
Abstract
Our goal was to identify strategies aimed at increasing Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) enrollment and participation rates. The WIC program provides many health benefits for pregnant women, mothers, and children. WIC offers nutrition education, formula, fruits and vegetables, and other food to pregnant and postpartum women and their children until they reach the age of five. Despite the availability of this program nationwide, enrollment and participation rates remain low across the country. Several states have tried various interventions to combat this deficiency of engagement with the goal of increasing WIC enrollment and participation. We conducted a scoping review to identify articles based on pre-specified inclusion and exclusion criteria. Two reviewers independently identified and screened articles. Subsequently, three reviewers independently extracted study details and outcomes related to WIC enrollment and participation rate changes. We included 14 studies reporting on 12 interventions from 3945 citations reviewed. Seven of these were published papers, while the others were final reports of USDA WIC Special Grant Projects. All the observed interventions had some success increasing WIC participation. Virtual interventions demonstrated the most success based on preliminary evidence. Successful interventions showed percentage gains in enrollment close to 8% and changes in participation over 9%. Overall, the literature surrounding WIC enrollment interventions reveal a mixed impact on improving participation. Many successful interventions involve an online or virtual engagement component which can provide educational resources on WIC benefits, nutrition, and living a healthy lifestyle.
Similar content being viewed by others

Introduction
The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) was piloted by the United States Department of Agriculture in 1972 to provide nutrition for at-risk, low-income pregnant and postpartum women, infants, and children up to the age of five [1]. The WIC food package, which eligible families may receive in addition to the broader Supplemental Nutrition Assistance Program (SNAP), has extensive health and lifestyle benefits for both mothers and children. Participation in WIC leads to fewer nutrient deficiencies, reduced cases of obesity, and increased healthcare access for mothers [2, 3]. For infants and preschoolers, participation in WIC is associated with cognitive and academic development, a better-quality diet, and reduces the likelihood of a premature or low birthweight birth [4,5,6]. WIC is associated with a $100 reduction in Medicaid costs per newborn [7]
Despite all of these benefits, fewer than half of WIC-eligible families receive WIC nutrition benefits [8]. Though the program is proven to be extremely beneficial, participation continues to fall each year, due to a variety of reasons including food package inflexibility, lack of fruit and vegetable funds, stigma using Electronic Benefit Transfer (EBT) cards, troubling finding WIC-approved products in stores, and fear of taking benefits away from families in greater need [9, 10]. Multiple studies have been conducted to determine why people do not take part in WIC. Informed by input from researchers and the greater WIC community, several states have tried programs to raise their enrollment and participation rates.
The aim of this study is to investigate what types of strategies to increase WIC enrollment and participation have been tested and what resulted. This scoping review will provide guidance to help make recommendations to improve policy, provide guidance for state and local WIC initiatives, and/or to identify areas for future research.
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Review (PRISMA-ScR) guidelines to ensure methodological and reporting quality.
Step 1: Identify the Research Question
One author (R.A.D.) conducted a rapid review of the existing literature to refine the research question. A preliminary search of MEDLINE, the Cochrane Database of Systematic Reviews, and Google Scholar was conducted and no current or underway systematic reviews or scoping reviews on the topic were identified.
Eligibility Criteria
Eligible published literature was defined using the following inclusion criteria: (1) Participants were enrolled in WIC or eligible for WIC or those providing WIC foods, such as grocery store owners, or physicians (2) Studies that looked at an intervention to increase WIC enrollment or WIC participation (3) Studies that took place within the United States. Gray literature was also included in this review.
Reports from prior to 2009 were excluded as WIC released a new food package that year. Interventions that were not yet implemented or did not provide outcome results were excluded from the review. We only included grants that have published final reports in order to chronicle a complete dataset.
A scoping review was selected for this study as it facilitates a broad review of WIC initiatives across the country to summarize attempts and results. We used Arksey and O’Malley’s original scoping review methodology to guide our research and used their recommended customizations to enhance our approach [11].
Step 2: Identify Relevant Studies
In collaboration with a research librarian, we developed and executed a comprehensive search strategy on 06/07/2022. The strategy was registered through OSF (#uq2eh). See Appendix I for full details of search strategy.
Search Strategy
The search strategy aimed to locate both published and unpublished studies. An initial limited search of MEDLINE Pubmed, SCOPUS, Web of Science, Cochrane Libraries, and gray literature were undertaken to identify articles on the topic.
We explored keywords such as “Food Assistance”, “WIC Programs”, “Special Supplemental Nutrition Program for Women, Infants, and Children (U.S.)”, and “Participation.” We used the Boolean term “AND” to combine themes and the term “OR” to search within themes. The only limit we imposed was that the studies must evaluate WIC after 2008, since a new WIC food program was implemented in 2009. Studies in all languages were included.
The search strategy, including all identified keywords and index terms, was adapted for each included database and/or information source. The reference list of all included sources of evidence were screened for additional studies. The databases searched included MEDLINE Pubmed, SCOPUS, Web of Science, Cochrane Libraries, and gray literature. Sources of unpublished studies/ gray literature were searched for through Google Scholar.
Step 3: Study Selection
Following the search, all identified citations were collated and uploaded into Endnote and duplicates removed. The remaining studies were then uploaded into a new Rayaan review [12]. Following a pilot test, titles and abstracts were then screened by two (R.A.D. and H.B.L.) blinded, independent reviewers for assessment against the inclusion criteria for the review. At the abstract review stage, studies were kept if they included an implementation and evaluation of a WIC engagement intervention. Potentially relevant sources were retrieved in full. The full text of selected citations was assessed in detail against the inclusion criteria by two (R.A.D. and H.B.L.) blinded, independent reviewers. Any disagreements that arose between the reviewers at each stage of the selection process were resolved through discussion, or with input from an additional reviewer (M.C.).
Step 4: Charting the Data
Data Extraction
Data was independently extracted from papers included in the scoping review by our team using a data extraction tool (Appendix II). The data extracted included specific details about the participants, context, intervention goals, methods, and key findings relevant to the review questions. The data extraction form was created in accordance with the TIDieR guidelines [13]. Any disagreements that arose between the reviewers were resolved through discussion. Authors of papers were contacted to request missing or additional data where required. We did not formally assess the risk of bias in included studies or outcomes.
Step 5: Collecting, Summarizing, and Reporting Results
Data Analysis and Presentation
The extracted data was tabulated and summarized. A descriptive narrative has been used to present the findings.
Results
Selection of Sources and Relevant Evidence
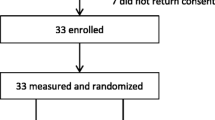
A total of 3,945 entries were loaded into Rayyan, and their titles and abstracts were subsequently reviewed (Fig. 1). 1151 duplicates were removed. After the primary review, we identified 30 citations for full text review. We excluded 23 citations after our secondary screen and identified 7 citations meeting our inclusion criteria. Two of those studies described the same initiative, so we combined their information for our results. An additional 7 studies were identified by reviewing the United States Department of Agriculture WIC Special Project Grant history, giving us a final list of 14 included articles [1]. One of these additional studies is another reporting of one of the included studies, so we reported these results together to reduce repetition.

PRISMA flow diagram
Characteristics of Implemented Interventions
Of the six studies included in the initial keyword search, two spanned the United States and four occurred in single states exclusively; for details see Table 1. Though the overarching goals of these interventions were to increase usage of WIC funds, some of the programs were designed to target specific areas such as fruit and vegetable redemption or farmer’s market allowances redeemed. The studies varied in ways to measure WIC enrollment and participation, including the number of people enrolled in WIC, voucher redemption rates, fruit and vegetable intake, and program reach. Three of the studies were targeted interventions while three of the studies examined data from external changes to the WIC program to assess the impact on enrollment and participation.
Intervention Impact on WIC Enrollment and Participation
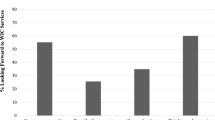
All the examined interventions had a positive impact on WIC participation (Table 2). The two studies that measured online versus offline benefits showed that participants had a clear preference for the online system [14, 15]. Offline benefits provided a check or voucher to WIC participants for them to bring to local supermarkets to redeem. In 2020, all states were required to switch to eWIC, or electronic benefit transfer (EBT), which replaced paper vouchers with a card [16]. There was approximately an 8% change in both studies between online and offline states. The various educational initiatives, including WIC Fresh Start, CRUNCH, and shopping orientation all resulted in increased participation, though CRUNCH was the only program to report statistical significance [17,18,19,20]. While the non-participants only redeemed 39% of Farmer’s Market Nutrition Program checks, those receiving the intervention redeemed 46.5% of their checks (P < 0.001) [17]. Nationwide, the redemption rate is a mere 60%, suggesting a need for continued attempts to increase redemption rates [21].
Characteristics of WIC Special Project Grants
The Food and Nutrition Service department of the United States Department of Agriculture provides funding “to test innovative projects that have the potential to improve and enhance the WIC program” [1]. Many of the yearly grants, provided on a competitive basis, align with our inclusion criteria of studies that increase WIC enrollment and participation. This resulted in seven projects that fit our inclusion criteria (Table 3). These projects spanned ideas such as cooking classes, texting reminders, and community partnerships. Some states, like Washington, dispersed their grant funds to several different WIC sites and nonprofit operations across the state to encourage many smaller experiments.
Outcomes of WIC Special Project Grants
There were mixed results among Special Grant Projects, though all reported some form of success. One main issue among several projects was staff turnover and lack of continuity of project activities. Of the six grants we analyzed, four had “mixed” results and two reported higher success metrics. The Massachusetts grant found that there was gap in addressing the social needs of prospective or current participants. This gap was alleviated by the incorporation of a Family Support Coordinator to connect social and welfare services to WIC participants, which increased the WIC child retention rate. The most successful project was observed to be the Colorado Texting for Retention Program texting service. Within this project, the group that had the best outcomes was the “augmented innovation” group that received additional educational texts about WIC beyond just appointment reminders. One of the twelve sites in Washington reported positive statistically significant results, which the report attributed to the fact that the program was offered year-round while the other sites only provided summer offerings.
Discussion
This review is the first to examine a variety of interventions to increase WIC enrollment and participation and compare their impact. Despite the different approaches and outcomes of the studies, we observed that simplicity is one key to increasing WIC enrollment and participation across the country. We observed that single faceted programs that focused on direct and simple interventions saw higher success in increasing WIC enrollment and participation across the country.
While conducting this review, we also examined the barriers that impacted WIC enrollment and participation. Administrative barriers were common in discouraging WIC participants from engaging with programs. These barriers include discovering eligibility criteria, paperwork and gathering documentation, time and inconvenience of registering for services, and stressors that come from interacting with government programs [22]. One article discussed administrative barriers fall into three sub categories: the learning costs of finding out about a program’s existence and benefits, the compliance costs of filling out forms, and the psychological costs, such as stress, frustration, and anxiety, that arise from interacting with these programs. These listed barriers can limit access to other government and social service programs, and decrease participation and enrollment rates resulting in health harming effects [22]. Other barriers include physical access to WIC services, stigma associated with redemptions, and lack of knowledge about redemption qualifications.
In addition to studies with outcome data included in our scoping review, several additional strategies proposed by WIC offices across the United States have been implemented over the past 20 years. One popular strategy across many states is data sharing, where SNAP and Medicaid registries are shared with WIC offices to encourage mothers to take advantage of multiple assistance programs [23]. The Jewish Health Foundation investigated best practices by states with the highest WIC enrollment and participation, Maryland and California, and found that linking with other services and support beyond nutritional and breastfeeding topics, were offered in these successful areas [24]. WIC offices partnered with other areas of government, such as childcare (i.e. HeadStart), to programs for mothers, like domestic violence or addition support groups, to increase the usefulness of continued enrollment in WIC [24]. Some states like Maryland enacted policy changes that allowed a short term, one-month, WIC certification if a family cannot produce all the required documents right away. This “trial period” may allow families to become familiar with WIC and experience the benefits before needing to put in the effort to continuously stay engaged. In terms of overcoming the confusion in-store when shopping for WIC, some states positioned WIC clinics adjacent to grocery stores that specialize in WIC offerings to guide families toward WIC products. Pennsylvania and Maryland took advantage of a mobile WIC app that allowed participants to test whether items qualify by scanning food barcodes. Many states have tried various forms of outreach to reach participants, from social media advertisements, to local television and radio slots, to placing marketing materials at physicians’ offices, churches, and other community organizations [25]. One creative idea Colorado WIC tried was sending out a card promoting the benefits of WIC on a child’s first birthday to encourage the caregiver to continue participation even after the baby moves away from formula [25]. These efforts, especially those that attempt to modernize and streamline the WIC enrollment process, appear to be designed with participants in mind and will hopefully produce increased participation.
Administrative burdens such as cross-organization communication, high turnover, accountability gaps, and so on were identified through this scoping review and are opportunities for future policy reform across WIC offices. Through future digitalization efforts and reduction of learning costs, there is strong potential for change in the administration barriers WIC programs face [26].
In addition to administrative burdens, WIC also faces other policy challenges that can further exacerbate one’s access to services as a prospective or current participant. Before the COVID-19 pandemic, only about half of eligible participants were enrolled in WIC services. Many states use electronic benefit transfer (EBT) debit cards to redeem participants benefits, but there are several “offline” states which require participants to physically reload their EBT cards at an official WIC office every 3–4 months [27]. Due to government shutdowns, this made redeeming WIC benefits especially difficult and deterred many eligible families from participating in WIC services [27].
Online educational programs to promote nutritional practices have shown to be a useful tactic in behavior change, and increasing redemption rates in other federal programs, like SNAP. These programs have become more widespread and have a higher rate of participation than in-person educational sessions. These nutrition-focused sessions have shown to increase the amount of fruit and vegetable purchases redeemed [28]. Incorporating these programs could provide better approaches to educate WIC participants of the options they have for redemptions and decrease the frustration and stigma that may come with shopping for WIC qualified products.
Although the literature indicates that these enrollment interventions may increase participants in WIC programs, we have identified research gaps that should be addressed. First, several studies require further research to establish statistical significance and program effectiveness. Additionally, work is needed to gather information on participant characteristics (age, language, location, etc.) to identify possible differences in demographics that might engage well with various enrollment interventions. Lastly, many of the studies examined were not longitudinal, so the long-term effects of the enrollment interventions overtime, and their impact on retention, have yet to be studied. The authors recommend these as future areas of enrollment investigation.
Study Limitations
Our study had several strengths We conducted a comprehensive search of the literature with no limitations on publication type. We were therefore able to assess the full breadth of literature on this topic. We also followed established PRISMA and Arksey & O’Malley guidelines and had two reviewers for the title, abstract and full text reviews, encouraging thoroughness. Our study also had several limitations. While we attempted to include all WIC engagement programs that had reported outcomes, there may be more whose results are either not publicly available, not yet published, or which we did not identify in our search. In addition, many of the interventions analyzed took place during the COVID-19 pandemic, which may have influenced the findings. We did not formally assess the quality of the included studies, which may have led to risk of bias or low-quality data inclusions. Further work to measure results of other WIC participation intervention would continue to advance our understanding of which methods work best to increase WIC utilization.
Conclusion
This scoping review highlights the wide variety of enrollment interventions being practiced at WIC offices across the US. The literature indicates that there are a wide variety of ways to engage WIC participants to continue participation or access additional benefits with varying levels of success, many suggesting online/virtual engagement strategies may be most effective. Ensuring engagement is vital to providing WIC eligible families with nutritional support and with the pathways to access WIC programs.
References
US Department of Agriculture. (2021). WIC Special Project Grants. Food and Nutrition Service. Retrieved June 27, 2022, from https://www.fns.usda.gov/wic/wic-special-project-grants
Owen, A. L., & Owen, G. M. (1997). Twenty years of WIC: A review of some effects of the program. Journal of the American Dietetic Association, 97(7), 777–782. https://doi.org/10.1016/S0002-8223(97)00191-0
Currie, J., & Rajani, I. (2015). Within-mother estimates of the effects of WIC on birth outcomes in New York City. Economic Inquiry, 53(4), 1691–1701. https://doi.org/10.1111/ecin.12219
Weinfield, N. S., Borger, C., Au, L. E., Whaley, S. E., Berman, D., & Ritchie, L. D. (2020). Longer participation in WIC is associated with better diet quality in 24-month-old children. Journal of the Academy of Nutrition and Dietetics, 120(6), 963–971. https://doi.org/10.1016/j.jand.2019.12.012
Jackson, M. I. (2015). Early childhood WIC participation, cognitive development and academic achievement. Social Science and Medicine, 126, 145–153. https://doi.org/10.1016/j.socscimed.2014.12.018
Figlio, D., Hamersma, S., & Roth, J. (2009). Does prenatal WIC participation improve birth outcomes? New evidence from Florida. Journal of Public Economics, 93(1), 235–245. https://doi.org/10.1016/j.jpubeco.2008.08.003
Schramm, W. F. (1985). WIC prenatal participation and its relationship to newborn Medicaid costs in Missouri: A cost/benefit analysis. American Journal of Public Health, 75(8), 851–857. https://doi.org/10.2105/AJPH.75.8.851
Smith, K. (2016). Fewer than half of WIC-eligible families receive WIC benefits. Carsey School of Public Policy. https://doi.org/10.34051/p/2020.267
USDA ERS - WIC Participation Continues To Decline. Retrieved May 26, 2022, from https://www.ers.usda.gov/amber-waves/2017/june/wic-participation-continues-to-decline
Gago, C. M., Wynne, J. O., Moore, M. J., et al. (2022). Caregiver perspectives on underutilization of WIC: A qualitative study. Pediatrics, 149(2), e2021053889. https://doi.org/10.1542/peds.2021-053889
Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. https://doi.org/10.1080/1364557032000119616
Ouzzani, M., Hammady, H., Fedorowicz, Z., & Elmagarmid, A. (2016). Rayyan—a web and mobile app for systematic reviews. Systematic Reviews, 5(1), 210. https://doi.org/10.1186/s13643-016-0384-4
TIDieR | Author tool. Retrieved June 27, 2022, from http://www.tidierguide.org/#/author-tool
Vasan, A., Kenyon, C. C., Feudtner, C., Fiks, A. G., & Venkataramani, A. S. (2021). Association of WIC participation and electronic benefits transfer implementation. JAMA Pediatrics, 175(6), 609–616. https://doi.org/10.1001/jamapediatrics.2020.6973
Vasan, A., Kenyon, C. C., Roberto, C. A., Fiks, A. G., & Venkataramani, A. S. (2021). Association of remote vs in-person benefit delivery with WIC participation during the covid-19 pandemic. JAMA, 326(15), 1531–1533. https://doi.org/10.1001/jama.2021.14356
US Department of Agriculture. (2022, April 27). WIC Frequently Asked Questions (FAQs). Food and Nutrition Service. Retrieved July 21, 2022, from https://www.fns.usda.gov/wic/frequently-asked-questions
Seidel, M., Brink, L., Hamilton, M., & Gordon, L. (2018). Increasing WIC farmers’ market nutrition program redemption rates: Results and policy recommendations. Progress in Community Health Partnerships: Research, Education, and Action, 12(4), 431–439. https://doi.org/10.1353/cpr.2018.0068
Di Noia, J., Monica, D., Cullen, K. W., & Sikorskii, A. (2015). A randomized controlled trial of nutrition education to promote farmers’ market fruit and vegetable purchases and consumption among women enrolled in the Special Supplemental Nutrition Program for Women, Infants and Children (WIC): Rationale and design of the WIC Fresh Start program. BMC Nutrition, 1(1), 33. https://doi.org/10.1186/s40795-015-0032-8
Zhang, J., Zhang, Q., Tang, C., et al. (2022). The role of generic price look-up code in WIC benefit redemptions. Journal of Public Policy & Marketing. https://doi.org/10.1177/07439156221092418
Sekhobo, J. P., Peck, S. R., Byun, Y., et al. (2017). Use of a mixed-method approach to evaluate the implementation of retention promotion strategies in the New York State WIC program. Evaluation and Program Planning, 63, 7–17. https://doi.org/10.1016/j.evalprogplan.2017.03.002
USDA Food and Nutrition Service. (2016). WIC Farmers Market Nutrition Program for FY 2014. Retrieved July 13, 2022, from https://www.fns.usda.gov/fmnp/wic-farmers-market-nutrition-program
Herd, P., & Moynihan, D. (2022). How administrative burdens can harm health. Health Affairs. https://doi.org/10.1377/hpb20200904.405159
Maneely, J. (April 27, 2021). Matching data across benefit programs can increase WIC enrollment. Center on Budget and Policy Priorities. Retrieved June 27, 2022, from https://www.cbpp.org/research/food-assistance/matching-data-across-benefit-programs-can-increase-wic-enrollment
Reinvigorating and Reimaging The Pennsylvania WIC Program. WHAMglobal. Retrieved June 27, 2022, from https://www.whamglobal.org/blog/viewall/reinvigorating-and-reimaging-the-pennsylvania-wic-program
Summary of WIC State Agency Strategies for Increasing Child Retention. WIC Works Resource System. Retrieved June 27, 2022, from https://wicworks.fns.usda.gov/resources/summary-wic-state-agency-strategies-increasing-child-retention
Barnes, C., & Riel, V. (2022). “I don’t know nothing about that:” How “learning costs” undermine COVID-related efforts to make SNAP and WIC more accessible. Administration & Society. https://doi.org/10.1177/00953997211073948
Vasan, A. (September 8, 2021). The impact of in-person benefit reloading on WIC participation during the COVID-19 pandemic. Retrieved June 27, 2022, from https://policylab.chop.edu/blog/impact-person-benefit-reloading-wic-participation-during-covid-19-pandemic
Au, L. E., Whaley, S., Gurzo, K., Meza, M., & Ritchie, L. D. (2016). If you build it they will come: Satisfaction of WIC participants with online and traditional in-person nutrition education. Journal of Nutrition Education and Behavior, 48(5), 336-342.e1. https://doi.org/10.1016/j.jneb.2016.02.011
Acknowledgements
The authors would like to thank Paige Scudder for her assistance with the search strategy. They would also like to thank Alice Ely, Dr. Rudolph Fedrizzi, and the rest of the Vermont WIC staff that helped contribute to the idea generation and organization of this project.
Funding
No funding was received to assist with the preparation of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Davis, R.A., Leavitt, H.B. & Chau, M. A Review of Interventions to Increase WIC Enrollment and Participation. J Community Health 47, 990–1000 (2022). https://doi.org/10.1007/s10900-022-01131-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-022-01131-2