
Abstract
Purpose Employers are important stakeholders in the return to work (RTW) of employees with cancer. However, it is unclear what employer actions are most important to that process. The objective, therefore, was to reach consensus on what employer actions are considered most important for the RTW of employees with cancer, by employers and employees separately. Methods A two-round online Delphi study was conducted with two expert panels: one with 23 employers and one with 29 employees with cancer. The results from each panel were analysed separately. Out of 24 suggested employer actions, participants selected the 10 they considered most important for RTW in each of the following RTW phases: (1) disclosure, (2) treatment, (3) RTW plan, and (4) actual RTW. The consensus threshold was set at ≥ 80% during the second round. Results The employer and employee expert panels both reached consensus on the importance of ‘emotional support’, ‘practical support’, ‘allow sufficient sick leave’, ‘plan return to work’, ‘adjust expectations’, ‘assess work ability’, and ‘show appreciation’. Employers also reached consensus on ‘communicate’ and ‘treat normally’, and employees on ‘handle unpredictability’. All these employer actions were considered to be specific for one to three RTW phases. Conclusions Employers reached consensus on the importance of nine employer actions, employees on eight. Both stakeholder perspectives showed great similarities, but did vary regarding important employer actions during the employee’s treatment. We recommend developing interventions targeting the employer, meeting both employer and employee needs in each RTW phase, to enhance RTW support for employees with cancer.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
The current worldwide incidence of cancer is 14.1 million and this number is expected to increase to an annual 25 million new diagnoses in 2025 [1, 2]. Approximately 50% of those diagnosed with cancer are of working age [3]. This percentage also likely to increase considerably, mainly due to the trend of employees having to work longer before reaching retirement age, while the incidence of cancer is the highest in the 65–69 age group [4]. The increased incidence rates in the working population in combination with improved survival rates imply that employees who return to work (RTW) or continue working after a cancer diagnosis are becoming more common in workplaces [5]. For these employees with cancer, participating in work is an important step forward towards a ‘normal life’, since work provides structure, the feeling of social belonging and financial security [6, 7]. However, various problems related to the employee’s workplace and mental, physical and (psycho)social functioning may impede the work participation of employees with cancer, such as fatigue, depression, problems with physical tasks and a lack of support from the workplace [6, 8,9,10,11]. On average, only 62% of employees with cancer have returned to work or are still working 1 year after diagnosis [12]. Facilitating work participation of employees with cancer is therefore an increasingly relevant topic.
Although several stakeholders can facilitate work participation of employees with cancer, attention has lately been drawn to the role of the employer during the RTW process [13,14,15,16]. The employer is designated as one of the main stakeholders since a supportive employer has been found to be a key facilitator of work participation by employees with cancer [17]. However, a recent review showed that both employees with cancer and employers perceive a plurality of barriers for work participation of employees with cancer related to the employer, e.g. employer–employee communication, employer’s knowledge about cancer and employer’s perception of the employee’s ability to work [18]. The variety of these perceived employer-related barriers indicates that being a supportive employer of employees with cancer is not straightforward. Rather, the employer has a complex and demanding role to play during the RTW process, may face different ways of influencing RTW and indicate a need for support [18, 19].
Current evidence on the role of the employer during the RTW of employees with cancer is mainly obtained by qualitative studies, and perspectives are wide and sometimes even contradictory [17, 18]. However, knowledge on what employer actions are considered most important to facilitate the RTW of employees with cancer is scarce and only descriptive in nature [20]. Ordering such actions by their perceived importance is of great relevance—among other things, in order to gain an insight into which employer actions should be prioritised in future RTW interventions targeting employers. Moreover, based on a recent qualitative study on the role of the employer during RTW of an employee with cancer [19], the RTW trajectory of employees with cancer can generally be divided into four phases: (1) disclosure, (2) treatment, (3) RTW planning, and (4) actual RTW. If we can determine what employer actions are considered most important during each of these phases, we may be able to intervene on the employers’ RTW support for employees with cancer, and thereby contribute to a sustainable work participation of employees with cancer.
The objective of this study was therefore to reach consensus on what employer actions are considered most important for the RTW of employees with cancer. The viewpoints of both employees with cancer and employers are of interest, since any differences between the two perspectives would have important implications for practice. The current study therefore mapped each perspective separately, resulting in the following research questions: what employer actions are considered most important for the RTW of employees with cancer, according to (a) employees with cancer and (b) employers?
Methods
Design
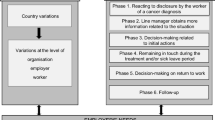
The Delphi technique was used, with a preparatory round and then two Delphi rounds, 1 and 2. The preparatory round was performed by the research team on the basis of a recent systematic review [18], whilst both Delphi rounds were each performed by two expert panels (see Fig. 1). This design was defined a priori and contained four important characteristics of the Delphi technique: experts participated in the Delphi rounds ‘anonymously’; the design contained ‘iterations’ of Delphi rounds (i.e. Delphi round 1 and 2); experts were provided with ‘controlled feedback’ of group responses; and ‘statistical group responses’ were analysed [21]. As such, the design was used to obtain consensus on which employer actions are considered as most important for the RTW of employees with cancer, by two expert panels separately. The Qualtrics online questionnaire system (http://www.qualtrics.com) was used and data was analysed using SPSS software (IBM SPSS Statistics version 24).

Design of the Delphi study, consisting of a preparatory round and two Delphi rounds, 1 and 2
Expert Panels
Employers
The inclusion criteria for the employer expert panel were that employers had been responsible for guiding at least one employee with cancer in the past 5 years (e.g., as HR manager or supervisor) and were able to speak and read Dutch. Employers were recruited via employers’ organisations, databases of employers who have participated in previous research [19, 22], social media and snowballing techniques. We strove for a heterogeneous panel in respect of gender, company size and function (supervisors, HR personnel and other employer representatives).
Employees with Cancer
For the employee expert panel, the inclusion criteria were that employees had been diagnosed with cancer in the past 7 years, were over 18 years of age at time of diagnosis, worked for an employer (either part-time or full-time, on a flexible, temporary or permanent basis) at time of diagnosis and were able to speak and read Dutch. A heterogeneous (gender and diagnosis) group of employees with cancer was purposefully sampled using a database of previous research [23]. In addition, we strove for heterogeneity in respect of company size and RTW outcomes.
We aimed to have 16 experts on each expert panel during the second Delphi round, as recommended for Delphi studies with a similar aim [24, 25]. Taking into account an expected 20% loss of follow-up after the first round, we included experts until 20 experts per expert panel filled out the first Delphi round, with no cut-off point in inclusion time. Experts were recruited in April–May 2017. Before inclusion, all experts received information about the study from the first author, both online and by telephone, and signed an online informed consent form.
Procedure
Preparatory Round
During this round, a list of employer actions was compiled based on a recent systematic review [18]. Consisting of 47 qualitative studies conducted from the perspective of employees with cancer and five from the employer perspective, this review identified perceived employer-related barriers and facilitators for work participation of employees with cancer. It applied the following definitions of a ‘barrier’ and a ‘facilitator’: behaviour, attitude and perception of the employer that was perceived to hinder (barrier) or enhance (facilitator) sustainable work participation of cancer survivors (p. 726). The first author (MG) openly coded the barriers and facilitators, resulting in several broad categories (e.g. ‘communication’, ‘practical support’ and ‘colleagues’). Subsequently, one concrete employer action per category was formulated, including a brief explanation which reflected the essence of all the barriers and facilitators in that specific category (e.g. ‘communicate: communicate effectively with the employee with cancer, in terms of tone, intensity, subjects and channels’). Next, the second author (ST) checked these first two steps. Finally, all the authors checked the complete list of employer actions, including the accompanying explanations, in respect of formulation (clear and consistent) and whether each action was indeed a concrete employer action. This process resulted in a list of 24 employer actions, which was used as input for Delphi round 1.
Delphi Round 1
In this first Delphi round, the experts’ demographic and work-related characteristics were recorded. Then the four RTW phases were addressed in turn.
Phase 1, Disclosure
The period between disclosure of the employee’s illness to the employer and the first treatment.
Phase 2, Treatment
The period during which the employee is on sick leave as a result of their treatment.
Phase 3, RTW Planning
The period in which concrete planning of and preparation for the employee’s RTW take place. The employee is still on sick leave during this phase.
Phase 4, Actual RTW
The period after RTW, up until 6 months after a stable work situation is reached. With ‘stable’ we refer to unchanged working hours and position at work.
These RTW phases were based on a recent qualitative study concerning the role of the employer in case an employee is diagnosed with cancer and adapted by more strict definition of the phases in consultation with all authors [19]. The period of 6 months for phase 4 was meant to make the experts aware that phase 4 was not only the moment of re-entering work, but also included a certain period of follow-up. Each phase was introduced in brief, after which the experts were asked whether they could recognise themselves in that phase. If so, the 24 employer actions were displayed in random order and the experts were asked to select the 10 they considered ‘most important for successful guidance focused on RTW’. If not, this expert was not asked to select the most important employer actions for this RTW phase and was thereby not taken along in the analysis of this RTW phase. This was done for each RTW phase separately. After each phase presentation, the experts who selected important employer actions were given the opportunity to add additional employer actions. The questionnaire of this Delphi round was pilot tested in respect of its formulation and use by four persons with a diverse level of education (low to high level of education), two of them were employees with cancer. Feedback was gathered by a telephone or face-to-face interview. Based on these pilot tests, some sentences and terminology were simplified and the experts were given the opportunity to add comments at the end of the Delphi round. The experts were asked to fill out the questionnaire of Delphi round 1 within a week, and if necessary received an e-mail and telephone reminder after 1 and 2 weeks respectively. Data collection of Delphi round 1 took place in April–May 2017.
After all experts participated in the first Delphi round, the percentage selecting a certain employer action as ‘most important’ was calculated separately for each expert panel and each RTW phase. This percentage was calculated to determine the ‘controlled feedback’ for the second Delphi round and to identify the employer actions which were selected as ‘most important’ by the highest percentage of experts. Since the purpose of Delphi round 1 was not to reach consensus among the experts, no criteria for consensus were defined for this round. In addition, four authors (MG, ST, MFD and AdB) decided by consensus whether or not to include the additional suggested actions in Delphi round 2. This decision was based on the following criteria: an included additional action indeed had to be an employer action and had to be one not already covered by any of the other actions.
Delphi Round 2
The 15 employer actions selected as ‘most important’ by the highest percentage of experts during the first Delphi round were included in the second Delphi round, together with additional actions that met the above criteria. The number of 15 actions was determined by the research team a priori, with the intention to incorporate a workable number of actions in the second Delphi round, without losing a sizeable range of options. In the second Delphi round, the employer actions were displayed in descending order and the percentage of experts who had selected each of them during the first round was shown (‘controlled feedback’). The questionnaire of Delphi round 2 was pilot tested by the same persons who pilot tested the questionnaire of Delphi round 1, but that exercise produced no major changes. Data was collected in May–June 2017. In this period, the experts were once again asked to select the 10 employer actions they considered ‘most important for successful guidance focused on RTW’. During the second Delphi round, experts could not add additional employer actions. All other methods for data collection were similar to the methods used for Delphi round 1.
The same procedure for data analysis was used as after the first Delphi round, with separate calculations for each RTW phase and each expert panel. Consensus was reached when ≥ 80% of the expert panel selected a certain employer action as ‘most important’ during a specific RTW phase. The research team decided a priori that two Delphi rounds were enough for the experts to make a considerate selection of the employer actions. The rationale behind this decision was that experts were given the opportunity to add additional employer actions (during Delphi round 1), were provided with controlled feedback of group responses (during Delphi round 2) and were given the opportunity to select any additional employer actions that were suggested by other experts (during Delphi round 2). Moreover, a small number of additional added employer actions during Delphi round 1 were expected, since the list of employer actions that was used as input for this round was expected to be fairly complete due to its comprehensive basis.
Results
Expert Panels
Employers
Twenty-three employers participated in the study (see Table 1), with 22 taking part in all rounds. Employers were recruited via employer’s organisations (n = 9), previous research (n = 5) [19, 22], social media (n = 1) or snowballing (n = 6). One did not answer the question about how he was recruited for the study. The employers had an average of 11 years of experience in guiding employees with cancer and collectively had worked with about 150 employees with cancer. Heterogeneity was reached in terms of gender and function, but most of the experts worked at medium-sized or large companies (≥ 51 employees). During the second Delphi round, all the employers indicated that they recognised themselves in all the RTW phases, with the exception of one and two who did not recognise themselves in phases 3 and 4, respectively, because the employees they had guided were ultimately unable to plan or achieve their RTW.
Employees with Cancer
A heterogeneous group of 29 employees completed both Delphi rounds (100% response rate). Most had been diagnosed with breast cancer (n = 9), gastro intestinal cancer (n = 6) or bladder cancer (n = 5) (see Table 2). The employees scored the guidance they had received from their employer with 3.8 ± 1.4 (1–5) on a scale of 1 (‘completely dissatisfied’) to 5 (‘completely satisfied’). During the second Delphi round, 90% recognised themselves in RTW phase 1 (disclosure), 90% in phase 2 (treatment), 86% in phase 3 (RTW planning) and 90% in phase 4 (actual RTW). The reasons cited for not identifying with a certain phase were that the employee was ‘diagnosed very suddenly and treated the same day’ (phase 1), ‘worked throughout the treatment’ (phase 2 and 3), and ‘has still not returned to work’ (phase 4). The number of employees that were included for analysis per RTW phase can be found in Table 3.
Selection of Employer Actions
Employers
During Delphi round 1, the employers suggested a total of 14 additional employer actions across the four RTW phases. One additional action for RTW phases 1 and 4 met the criteria for inclusion in Delphi round 2: ‘support relationship with direct supervisor’ (see “Appendix”). The other actions were either not considered as an employer action (n = 1: ‘... the employee himself owns his work and its absence and is deemed to act from that perspective’) or already covered by another employer action (n = 11, e.g., ‘keep in touch with the employee when he or she is absent for operations and treatments’, which was covered by the employer action: ‘communicate’). These actions were therefore not included in Delphi round 2.
Consensus was reached on the importance of nine different employer actions, divided over all four RTW phases (and with some included in more than one phase): three in phase 1, disclosure (‘practical support’, ‘communicate’ and ‘emotional support’); four in phase 2, treatment (‘communicate’, ‘emotional support’, ‘allow sufficient sick leave’ and ‘plan return to work’); five in phase 3, RTW planning (‘assess work ability’, ‘communicate’, ‘adjust expectations’, ‘plan return to work’ and ‘show appreciation’); and five in phase 4, actual RTW (‘practical support’, ‘treat normally’, ‘assess work ability’, ‘show appreciation’ and ‘plan return to work’). See also Table 3.
Employees with Cancer
Eleven additional employer actions were suggested during Delphi round 1. Six of these were not considered as an employer action (e.g., ‘good advice and coaching from the occupational physician’) and five were already covered by another employer action (e.g., ‘ongoing communication about how the employee is doing personally and at work’, which was covered by the employer action ‘communicate’).
The employees with cancer reached consensus on the importance of eight different employer actions across the four RTW phases: four in phase 1, disclosure (‘allow sufficient sick leave’, ‘practical support’, ‘assess work ability’ and ‘emotional support’); two in phase 2, treatment (‘allow sufficient sick leave’ and ‘handle unpredictability’); five in phase 3, RTW planning (‘practical support’, ‘assess work ability’, ‘show appreciation’, ‘plan return to work’ and ‘adjust expectations’); and three in phase 4, actual RTW (‘practical support’, ‘assess work ability’ and ‘show appreciation’). See also Table 3.
Discussion
The aim of this study was to reach consensus on which employer actions are considered most important for the RTW of employees with cancer. In this two-round Delphi study, employers reached consensus on the importance of nine employer actions: ‘emotional support’, ‘communicate’, ‘practical support’, ‘allow sufficient sick leave’, ‘plan return to work’, ‘adjust expectations’, ‘assess work ability’, ‘show appreciation’ and ‘treat normally’. Employees with cancer reached consensus on the importance of eight employer actions: ‘emotional support’, ‘allow sufficient sick leave’, ‘practical support’, ‘assess work ability’, ‘handle unpredictability’, ‘plan return to work’, ‘adjust expectations’, and ‘show appreciation’.
Comparison with the Literature
Both stakeholder groups showed great similarity regarding perceptions of important employer actions for the RTW of employees with cancer and reached consensus on the importance of seven corresponding employer actions. For example, both agreed on the importance of emotional support during the first RTW phase, employer appreciation during the later phases, making a plan for the RTW in consultation with the employee during phase 3 and practical support during phases 1 and 4. These finding are in line with a recent qualitative study with breast cancer survivors on supporting practices of their employers, in which the importance of preparing a structured RTW before the actual RTW and the importance of flexible working hours (i.e. practical support) after RTW were mentioned [20]. Similar results were also found in a qualitative study concerning supervisor actions during the RTW of employees on sick leave due to depression [26]. This study found that emotional support, giving recognition and providing assistance (i.e. practical support) were among the most implemented employer actions to facilitate the RTW [26]. Interestingly, neither employers nor employees with cancer selected ‘possess of seek knowledge of cancer’ among the most important employer actions in the current study, even though previous studies have found repeatedly that employers do need a certain amount of knowledge of cancer in order to manage the RTW of employees with cancer [18, 19, 27]. Another study on the RTW of mixed populations also found knowledge of the consequences of the employee’s sickness for their work to be among the most important supervisor competencies [28]. That knowledge on cancer was not among the most important employer actions in the current study may be due to the high level of experience of the employers taking part: experienced employers might undervalue its importance because, for them, a certain amount of cancer-related knowledge might be ‘normal’. Whether less experienced employers would select knowledge of cancer as one of the most important employer actions and if so, what specific knowledge these employers need to facilitate the RTW of employees with cancer, should therefore be subject of further research.
Some interesting differences between stakeholder perceptions were also found, especially with regard to the phase in which the employee is on sick leave as a result of their treatment (RTW phase 2). Employers selected communicating effectively and making a RTW plan as important employer actions, whereas employees agreed on the importance of an employer being able to cope with the unpredictability of the illness. This indicates that employers might be one step ahead of the employee at this stage, a finding also substantiated by previous studies. For example, employees on sick leave with cancer might still feel vulnerable, uncertain about their mental and physical ability to work and sensitive to contact with their employer [29, 30], whereas employers are already trying to manage the absence and expected return to work of the employee [31, 32]. The discrepancy between these two perspectives could put effective employee–employer collaboration at risk. Since previous studies have perceived collaboration between the two parties as a pre-requisite for a successful RTW [30, 33], mutual understanding of their respective perspectives could well be crucial to facilitate the RTW of employees with cancer. For this reason, it is recommended that both stakeholders be open: employees with cancer about their uncertainties and needs regarding RTW, and employers about their need to be updated about the employee’s situation in order to manage the absence of the employee. For this, employers might benefit from communication skills training, since such training for employees with cancer was perceived to be helpful to enhance communication in the workplace [34]. We therefore recommend to provide employers with communication skills training to improve employer–employee communication and collaboration, with the aim of enhancing RTW of employees with cancer.
Other previous studies have shown that employers feel uncertain about what actions are required to facilitate the RTW of employees with cancer [19, 35]. Although the employers included in this study did reach consensus on the importance of a number of actions, perspectives were different for the majority of actions. This is in line with a previous study which found that organisational culture and the characteristics of both the employer and the employee might influence perceptions concerning facilitating employer actions [19]. The influence of employee characteristics was also discerned in the current study, since a certain variance was found in the selection of important employer actions by the employees with cancer, especially during RTW phase 2. This variance may be the result of differences between the employees in terms of their diagnosis and treatment [36] and in how they experience their illness and being work disabled—differences which might affect their support needs from the employer [37]. It is therefore recommended that employers be aware of the full range of actions which might facilitate the RTW of employees with cancer and tailor their use to the needs and preferences of the individual employee.
Strengths and Limitations
The strength of the current study is its inclusion of the perspectives of both employees with cancer and employers, as well as the fact that it draws a distinction between the different RTW phases. This enhances the practical utility of the results. Secondly, the level of flexibility provided by the Delphi technique and the absence of strict guidelines resulted in a study design tailored to the current status of international research and in line with the aims of the study, e.g. with a preparatory round and concerning the predefined consensus threshold [38]. Thirdly, the participating employers had ample experience guiding employees with cancer, in terms of both years (11 on average) and numbers (about 150 in total), which contributed to the external validity of the outcomes. Finally, the heterogeneity of the employees and employers taking part also contributed to the external validity of the findings.
Some limitations should also be taken into consideration. Firstly, although the number of experts per panel was in accordance with the Delphi guidelines [25], the study’s statistical power might not be adequate to be sure that the 80% consensus threshold was not reached by chance and thereby to generalise the results to a larger population. We therefore suggest increasing the recommended number of experts per panel in order to enhance the statistical substantiality of future Delphi studies. Secondly, despite the considered process used to define the employer actions, some participants noticed a certain amount of overlap between certain actions (e.g. between ‘adjust expectation’ and ‘reduce work pressure’), which may have influenced their selection and thereby the internal validity of the findings. Thirdly, the number of actions included per RTW phase in the second Delphi round ranged between 15 and 18, due to the inclusion of additional suggested actions and a shared 15th position—the cut-off point for inclusion—in the first Delphi round. Since the experts had to select a fixed number of actions, 10, including more of these in the second Delphi round increased the number of possible permutation and so reduced the chance of reaching the ≥80% consensus threshold. Finally, two limitations might have influenced the external validity of the findings. Firstly, although we strived for heterogeneity on company size, the employers included hardly worked at small companies. The underrepresentation of small sized companies, which has also been noticed for international research at large [39], may have affected the outcomes of the current study. Large sized companies may have resources not available at smaller companies [39], for example an occupational physician to ‘assess the work ability’ of an employee with cancer, which might have resulted in an underestimation of the importance of these employer actions in this study. Besides, in the Netherlands some employer actions are required by law and this may have influenced the selection and hence the external validity of the findings for countries with different legislation. For example, Dutch employers are obliged to cover the employee’s income for at least 2 years [40]. This may be why few participants in this study selected financial support as an important employer action, whereas that might be a more relevant employer action in countries with fewer employer-related obligations from the social security system.
Recommendations for Future Research and Practice
We recommend to study international variations in perceptions of important employer actions for the RTW of employees with cancer, since these perceptions may be influenced by national and organisational policies. With regard to practice, we recommend developing interventions that facilitate employers to perform the most important employer actions, e.g. information about appropriate practical support and assistance in assessing the work ability of an employee with cancer. These interventions should meet both employer and employee needs, so as to enhance RTW support for employees with cancer. It is also recommended that future RTW interventions draw a distinction between the four RTW phases presented in the current study, since the selection of important employer actions differed between these four phases. These differences confirm the existence of the different RTW phases and imply that each phase requires a specific approach from the employer. For phase 4, a period up until 6 months after reaching a stable situation was chosen. We do not expect that participants would have selected other employer actions when we would have chosen a longer period of follow-up. However, further research should confirm this. Lastly, some employers mentioned that they missed a fifth phase: when RTW is not possible due to the employee’s health or for organisational reasons. This phase was also identified in a recent qualitative study among employers [19], but was omitted from this study because it fell outside its particular scope, namely the return to work of employees with cancer. However, we still recommend the study of important employer actions during this fifth phase, since knowledge of what to do at this stage lacks and employers have mentioned to experience this as stressful phase [19].
Conclusions
The current study ordered the wide range of findings from international qualitative studies on the role of the employer during the RTW of employees with cancer into consensus on the importance of a number of concrete employer actions in different RTW phases. Employers reached consensus on the importance of nine employer actions, employees with cancer on eight. Although the two stakeholders’ perspectives on important employer actions showed great similarities, with consensus on seven corresponding employer actions, perspectives did vary when it came to important actions while the employee is on sick leave as a result of their treatment. The results can be used to develop interventions targeting the employer, with the aim of enhancing their RTW support for employees with cancer throughout the different RTW phases. These interventions should meet both employer and employee needs, and should also incorporate a certain amount of flexibility since the employee perspectives concerning important employer actions were not univocal during all the RTW phases.
References
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–E386.
Bray F, Soerjomataram I. The changing global burden of cancer: transitions in human development and implications for cancer prevention and control. In: Gelband H, Jha P, Sankaranarayanan R, Horton S, editors. Cancer: disease control priorities, 3rd ed. (vol 3). Washington (DC): World Bank; 2015
Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, Rosso S, Coebergh JW, Comber H, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013;49(6):1374–1403.
UK Cr. Cancer incidence by age. http://www.cancerresearchuk.org/health-professional/cancer-statistics/incidence/age#heading-Zero (2016). Accessed 1 Aug 2017.
Society AC cancer facts & figs. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2017/cancer-facts-and-figures-2017.pdf (2017).
de Boer AG, Taskila TK, Tamminga SJ, Feuerstein M, Frings-Dresen MH, Verbeek JH. Interventions to enhance return-to-work for cancer patients. Cochrane Database Syst Rev. 2015. https://doi.org/10.1002/14651858.CD007569.pub2.
Stergiou-Kita M, Grigorovich A, Tseung V, Milosevic E, Hebert D, Phan S, et al. Qualitative meta-synthesis of survivors’ work experiences and the development of strategies to facilitate return to work. J Cancer Surviv. 2014;8(4):657–670.
Duijts SF, van Egmond MP, Spelten E, van Muijen P, Anema JR, van der Beek AJ. Physical and psychosocial problems in cancer survivors beyond return to work: a systematic review. Psychooncology. 2014;23(5):481–492.
Steiner JF, Nowels CT, Main DS. Returning to work after cancer: quantitative studies and prototypical narratives. Psychooncology. 2010;19(2):115–124.
Cheung K, Ching SYS, Chan A, Cheung D, Cheung SYP. The impact of personal-, disease- and work-related factors on work ability of women with breast cancer living in the community: a cross-sectional survey study. Support Care Cancer. 2017;25(11):3495–3504.
Bijker R, Duijts SFA, Smith SN, de Wildt-Liesveld R, Anema JR, Regeer BJ. Functional impairments and work-related outcomes in breast cancer survivors: a systematic review. J Occup Rehabil. 2017. https://doi.org/10.1007/s10926-017-9736-8
Mehnert A, de Boer A, Feuerstein M. Employment challenges for cancer survivors. Cancer. 2013;119(Suppl 11):2151–2159.
de Boer AG. The European cancer and work network: CANWON. J Occup Rehabil. 2014;24(3):393–398.
Nilsson M, Olsson M, Wennman-Larsen A, Petersson LM, Alexanderson K. Return to work after breast cancer: women’s experiences of encounters with different stakeholders. Eur J Oncol Nurs. 2011;15(3):267–274.
Tiedtke C, Donceel P, Knops L, Desiron H, Dierckx de Casterle B, de Rijk A. Supporting return-to-work in the face of legislation: stakeholders’ experiences with return-to-work after breast cancer in Belgium. J Occup Rehabil. 2012;22(2):241–251.
Young AE, Wasiak R, Roessler RT, McPherson KM, Anema JR, van Poppel MN. Return-to-work outcomes following work disability: stakeholder motivations, interests and concerns. J Occup Rehabil. 2005;15(4):543–556.
Islam T, Dahlui M, Majid HA, Nahar AM, Mohd Taib NA, Su TT, et al. Factors associated with return to work of breast cancer survivors: a systematic review. BMC Public Health. 2014;14(Suppl 3):S8.
Greidanus MA, de Boer A, de Rijk AE, Tiedtke CM, Dierckx de Casterle B, Frings-Dresen MHW, et al. Perceived employer-related barriers and facilitators for work participation of cancer survivors: a systematic review of employers’ and survivors’ perspectives. Psychooncology. 2018;27(3):725–733.
Tiedtke CM, Dierckx de Casterle B, Frings-Dresen MHW, De Boer A, Greidanus MA, Tamminga SJ, et al. Employers’ experience of employees with cancer: trajectories of complex communication. J Cancer Surviv. 2017;11(5):562–577.
Caron M, Durand MJ, Tremblay D. Perceptions of breast cancer survivors on the supporting practices of their supervisors in the return-to-work process: a qualitative descriptive study. J Occup Rehabil. 2018;28(1):89–96.
von der Gracht HA. Consensus measurement in Delphi studies Review and implications for future quality assurance. Technol Forecast Soc Chang. 2012;79(8):1525–1536.
de Jong M, Tamminga SJ, de Boer AG, Frings-Dresen MH. Quality of working life of cancer survivors: development of a cancer-specific questionnaire. J Cancer Surviv. 2016;10(2):394–405.
de Jong M, Tamminga SJ, Frings-Dresen MH, de Boer AG. Quality of working life of cancer survivors: associations with health- and work-related variables. Support Care Cancer. 2017;25(5):1475–1484.
Diamond IR, Grant RC, Feldman BM, Pencharz PB, Ling SC, Moore AM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. 2014;67(4):401–409.
Okoli C, Pawlowski SD. The Delphi method as a research tool: an example, design considerations and applications. Inform Manag. 2004;42(1):15–29.
Negrini A, Corbiere M, Lecomte T, Coutu MF, Nieuwenhuijsen K, St-Arnaud L, et al. How can supervisors contribute to the return to work of employees who have experienced depression? J Occup Rehabil. 2017;28(2):279–288.
Tamminga SJ, van Hezel S, de Boer AG, Frings-Dresen MH. Enhancing the return to work of cancer survivors: development and feasibility of the nurse-led ehealth intervention cancer@work. JMIR Res Protoc. 2016;5(2):e118.
Johnston V, Way K, Long MH, Wyatt M, Gibson L, Shaw WS. Supervisor competencies for supporting return to work: a mixed-methods study. J Occup Rehabil. 2015;25(1):3–17.
Tiedtke C, Dierckx de Casterle B, Donceel P, de Rijk A. Workplace support after breast cancer treatment: recognition of vulnerability. Disabil Rehabil. 2015;37(19):1770–1776.
Amir Z, Neary D, Luker K. Cancer survivors’ views of work 3 years post diagnosis: a UK perspective. Eur J Oncol Nurs. 2008;12(3):190–197.
McKay G, Knott V, Delfabbro P. Return to work and cancer: the Australian experience. J Occup Rehabil. 2013;23(1):93–105.
Tiedtke C, Donceel P, de Rijk A, Dierckx de Casterle B. Return to work following breast cancer treatment: the employers’ side. J Occup Rehabil. 2014;24(3):399–409.
Stochkendahl MJ, Myburgh C, Young AE, Hartvigsen J. Manager experiences with the return to work process in a large, publically funded, hospital setting: walking a fine line. J Occup Rehabil. 2015;25(4):752–762.
Brown RF, Owens M, Bradley C. Employee to employer communication skills: balancing cancer treatment and employment. Psychooncology. 2013;22(2):426–433.
Amir Z, Wynn P, Chan F, Strauser D, Whitaker S, Luker K. Return to work after cancer in the UK: attitudes and experiences of line managers. J Occup Rehabil. 2010;20(4):435–442.
Taskila T, Lindbohm ML, Martikainen R, Lehto US, Hakanen J, Hietanen P. Cancer survivors’ received and needed social support from their work place and the occupational health services. Support Care Cancer. 2006;14(5):427–435.
Tiedtke C, Dierckx de Casterle B, de Rijk A, Christiaens MR, Donceel P. Breast cancer treatment and work disability: patient perspectives. Breast. 2011;20(6):534–538.
Rowe G, Wright G. The Delphi technique: Past, present, and future prospects—introduction to the special issue. Technol Forecast Soc Chang. 2011;78(9):1487–1490.
Kristman VL, Shaw WS, Boot CR, Delclos GL, Sullivan MJ, Ehrhart MG, et al. Researching complex and multi-level workplace factors affecting disability and prolonged sickness absence. J Occup Rehabil. 2016;26(4):399–416.
Hoefsmit N, de Rijk A, Houkes I. Work resumption at the price of distrust: a qualitative study on return to work legislation in the Netherlands. BMC Public Health. 2013;13(1):153.
Acknowledgements
Sponsor: Dutch Cancer Society (Grant No. UVA 2014-7153). The authors would like to thank all participants for their time.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
M.A. Greidanus, S.J. Tamminga, A.E. de Rijk, M.H.W. Frings-Dresen and A.G.E.M. de Boer declare that they have no conflict of interest.
Ethical Approval
Ethic approval was deemed not necessary by the Medical Ethics Review Committee of the Academic Medical Center (Reference Number W17_124). Though, all procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Before being included in the study, informed consent was obtained from all participants.
Appendix
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Greidanus, M.A., Tamminga, S.J., de Rijk, A.E. et al. What Employer Actions Are Considered Most Important for the Return to Work of Employees with Cancer? A Delphi Study Among Employees and Employers. J Occup Rehabil 29, 406–422 (2019). https://doi.org/10.1007/s10926-018-9800-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10926-018-9800-z