
Abstract
Unfortunately, only a small percent of pathological gamblers seek the professional help they need. In the current study, we test the idea that individual differences in reward sensitivity should predict whether a pathological gambler has sought treatment—the odds of treatment seeking should decrease as reward sensitivity increases. This hypothesis rests on the proposition that reward sensitive pathological gamblers should find treatment seeking aversive because doing so would remove a route to reward. We also tested those motivations to gamble that are positively reinforcing (social affliction and self-enhancement) as a possible mechanism by which reward sensitivity undermines treatment seeking—we did not anticipate negatively reinforcing motivations (e.g., coping) to be a mechanistic variable. Ninety-two pathological gamblers completed a large-scale survey that contained the variables of interest. As predicted, pathological gamblers were less likely to have sought treatment as reward sensitivity increased. Moreover, this relationship was mediated by social affiliation motivations to gamble, but not self-enhancement or coping motives. Reward sensitive gamblers did not wish to seek treatment to the extent that they were motivated to gamble for the social interactions it provides—seeking treatment would cut this avenue of affiliation with others. In light of these results, we suggest health care professionals take reward sensitivity into account when trying to promote treatment seeking, to say nothing of the social affiliation motives that underlie the reward sensitivity-treatment seeking link.
Similar content being viewed by others


To the gambler, the prospect of success looms large in any wager. Indeed, one of the allures of betting on games of chance is the possibility that the gambler will be rewarded (Neighbours et al. 2002). Some gamblers, however, are more sensitive to the potential of winning than are other gamblers. That is, whilst all gamblers place bets in the hope of financial gain, some gamblers are particularly attracted to the prospect of a rewarding outcome (i.e., a monetary wins). A propensity to be attracted to reward is often labeled reward sensitivity (Torrubia et al. 2001). Importantly, individual differences in reward sensitivity have been implicated in heightened risk for addiction, including alcoholism (see Loxton and Dawe 2006) and compulsive behaviors (see Davis and Woodside 2002). However, there is limited research on how reward sensitivity among those who are already addicted influences treatment seeking. In the current study, we test the idea that pathological gamblers who are reward sensitive may be especially reluctant to seek treatment. We base this on the contention that their attraction to reward might overpower the need for professional assistance.
Importantly, sensitivity to reward in-and-of-itself might not fully explain why pathological gamblers fail to seek treatment. According to Davis et al. (2007), motivational factors underlie the reward sensitivity-behavior link. In this light, gambling motivations might be at the heart of an association between reward sensitivity and the desire to continue gambling. In the current study, we test the idea that reward sensitivity undermines treatment seeking among pathological gamblers to the extent that they are motivated to gamble due to self-enhancement or social affiliation needs.
Sensitivity to Reward and Treatment Seeking Among Pathological Gamblers
Although a harmless form of entertainment for most, gambling can result in serious negative consequence for a small, but significant proportion of the population (Shaffer et al. 1999; Volberg 1994). Often referred to as problem or pathological gamblers, this segment of the gambling population is frequently persistent at gambling in the face of continued loss (Young and Wohl 2009), chase their loses (Lesieur 1984), and has difficulty quitting or cutting down their gambling (among other maladaptive behaviors). Of course, altering one’s problematic gambling behavior is very difficult. Doing so often involves numerous attempts to quit, followed by relapse and further attempts to quit (see the transtheoretical model of change; Prochaska and DiClemente 1986). To facilitate change, gamblers often need to seek professorial care (Nathan 2003).
Unfortunately, only a minority of pathological gamblers seek professional help to resolve their problem. Indeed, Hardoon et al. (2003) reported that only 18.8 % of people identified as problem gamblers contemplate seeking treatment. Empirically-based explanations for this failure to seek help from a professional (e.g., an addictions counselor) are limited (for an exception see Wohl et al. 2005). Yet, understanding the mechanisms that help or hinder treatment seeking may provide a base for public health initiatives aimed at secondary prevention of pathological gambling. Moreover, the empirical assessment of factors that undermine cutting back and quitting might also benefit mental health professionals involved in treating clients who are attempting to overcome their gambling disorder.
We offer reward sensitivity as a possible psychological impediment for treatment seeking behaviors. According to Gray (1981, 1982), individual differences exist in people’s response to incentives or rewards—otherwise known as reward sensitivity. Driven by differences in the behavioral activation system (BAS; Fowles 1987; Gray 1982; Torrubia et al. 2001), people who are reward sensitive demonstrate a lack of restraint over reward seeking and appetitive behaviors (Carver and White 1994; Cloninger 1988; Smillie and Jackson 2005). Indeed, reward sensitivity has been implicated in over-consumption behaviors such as alcohol abuse and binge eating (Davis et al. 2007; O’Connor and Colder 2005). This is because reward sensitive people seek out behaviors they find rewarding and have less restraint in delaying the satisfaction they gain from those behaviors. This situation may be particularly problematic in terms of treatment seeking among people who have already developed problematic behavioral patterns. Specifically, quitting or cutting back a rewarding, yet, problematic behavior, such as gambling, may be difficult for people who are sensitive to reward, particularly for those already struggling with problem gambling. In this regard, it is expected that reward sensitivity will be inversely related to treatment seeking. However, we argue that the reward sensitivity-treatment seeking link is likely indirect. Herein, we test the idea that variations in the gambler’s motivation to play might be a mechanism by which sensitivity to reward undermines willingness to seek treatment.
Sensitivity to Reward: From Motivation to Treatment Seeking
Reward sensitivity describes not only individual differences in response to the possibility of reward, but also the reason why some people seek reinforcing stimuli (Davis et al. 2007). Indeed, being sensitive to reward elevates incentive motivation (Robinson and Berridge 2001), especially when an activity results in positive reinforcement (Reuter et al. 2005). Gambling, by virtue of the possibility of winning at a game of chance, provides the opportunity for positive reinforcement (Stewart and Zack 2008). In this light, reward sensitive people are likely to be attracted to gambling for those aspects of the game that are positively reinforcing.
Although gamblers report a varied array of reasons for their gambling behavior (see Neighbours et al. 2002), Stewart and Zack (2008) provided evidence for two overarching motives that are associated with the positively reinforcing aspects of gambling. First, some gamblers are motivated to gamble for the purpose of self-enhancement. Specifically, these gamblers play to increase the quantity and quality of positive emotion (i.e., internal, positive reinforcement) through the thrill and excitement of gambling (Boyd 1976; Coventry and Brown 2006). Second, some gamblers are motivated to gamble for the social interaction or affiliations that play provides. The socially motivated gambler might be attracted by the prospect of talking to other gamblers around the betting table or by the prospect of going to the casino with friends. Because gambling can provide self-enhancement and social reinforcement, reward sensitive gamblers might be particularly reluctant to seek treatment to the extent that these motivations are important—by seeking treatment, an avenue to fulfill their positive reinforcing needs would be blocked. To the point, we hypothesized that enhancement and social motives are potential mediators of the hypothesized association between reward sensitivity and treatment seeking.
Note, however, gambling can also provide the opportunity for negative reinforcement. In this way, some gamblers are motivated to play as a means of coping with negative life events that yield negative emotions, i.e., to temporarily escape their life problems (Diskin and Hodgins 1999; Ledgerwood and Petry 2006; Wynne 1994). According to Stewart and Zack (2008), gamblers who engage in play for its negative reinforcing qualities are coping motivated. We contend that because reward sensitivity leads people to seek out positive reinforcing activities, reward sensitive gamblers are not likely to be motivated to play as a means to cope. As such, coping motivation is not a likely candidate mediating variable for the reward sensitivity-treatment seeking link.
Overview of Current Research
Although prior research (see Lloyd et al. 2010; Stewart and Zack 2008) has demonstrated that gambling-related motives predict problematic gambling behavior, to our knowledge, no research has focused on how the gambling motives among those who have already developed pathological gambling behavior influence treatment seeking. We argue that gambling motives that are positively reinforcing should mediate the relationship between reward sensitivity and treatment seeking. This is because reward sensitive pathological gamblers should be motivated to play as a way to attain positive reinforcement, i.e., for enhancement or social reasons. These motivations should, in turn, undermine treatment seeking because quitting or cutting back would remove these gamblers preferred vehicle for reward.
In summary, the purpose of the current study was to investigate the role that gambling motives play in the relationship between sensitivity to reward and treatment seeking among pathological gamblers. It was expected that gamblers with an elevated sensitivity to reward would report less treatment seeking behavior than gamblers with low sensitivity to reward. Moreover, we hypothesized that the reward sensitivity-treatment seeking link would be mediated by self-enhancement and social motives, but not coping motives.
Methods
Participants
Participants were 92 gamblers (61 male and 31 female) recruited via advertisements at a casino, a gambling addictions centre, online, and at a large Canadian university. Participants were selected based on gambling pathology according to the DSM-IV (American Psychiatric Association [APA] 1994). Specifically, the current sample was composed of pathological gamblers (5 or more endorsed criteria). The age of this sample ranged from 19 to 78 years (M = 38.15, SD = 15.20), and were from various ethnic backgrounds (Caucasian/European 72.8 %; East Asian 12 %; Native Canadian/American 7.6 %; African-Canadian 2.2 %, and other or multi-ethnic 5.4 %). Following study involvement all participants were provided $25 for their time.
Procedure
Upon arriving at the laboratory, an experimenter greeted participants and explained that the purpose of the current study was to investigate peoples’ gambling attitudes and beliefs. Participants were then asked to read and sign an informed consent. Following this consent, participants were given a study booklet containing a series of questionnaires including: the DSM-IV checklist for pathological gambling (APA 1994), the gambling motives questionnaire (Stewart and Zack 2008), and the sensitivity to punishment and sensitivity to reward questionnaire (Torrubia et al. 2001). Upon completion of the study booklet, participants were verbally debriefed.
Measures
Sensitivity to Reward
The Sensitivity to Reward (SR) scale of the Sensitivity to Punishment and Sensitivity to Reward Questionnaire is a one factor 24-item measure, used to detect individual differences in the functional capabilities of the Behavioural Activation System (BAS; Fowles 1987; Gray 1982). Specifically, it was designed to show differences in peoples impulsivity dimension, described by Gray (Torrubia et al. 2001). The SR scale differs from Carver and White’s (1994) three-factor BAS measure (i.e., drive, reward responsiveness, and fun seeking) in that it measures specific rewards (e.g., money, sex, social power, and praising; Torrubia et al. 2001) conglomerated into a single factor. Example items include: “Do you often do things to be praised?” or “Would you like to be a socially powerful person?” A “yes” “or “no” response was provided for each item. The SR scale showed good internal consistency (Cronbach’s α = .85).
Gambling Motives
The Gambling Motives Questionnaire (GMQ) is a three factor 15-item measure that assesses motivations to gamble. The GMQ measures three motives: enhancement motives (e.g., because it’s exciting), social motives (e.g., to be sociable), and coping motives (e.g., to forget your worries). Both enhancement and social motives are driven by positive reinforcement, such that gambling brings positive emotion; however, they differ in that enhancement motives are for internal reasons whereas social motives are for external reasons. Conversely, coping motives are driven by negative reinforcement, where gambling brings a relief of an internally aversive state (e.g., depressed mood or nervousness). Responses were anchored at 1 (almost never/never) and 4 (almost always). The GMQ demonstrated good internal consistency (Cronbach’s α = .83).
Treatment Seeking
Participants were asked to indicate if they had ever been to a professional counselor to help with their excessive gambling within their lifetime. A “yes” or “no” response was provided.
Results
Preliminary Analysis
We first examined whether sex differences were present among the measured variables. Analysis of Variance (ANOVA) revealed that males (M = .61, SD = .26) had significantly higher reward sensitivity than females (M = .45, SD = .21), F(1, 91) = 9.42, p = .003—a result that is replicated in the literature (see Li et al. 2007). ANOVA also showed that, akin to prior research (Stewart and Zack 2008) females (M = 2.72, SD = .59) gamble significantly more for coping motives than males (M = 2.28, SD = .68), F(1, 92) = 9.85, p = .002. No sex differences were found with respect to enhancement motives, F(1, 92) = .40, p = .53, or social motives, F(1, 92) = .13, p = .72. Finally, logistic regression analysis revealed that treatment seeking did not differ by sex, Wald’s χ 2 (1) = .61, p = .44. Since sex did significantly predict differences in reward sensitivity and gambling motives, we controlled for sex in all subsequent analysis.
Treatment Seeking
To test the effect of sensitivity to reward on treatment seeking, we conducted a binary logistic regression. This analysis revealed that sensitivity to reward was a significant predictor of lifetime treatment seeking, Wald’s χ 2 (1) = 6.20, p = .01. Specifically, the likelihood that a problem gambler had ever been to a professional counselor to help with their excessive gambling within their lifetime decreased as their sensitivity to reward increased, OR = .09. Importantly, the Hosmer–Lemeshow goodness-of-fit test was insignificant, χ 2 (8) = 4.63, p = .80, and thus the model fit the data well.
In order to determine if gambling motives predicted treatment seeking and efforts to change, we conducted three separate binary logistic regressions. Specifically, each GMQ subscale was entered into a logistic equation separately and used to predict treatment seeking. Results revealed that coping motives predicted lifetime treatment seeking, Wald’s χ 2 (1) = 3.48, p = .06. The likelihood that a problem gambler had ever been to a professional counselor to help with their excessive gambling within their lifetime increased as coping motives increased, OR = 1.92. This model was a good fit to the data according to the Hosmer–Lemeshow goodness-of-fit test, χ 2 (8) = 3.82, p = .87.
Similarly, social motives significantly predicted lifetime treatment seeking, Wald’s χ 2 (1) = 11.77, p = .001. The likelihood that a problem gambler had ever been to a professional counselor to help with their excessive gambling within their lifetime decreased as social motives increased, OR = .26. Again, this model was a good fit to the data according to the Hosmer–Lemeshow goodness-of-fit test, χ 2 (8) = 6.80, p = .56. Finally, enhancement motives were not a significant predictor of lifetime treatment seeking, Wald’s χ 2 (1) = 1.23, p = .27.
Reward Sensitivity
To test the effect of sensitivity to reward on gambling motives, three separate regression analyses were conducted on each subscale of the GMQ. Results revealed that increased sensitivity to reward significantly predicted increased gambling for enhancement motives, B = .06, t(90) = 3.92, p < .001, and social motives, B = .06, t(90) = 3.64, p < .001. However, gambling for coping motives was not significantly predicted by sensitivity to reward, B = .02, t(90) = .96, p = .34.
Mediation Analysis
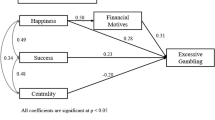
To determine whether gambling motives mediated the relationship between sensitivity to reward and problem gambling, Barron and Kenny’s (1986) regression procedure for testing mediation was used. As demonstrated by the previously reported regression analyses, reward sensitivity is a predictor of gambling for both enhancement and social motives, but only social motives was a significant predictor of treatment seeking. As such, social motivation to gamble (but not enhancement) was a viable potential mediator according to Barron and Kenny’s procedure. Thus, we proceeded to test the full mediation model with only social motives as a possible mediator. Importantly, when social motives was added into a mediating model, the direct effect between sensitivity to reward and treatment seeking became non-significant, B = −1.46, Wald’s χ 2 (1) = 1.90, p = .17. See Fig. 1.

Mediation model with reward sensitivity as the independent variable, social motives to gamble as the mediator, and treatment seeking as the dependent variable. The unstandardized coefficients and standard error shown in parentheses reflect the inclusion of the mediator into the equation. Unstandardized coefficients and standard error with a single asterisk indicate a significant path at p < .05; double asterisk indicate a significant path at p < .01
We then used the bootstrapping technique (with 5,000 iterations) recommended by Preacher and Hayes (2004) to determine whether the indirect effect of social motives was significant. This analysis revealed that the indirect effect of sensitivity to reward on treatment seeking through social motives was significantly different from zero at p < .05, as zero is not within the 95 % confidence intervals, CI 95 = −3.39, −.35. Thus, we conclude that social motives do indeed mediate the effects of reward sensitivity on treatment seeking.
Importantly, an alternative model was also examined with social motivation to gamble as a predictor and reward sensitivity as a mediator. Again, we then used the bootstrapping technique (with 5,000 iterations) recommended by Preacher and Hayes (2004) to determine the indirect effect of reward sensitivity in this alternative model was significant. However, the indirect effect was not statistically significant, CI 95 = −.56, .03, suggesting that our proposed original mediation model is a better explanation for the relationship between reward sensitivity, social motivations and treatment seeking.
Discussion
Reward sensitive people find it difficult to refrain from engaging in appetitive behaviors (Cloninger 1988; Smillie and Jackson 2005; Torrubia et al. 2001). In the current study, we examined reward sensitivity within the context of gambling. Specifically, we tested the idea that reward sensitivity among pathological gamblers would predict treatment seeking behavior. In line with our general hypothesis, reward sensitivity was negatively associated with seeking treatment among pathological gamblers. Gamblers high in reward sensitivity simply felt that the cost of quitting—abandoning their route to reward—outweighed the cost of continued play—financial loss.
We also showed that reward sensitivity increased pathological gamblers’ motivation to gamble for its positive reinforcing qualities. Specifically, we showed that participants who were sensitive to reward were more likely to report being motivated to gamble for self-enhancement and social affiliation reasons. Put another way, pathological gamblers who are sensitive to reward engage in play because doing so makes them feel good about themselves and provides them with social connections. These results are in line with the extant literature on reward sensitivity that suggests reward sensitive people are attracted to positive reinforcing, appetitive behaviors (e.g., Corr 2004; Davis et al. 2007; Kambouropoulos and Staiger 2002). Gambling provides such an opportunity because wins allow for self-enhancement and the nature of some gambling games (e.g., poker and craps) creates a social environment for players. Reward sensitivity, however, did not predict coping-related motives for play. This is consistent with previous research suggesting that negative reinforcement (coping-related motives) is linked to behavioral inhibition, as opposed to reward sensitivity (or behavioral activation) (see O’Connor and Colder 2005; Wardell et al. 2011).
Importantly, we also hypothesized that the relationship between reward sensitivity and treatment seeking is indirect. That is, we predicted gambling-related motives that are focused on the positive reinforcing nature of gambling would mediate the reward sensitivity-treatment seeking link. However, only the need for the social aspects of gambling predicted treatment seeking such that the more gamblers engaged in play to fulfill the social needs, the less likely it was that they sought treatment for their gambling. Unlike social motives, whether or not a person feels enhanced via gambling depends on the outcome of play. It is possible that the null effect between enhancement motives and treatment seeking is the result of two opposing situations—those who don’t self-enhance via play seek treatment whereas those who do enhance via play continue wagering. Unfortunately, we did not include variables to assess this possibility. Social motives, however, did predict treatment seeking. That is, the more pathological gamblers gambled for the social connections it provided, the less likely they were to have sought treatment. Intuitively, this association makes some sense. By seeking treatment, the reward sensitive pathological gambler is forfeiting a consistent route to positive reinforcement.
Because reward sensitivity predicted social motives to gamble, and because social motives to gamble predicted treatment seeking, we were able to test a mediation model in which reward sensitivity predicts treatment seeking to the extent that the gamblers played to fulfill social needs. As predicted, social motives fully mediated the relationship between reward sensitivity and seeking professional treatment. This result is particularly informative in light of the fact that the extant gambling literature has largely ignored social motives because it fails to predict the development of pathological gambling (see Stewart and Zack 2008). The current research suggests that although social motives are not predictive of symptomatology they hold particular significance once a person has developed pathological patterns of gambling behavior. Specifically, pathological gamblers who are sensitive to reward are less likely to seek treatment if they gamble for social motives.
We suggest that one possible reason for the significant role played by social motives in the reward sensitivity-treatment seeking link is that social affiliation provides reliable and consistent positive reinforcement regardless of gambling-related outcomes. That is, reward sensitive pathological gamblers develop positively reinforcing social affiliations in a gambling environment—fulfilling a need—that is not contingent on whether they win or lose. By seeking treatment, the gambler not only brings an end to their gambling behavior, but likely their social network. The result would be a great deal of social pain—a type of pain that has been shown to be equal to, if not greater than, physical pain (see MacDonald and Leary 2005; Papini et al. 2006).
Caveats and Future Directions
Some limitations of the current study should be noted. First, the pathological gamblers that participated in the current study were recruited using convenience sampling. That is to say, participants were largely comprised of gamblers who chose to answer advertisements about a study on gambling attitudes and behavior. In this way, the current sample of pathological gamblers may not be representative of all pathological gamblers. Indeed, research suggests that those who volunteer to participate in gambling research may be more likely to be thinking about changing or cutting back their gambling behavior (Wohl and Sztainert 2011). Therefore, this study may over represent pathological gamblers who might seek treatment or change their gambling behavior. However, this should not affect the relationships between reward sensitivity and gambling motivations found in the current study. Further research should examine gamblers’ likelihood to seek treatment in the future and willingness to seek treatment among gamblers who have not yet done so.
Secondly, the current study did not examine those without pathology. Thus, the current research is more relevant to treatment than prevention. It is possible that reward sensitivity develops in recreational gamblers, and then leads to enhancement motivations as the gambler progresses into pathology. However, due to the cross-sectional nature of this study, questions about the progression of reward sensitivity and gambling motivations could not be directly assessed. To determine whether reward sensitivity is a predictor of gambling pathology or whether reward sensitivity develops alongside gambling pathology is best determined via longitudinal studies.
Lastly, there is no single factor that determines why some individuals seek treatment and others do not. In this paper we put forward that reward sensitivity affects treatment seeking via gambling motivations. One of the gambling motivations which predicted treatment seeking was coping motives. Although this motivation was not related to reward sensitivity, is possible that other factors may explain its relationship to treatment seeking. Insofar as individuals use gambling as a form of stress reduction and escape from daily and long-term problems, coping motivations may be related to existing/historical stress and mood disorders. Therefore, future research should aim at explaining the coping motives to treatment seeking link among pathological gamblers.
Conclusion
The current study examined whether reward sensitivity undermines treatment seeking among pathological gamblers. Support was found for this contention. Importantly, we also showed that this association was indirect—reward sensitivity decreases treatment seeking to the extent that gambling fulfills pathological gamblers’ social needs. Therefore, the maintenance of social affiliations is an important consideration for efforts to get pathological gamblers to seek treatment. Thus, any stakeholder in motivating a pathological gambler to seek treatment (family, friends, clinicians, the industry to name a few) should take social needs into account, especially for gamblers who are sensitive to reward. Without finding avenues to build social networks outside of gambling, the reward sensitive gambler is unlikely to seek the professional support they need.
References
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51, 1173–1182.
Boyd, W. H. (1976). Excitement: The gambler’s drug. In W. R. Eadington (Ed.), Gambling and society (pp. 371–375). Springfield, IL: Thomas.
Carver, C. S., & White, T. L. (1994). Behavioral inhibition, behavioral activation, and affective responses to impending reward and punishments: The BIS/BAS scales. Journal of Personality and Social Psychology, 67, 319–333.
Cloninger, C. R. (1988). A unified biosocial theory of personality and its role in the development of anxiety states: A reply to commentaries. Psychiatric Developments, 5, 83–120.
Corr, P. J. (2004). Reinforcement sensitivity theory and personality. Neuroscience and Biobehavioral Reviews, 28, 317–332.
Coventry, K. R., & Brown, R. L. (2006). Sensation seeking, gambling and gambling addictions. Addiction, 88, 541–554.
Davis, C., Patte, K., Levitan, R., Reid, C., Tweed, S., & Curtis, C. (2007). From motivation to behaviour: A model of reward sensitivity, overeating, and food preferences in the risk profile for obesity. Appetite, 48, 12–19.
Davis, C., & Woodside, D. B. (2002). Sensitivity to the rewarding effects of food and exercise in the eating disorders. Comprehensive Psychiatry, 43, 189–194.
Diskin, K. M., & Hodgins, D. C. (1999). Narrowing of attention and dissociation in pathological video lottery gamblers. Journal of Gambling Studies, 15, 17–28.
Fowles, D. C. (1987). Application of a behavioral theory of motivation to the concepts of anxiety and impulsivity. Journal of Research in Personality, 21, 417–435.
Gray, J. A. (1981). A critique of Eysenck’s theory of personality. In H. J. Eysenck (Ed.), A model for personality (pp. 246–276). New York: Springer.
Gray, J. A. (1982). The neuropsychology of anxiety: An enquiry into the functions of the septo-hippocampal system. Oxford: Oxford University Press.
Hardoon, K., Derevensky, J. L., & Gupta, R. (2003). Empirical measures vs. perceived gambling severity among youth: Why adolescent problem gamblers fail to seek treatment. Addictive Behaviors, 28, 933–946.
Kambouropoulos, N., & Staiger, P. K. (2002). The influence of sensitivity to reward on reactivity to alcohol-related cues. Addiction, 96, 1175–1185.
Ledgerwood, D. M., & Petry, N. M. (2006). Psychological experience of gambling and subtypes of pathological gamblers. Psychiatry Research, 144, 17–27.
Lesieur, H. R. (1984). The chase: Career of the compulsive gambler. Cambridge, MA: Schenkman Books.
Li, C. S. R., Huang, C. Y., Lin, W. Y., & Sun, C. W. V. (2007). Gender differences in punishment and reward sensitivity in a sample of Taiwanese college students. Personality and Individual Differences, 43, 475–483.
Lloyd, J., Doll, H., Hawton, K., Dutton, W. H., Geddes, J. R., Goodwin, G. M., et al. (2010). How psychological symptoms relate to different motivations for gambling: An online study of internet gamblers. Biological Psychiatry, 68, 733–740.
Loxton, N. J., & Dawe, S. (2006). Reward and punishment sensitivity in dysfunctional eating and hazardous drinking women: Associations with family risk. Appetite, 47, 361–371.
MacDonald, G., & Leary, M. R. (2005). Why does social exclusion hurt? The relationship between social and physical pain. Psychological Bulletin, 131, 202–223.
Nathan, P. E. (2003). The role of natural recovery in alcoholism and pathological gambling. Journal of Gambling Studies, 19, 279–286.
Neighbours, C., Lostutter, T. W., Cronce, J. M., & Larimer, M. E. (2002). Exploring college student gambling motivation. Journal of Gambling Studies, 18, 361–370.
O’Connor, R. M., & Colder, C. R. (2005). Predicting alcohol patterns in first-year college students through motivational systems and reasons for drinking. Psychology of Addictive Behaviors, 19, 10–20.
Papini, M. R., Wood, M., Daniel, A. M., & Norris, J. N. (2006). Reward loss as psychological pain. International Journal of Psychology and Psychological Therapy, 6, 182–213.
Preacher, K. J., & Hayes, A. F. (2004). SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behavior Research Methods, Instruments, and Computers, 36, 717–731.
Prochaska, J. Q., & DiClemente, C. C. (1986). Toward a comprehensive model of change. In W. R. Miller & N. Heather (Eds.), Treating addictive behaviors: Processes of change (pp. 3–27). New York: Plenum Press.
Reuter, M., Schmitz, A., Conrr, P., & Hennig, J. (2005). Molecular genetics support Gray’s personality theory: The interaction of COMT and DRD2 polymorphisms predicts the behavioural approach system. The International Journal of Neuropsychopharmacology, 1, 1–12.
Robinson, T. E., & Berridge, K. C. (2001). Incentive-sensitization and addiction. Addiction, 96, 103–114.
Shaffer, H. J., Hall, M. N., & Vander Bilt, J. (1999). Estimating the prevalence of disordered gambling behavior in the United States and Canada: A research synthesis. American Journal of Public Health, 89, 1369–1376.
Smillie, L. D., & Jackson, C. J. (2005). The appetitive motivation scale and other BAS measures in the prediction of approach and active avoidance. Personality and Individual Differences, 38, 981–994.
Stewart, S. H., & Zack, M. (2008). Development and psychometric evaluation of a three-dimensional Gambling Motives Questionnaire. Addiction, 103, 1110–1117.
Torrubia, R., Avila, C., Molto, J., & Caseras, X. (2001). The sensitivity to punishment and sensitivity to reward questionnaire (SPSRQ) as a measure of Gray’s anxiety and impulsivity dimensions. Personality and Individual Differences, 31, 837–862.
Volberg, R. A. (1994). The prevalence and demographics of pathological gamblers: Implications for public health. American Journal of Public Health, 84, 237–241.
Wardell, J. D., O’Connor, R. M., Read, J. P., & Colder, C. R. (2011). Behavioral approach system moderates the prospective association between the behavioral inhibition system and alcohol outcomes in college students. Journal of Studies on Alcohol and Drugs, 72, 1028–1036.
Wohl, M. J. A., & Sztainert, T. (2011). Where did all the pathological gamblers go? Gambling symptomatology and stage of change predict attrition in longitudinal research. Journal of Gambling Studies, 27, 155–169.
Wohl, M. J. A., Young, M. M., & Hart, K. E. (2005). Untreated young gamblers with game-specific problems: Self concept involving luck, gambling ecology and delay in seeking professional treatment. Addiction Research and Theory, 13, 445–459.
Wynne, H. (1994). A description of problem gamblers in Alberta: A secondary analysis of the gambling and problem gambling in Alberta study. Edmonton: Alberta Alcohol and Drug Abuse Commission.
Young, M. M., & Wohl, M. J. A. (2009). The gambling craving scale: Psychometric validation and behavioral outcomes. Psychology of Addictive Behaviors, 23, 512–522.
Acknowledgments
This research was supported in part by an Ontario Problem Gambling Research Centre (OPGRC) research Grant (#2639).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Sztainert, T., Wohl, M.J.A., McManus, J.F. et al. On Being Attracted to the Possibility of a Win: Reward Sensitivity (via Gambling Motives) Undermines Treatment Seeking Among Pathological Gamblers. J Gambl Stud 30, 901–911 (2014). https://doi.org/10.1007/s10899-013-9394-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-013-9394-5