicted a higher readiness score; a one unit increase in participants’ perception of the supportiveness of their congregation’s environment with regard to handling addiction-related issues (COMMUNITY) was associated with a 0.64 higher congregational readiness score, controlling for all other variables.
-
A higher VALUE score predicted a higher readiness score; a one unit increase in participants’ perception of the importance that the faith community helps those with addictions to alcohol and/or drugs (VALUE) was associated with a 0.18 higher congregational readiness score, controlling for all other variables.
The intraclass correlation coefficient for the null model was 0.04. There was more variation within congregations (2.20) than between congregations (0.09). We also tested whether models 2 (AIC = 3516.99), 3 (AIC = 3520.58), and 4 (AIC = 3519.30) fit better than model 1 (AIC = 3519.26) based on -2LL chi-square tests and none of the tests resulted in a significant difference. Almost none of the total variation in congregational readiness can be accounted for by which congregation each congregant was in. Random effects analyses resulted in no significant variability among congregations (0.004, 95% CI: < 0.001, 212.82).
Follow-up analyses examining interactions between each CSL and time resulted in a significant interaction between time and RESOURCES (B = 0.34, 95% CI: 0.005, 0.67). We further probed this significant interaction with two contrasts: The first examined the change in congregational readiness score between time 1 and time 2 where RESOURCES was “yes”; the second examined the change in congregational readiness score between time 1 and time 2 for where RESOURCES was “no”. The follow-up analyses resulted in a statistically significant difference in congregational readiness score among those who said yes to RESOURCES at time 1 and time 2. The marginal mean congregational readiness score where RESOURCES was “yes” at time 1 and time 2 was 1.75 (SD = 0.08) and 2.06 (SD = 0.08), respectively. On average, there was a 0.31 (95% CI: 0.13, 0.48) change in congregational readiness score for those who said yes to RESOURCES at time 1 and time 2.
Discussion
Study findings illuminate the role of capacity building (via resources, knowledge, and value) in enhancing congregational readiness to provide resilience and recovery support programming for those dealing with substance use problems or disorders. Yet, everyday challenges pervade. All types of stigma (e.g., structural, public, and individual) can interfere with the care for substance use disorders along a continuum such as access, treatment, or retention as well as can diminish one’s sense of dignity (Wogen & Restrepo, 2020). Also, faith communities, nor are its congregants, are “one size fits all.” Therefore, capacity building interventions need to be mindful of the cultural context and the unique challenges faced within marginalized communities or groups.
In addition, some faith communities provide support to prevention programs intended to increase resilience and reduce risk for substance use disorders. There are also addiction treatment and peer support programs supported by churches and synagogues. However, these efforts are small compared to the vastness of the larger faith community in terms of available social and material resources and potential opportunity for expansion of prevention, treatment, and recovery support activities.
In order to expand the number of faith communities actively involved in supporting resilience to and recovery from substance use disorders, more knowledge is needed regarding effective methods to recruit these congregations to become engaged in deliberate programming focused on building capacity and change readiness to address substance use disorders. The present analysis is intended to use a convenience sample of congregations whose leaders have been recruited to participate in a leadership training and awareness intervention. It is hoped that the data obtained from this sample may provide suggestions for refining and testing intervention components that may have increased effectiveness to enhance congregational readiness.
Increasing the willingness of congregations to engage in supporting addiction recovery is a central goal for the Faith Partners program. The present study suggests that congregational willingness can be expected to improve after participation in the intervention. This is an important finding that supports the value of the program.
Furthermore, the findings point to several intervention "levers" which may enhance the effectiveness of the program. Results indicate that congregational willingness may increase in association with an intervention that addresses several covariates.
The primary covariate is congregational awareness of resources people currently in the congregation can use to help with someone who has an alcohol or other drug problem.
In terms of stages of change, this may mean that some people who have been pre-contemplators (Dearing & Cox, 2018) have been encouraged by their participation in the Faith Partners program to consider supporting addiction recovery activities. Persuasion tools may include increased awareness that there are already other congregants who are helping people in recovery, and that the congregation has a number of services in place to provide recovery support.
Diffusion of innovations theory posits several attributes of innovations that influence rapidity of diffusion. One key attribute is that of compatibility as defined by the degree to which the innovation is perceived to be consistent with community values and needs (Rogers, 2003). The RESOURCES and COMMUNITY variables are directly related to consistency with congregational values, and the VALUE variable addresses perceived congregational need. Thus, the influence of the three covariates of the study support may be explained in part by the diffusion of innovations theory.
Based on these findings, the intervention group may focus on pre-contemplators who are not yet thinking seriously about committing to be involved, or are ambivalent about joining in. These are not the innovators or early adopters who only need information and knowledge to get on board. The pre-contemplators are people who are candidates to be early majority or late majority adopters who need persuasion and social reassurance in order to participate. The social reassurance may, for example, take the form of promotional activities to increase awareness of existing congregational recovery support resources and community prevention activities, as well as testimonials from members who endorse congregational engagement in the program. By doing so, faith communities can enhance opportunities to engage leaders and build their capacity to address recovery and resiliency from substance use disorders in a way that address their unique challenges and galvanizes support in the long run.
Study Limitations
A primary weakness of the study is its focus on an organizational intervention using only a small number of organizations. Another weakness is that we were not able to track participants from time 1 to time 2, which is why we conducted an independent samples t test. The data are drawn from organizational (congregational) members as individuals without regard to organizational differences. In fact, organizational variance with regard to location and religious affiliation was found to be nonsignificant. Finally, data have potential limitations based on the timing collected. Yet, given the difficulty in studying congregational communities in the real world, and the lack of knowledge about methods of increasing social support for addictions programming in faith communities, the present analysis is undertaken as a beginning effort to examine intervention tools that may be effective in this work, and to suggest hypotheses for follow-up studies.
Conclusion and Future Directions
Study findings indicate that enhancing organizational-level capacity as levers for change can spur congregational readiness for resilience and recovery support programming to address challenges of those struggling with substance use problems. But while our current study speaks to the importance of capacity building and readiness within faith communities, more research is needed. It is important to not only document, examine, and evaluate how congregational readiness can support behavior change. Critical research questions must be answered that focus on how behavior change, in turn, can have an impact on those struggling with substance use disorders or problems. To address these questions, there is a need for current and ongoing data collection and research to be undertaken with appropriate financial support and resources to translate findings to action.
Faith Partners' work will continue in this space, particularly in evaluations of its programmatic efforts. And we encourage researchers, policy makers, and community leaders to engage in partnerships and research to build, test, or enhance interventions that have potential to make a meaningful difference in the longer term for addictions resilience and recovery for those in need.
References
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing and interpreting interactions. Thousand Oaks: SAGE Publications.
Al-Haddad, S., & Kotnour, T. (2015). Integrating the organizational change literature: A model for successful change. Journal of Organizational Change Management, 28(2), 234–262.
Anderson, D., Guthrie, T., & Schirle, R. (2002). A nursing model of community organization for change. Public Health Nursing, 19(1), 40–46.
Batras, D., Duff, C., & Smith, B. J. (2016). Organizational change theory: Implications for health promotion practice. Health Promotion International, 31(1), 231–241.
Beraldo, L., Gil, F., Ventriglio, A., de Andrade, A. G., da Silva, A. G., Torales, J., et al. (2019). Spirituality, religiosity and addiction recovery: Current perspectives. Current Drug Research Reviews Formerly: Current Drug Abuse Reviews, 11(1), 26–32.
Brown, A. E., Tonigan, J. S., Pavlik, V. N., Kosten, T. R., & Volk, R. J. (2013). Spirituality and confidence to resist substance use among celebrate recovery participants. Journal of Religion and Health, 52(1), 107–113.
Bruguera, P., Reynolds, J., Gilvarry, E., Braddick, F., Marath-Veettil, A. L., Anderson, P., Mielecka-Kubien, Z., Kaner, E., & Gual, A. (2018). How does economic recession affect substance use? A reality check with clients of drug treatment centres. The Journal of Mental Health Policy and Economics, 21(1), 11–16.
Chilenski, S. M., Greenberg, M. T., & Feinberg, M. E. (2007). Community readiness as a multidimensional construct. Journal of Community Psychology, 35(3), 347–365.
Clay, R. A. (2020, April 15). Advice for treating and preventing substance use during COVID-19. Washington, DC: American Psychological Association. https://www.apa.org/topics/covid-19/substance-use
Cohen, J., & Cohen, P. (1983). Applied multiple regression/correlation analysis for the behavioral sciences. Erlbaum.
Dearing, J. W., & Cox, J. G. (2018). Diffusion of innovations theory, principles, and practice. Health Affairs, 37(2), 183–190.
Dermatis, H., & Galanter, M. (2016). The role of twelve-step-related spirituality in addiction recovery. Journal of Religion and Health, 55(2), 510–521.
Evans, S. D., & Loomis, C. (2009). Organizational and community change. In D. Fox, I. Prilleltensky, & S. Austin (Eds.), Critical psychologically: An introduction (2nd ed., pp. 373–390). SAGE Publications.
Fallot, R. D. (2007). Spirituality and religion in recovery: Some current issues. Psychiatric Rehabilitation Journal, 30(4), 261–270.
Fair Treatment.(n.d.). ‘We want fair treatment’. Uniting Church in Australia, Synod of New South Wales and Australian Capital Territory. Retrieved November 23, 2020, from https://www.fairtreatment.org/.
Gorsuch, R. L. (1995). Religious aspects of substance abuse and recovery. Journal of Social Issues, 51(2), 65–83.
Grim, B. J., & Grim, M. E. (2019). Belief, behavior, and belonging: How faith is indispensable in preventing and recovering from substance abuse. Journal of Religion and Health, 58, 1713–1750.
Gutierrez, D., Crowe, A., Mullen, P. R., Pignato, L., & Fan, S. (2020). Stigma, help seeking, and substance use. Professional Counselor, 10(2), 220–234.
Hai, A. H., Franklin, C., Park, S., DiNitto, D. M., & Aurelio, N. (2019). The efficacy of spiritual/religious interventions for substance use problems: A systematic review and meta-analysis of randomized controlled trials. Drug and Alcohol Dependence, 202, 134–148.
Hennessy, E. A., & Fisher, B. W. (2015). A meta-analysis exploring the relationship between 12-Step attendance and adolescent substance use relapse. Journal of Groups in Addiction & Recovery, 10(1), 79–96.
Jozaghi, E., Asadullah, M., & Dahya, A. (2016). The role of Muslim faith-based programs in transforming the lives of people suffering with mental health and addiction problems. Journal of Substance Use, 21(6), 587–593.
Kostadinov, I., Daniel, M., Stanley, L., Gancia, A., & Cargo, M. (2015). A systematic review of community readiness tool applications: Implications for reporting. International Journal of Environmental Research and Public Health, 12(4), 3453–3468.
Leigh, J., Bowen, S., & Marlatt, G. A. (2005). Spirituality, mindfulness and substance abuse. Addictive Behaviors, 30(7), 1335–1341.
Livingston, J. D., Milne, T., Fang, M. L., & Amari, E. (2012). The effectiveness of interventions for reducing stigma related to substance use disorders: A systematic review. Addiction, 107(1), 39–50.
Lyons, G. C., Deane, F. P., & Kelly, P. J. (2010). Forgiveness and purpose in life as spiritual mechanisms of recovery from substance use disorders. Addiction Research and Theory, 18(5), 528–543.
Marsiglia, F. F., Kulis, S., Nieri, T., & Parsai, M. (2005). God forbid! Substance use among religious and non-religious youth. The American Journal of Orthopsychiatry, 75(4), 585–598.
Nagelhout, G. E., Hummel, K., de Goeij, M. C., de Vries, H., Kaner, E., & Lemmens, P. (2017). How economic recessions and unemployment affect illegal drug use: A systematic realist literature review. International Journal of Drug Policy, 44, 69–83.
Oetting, E. R., Jumper-Thurman, P., Plested, B., & Edwards, R. W. (2001). Community readiness and health services. Substance Use & Misuse, 36(6–7), 825–843.
Panchal, N., Kamal, R., Orgera, K., Cox, C., Garfield, R., Hamel, L., Muñana, C., & Chidambaram, P. (2020, August 21). The Implications of COVID-19 for Mental Health and Substance Use. KFF. https://www.kff.org/coronavirus-covid-19/issue-brief/the-implications-of-covid-19-for-mental-health-and-substance-use/
Pardini, D. A., Plante, T. G., Sherman, A., & Stump, J. E. (2000). Religious faith and spirituality in substance abuse recovery: Determining the mental health benefits. Journal of Substance Abuse Treatment, 19(4), 347–354.
Prochaska, J. O., & DiClemente, C. C. (1986). Toward a comprehensive model of change. In W. R. Miller & N. Heather (Eds.), Treating addictive behaviors (pp. 3–27). Springer.
Prochaska, J. M., Prochaska, J. O., & Levesque, D. A. (2001). A transtheoretical approach to changing organizations. Administration and Policy in Mental Health and Mental Health Services Research, 28(4), 247–261.
Rogers, E. M. (2003). Diffusion of innovations. (5th ed.). New York: Free Press.
Rogosa, D. (1980). Comparing nonparallel regression lines. Psychological Bulletin, 88(2), 307–321.
Rogosa, D. (1981). On the relationship between the Johnson–Neyman region of significance and statistical tests of parallel within-group regressions. Educational and Psychological Measurement, 41(1), 73–84.
Smyth, K. & Porter, S. (2018). Fair Treatment: Why We Need to Change Our Approach to People Who Need Treatment. https://fairtreatment.org/wp-content/uploads/2019/08/FT_DOCV2.pdf
Substance Abuse and Mental Health Services Administration (SAMHSA). (2019). Key substance use and mental health indicators in the United States: Results from the 2018 National Survey on Drug Use and Health (HHS Publication No. PEP19–5068, NSDUH Series H-54). Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/
Teti, M., Drainoni, M., Raj, A., Cozier, Y., Harris, C., Bright, D., & Welles, S. L. (2011). Barriers and facilitators to providing HIV-related services in Bostononian African-American churches: A focus group study of clergy and community members. Journal of HIV/AIDS & Social Services, 10(4), 345–362.
Thurman, P. J., Plested, B. A., Edwards, R. W., Foley, R., & Burnside, M. (2003). Community readiness: The journey to community healing. Journal of Psychoactive Drugs, 35(1), 27–31.
Travis, D. J., Learman, J. A., Brooks, D., Merrill, T., & Spence, R. T. (2012). The faith community, substance abuse, and readiness for change: A national study. Journal of Social Service Research, 38(2), 231–247.
Walton-Moss, B., Ray, E. M., & Woodruff, K. (2013). Relationship of spirituality or religion to recovery from substance abuse: A systematic review. Journal of Addictions Nursing, 24(4), 217–226.
Weiner, B. J. (2009). A theory of organizational readiness for change. Implementation Science. https://doi.org/10.1186/1748-5908-4-67.
West, R. (2005). Time for a change: Putting the Transtheoretical (Stages of Change) Model to rest. Addiction, 100(8), 1036–1039.
Wogen, J., & Restrepo, M. T. (2020). Human rights, stigma, and substance use. Health and Human Rights, 22(1), 51.
Wong, E. C., Derose, K. P., Litt, P., & Miles, J. N. (2018). Sources of care for alcohol and other drug problems: The role of the African American church. Journal of Religion and Health, 57(4), 1200–1210.
Funding
A university-based institutional review board of record approved all study protocols. The initial project was funded by the Substance Abuse and Mental Health Services Administration/Center for Substance Abuse Prevention (Grant 280-02-0602) through a contract with Faith Partners Inc.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Travis, D.J., Vazquez, C.E., Spence, R. et al. Faith Communities’ Improvements in Readiness to Engage in Addictions Resilience and Recovery Support Programming. J Relig Health 60, 3931–3948 (2021). https://doi.org/10.1007/s10943-021-01235-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-021-01235-4