
Abstract
Intimate partner and family violence (IPFV) is highly prevalent among tertiary students in Australia and internationally. Yet, relatively little is known about the help-seeking patterns of student victim-survivors and how these patterns vary cross-culturally. This study examined formal help-seeking needs, behaviors, and barriers among women tertiary students in Australia who had experienced IPFV and cross-cultural differences therein. Cross-sectional survey data were collected from adult women studying at tertiary education institutions across Australia. Those who reported IPFV (physical, sexual, psychological, and/or financial) victimization during their adult lives were included in this study (N = 1,606). Descriptive statistics were calculated for the full sample and by cultural identity. A series of logistic regression analyses was conducted to assess associations between culture and help-seeking, unadjusted and adjusted for sociodemographic factors (gender identity, age, area, employment, and institution type). Less than half (48.7%) of participants had sought formal help, despite a larger proportion (66.2%) perceiving a need for such help. Two thirds (65.5%) of participants reported barriers to help-seeking, which were predominantly attitudinal or normative in nature. Cultural identity was significantly associated with help-seeking in the unadjusted and adjusted analyses. Cultural minority students were generally less likely to perceive a need for help and to seek help than the majority. Continued efforts are needed to promote and facilitate formal help-seeking for IPFV among tertiary students, and particularly among cultural minority students. Further work is needed to understand the factors that contribute to cultural inequalities in help-seeking and to inform culturally responsive support services for student victim-survivors.
Similar content being viewed by others


Violence against women is one of the most pervasive human rights violations in Australia and around the world (Australian Human Rights Commission, 2014; World Health Organization [WHO], 2021). This violence most often occurs in the context of intimate and familial relationships, referred to by various terms including ‘intimate partner violence’ (IPV), ‘family violence’, ‘domestic violence’, and ‘domestic abuse’. For clarity, the term ‘intimate partner and family violence’ (IPFV) is used throughout this paper to refer to any violence perpetrated by a current or former intimate partner or family member, including physical, sexual, psychological, financial, and other forms of abuse. This broader conceptualization captures the wide-ranging relationships in which violence can occur, including extended family and kinship networks, which are particularly relevant to Indigenous and cultural minority communities (Australian Institute of Health and Welfare [AIHW], 2019; Vaughan et al., 2015). It also reflects the frequent co-occurrence and common risk factors across different types of IPFV (Smith Slep & Heyman, 2001; Tolan et al., 2006). Still, most prior studies in this area focus exclusively on IPV, and this more specific term will be used when referring to their findings.
Intimate Partner and Family Violence Among Tertiary Students
Violence against women in the tertiary education sector has garnered increased research and public attention over recent decades (Rennison & Addington, 2014). This subpopulation may face increased vulnerabilities related to young age, financial insecurity, academic demands and stress, alcohol and drug use, mental health difficulties, campus and peer cultures, and violence-supportive attitudes (Duval et al., 2020; Kaukinen, 2014; Moylan & Javorka, 2020). Further, in addition to the physical and mental health impacts of violence that all victim-survivors face, including increased risk of chronic physical health conditions, chronic pain, depressive disorders, anxiety disorders, post-traumatic stress disorder, and suicide and self-inflicted injury (AIHW, 2019; Dillon et al., 2013), student victim-survivors may experience negative academic impacts including increased academic difficulties, lower academic achievement, and academic disengagement (Banyard et al., 2020; Brewer et al., 2018).
While research on violence among tertiary students has primarily focused on sexual assault, a growing body of evidence suggests that this subpopulation also experiences exceptionally high rates of IPFV (Rennison & Addington, 2014). Data from the International Dating Violence Study indicate that, across nearly 16,000 university students in 21 countries, a median of 26% had experienced physical assault, and 24% had experienced sexual coercion, by a dating partner in the previous 12 months (Chan et al., 2008). Among college students in the United States (US), studies have reported 12-month prevalence rates between 16% and 34% for physical IPV, 10% and 36% for sexual IPV, and 17% and 76% for psychological IPV (see literature review in Scherer et al., 2016). Among women tertiary students in Australia, a recent study reported prevalence estimates of 56% for physical violence, 53% for sexual violence, 81% for psychological violence, and 48% for financial violence, by an intimate partner or family member since the age of 18 years (Zark et al., in press).
Help-Seeking for Intimate Partner and Family Violence
Given the high prevalence and adverse effects of IPFV, it is important to understand victim-survivors’ help-seeking behaviors. Help-seeking refers to the process of actively pursuing external assistance, which may be in the form of understanding, advice, information, treatment, or general support (Rickwood et al., 2014). Disclosure refers more broadly to discussing one’s experience of victimization with another person (Mennicke et al., 2021). While help-seeking typically involves disclosure, not all disclosures are intended to gain help; nevertheless, the terms are often used interchangeably in the literature (see Sabina & Ho, 2014). Research distinguishes between two sources of help-seeking: formal (e.g., law enforcement, health care, and social services) and informal (e.g., family and friends; McCart et al., 2010). Extensive evidence indicates that engagement with services can reduce the impacts of victimization and the risk of revictimization (see literature reviews in Ravi et al., 2021, and Robinson et al., 2020). While informal social support also plays a critical role in protecting against negative health outcomes (Coker et al., 2003; Sylaska & Edwards, 2014), formal support systems may confer the additional benefits of connecting victim-survivors with evidence-based information, resources, and care (Mennicke et al., 2021). For the purpose of this paper, we focus on formal help-seeking for IPFV.
Two other concepts that are important for understanding help-seeking behaviors are perceived need and barriers. Perceived need refers to an individual’s subjective perception of the need for assistance or a particular type of assistance (McCart et al., 2010). Many victim-survivors may not seek services because they do not perceive a need for them, and conversely, many victim-survivors may perceive a need for services but not take action to procure them (Lövestad et al., 2021). Barriers refer to any factor that serves as an impediment to seeking or obtaining assistance. This could be by inhibiting disclosure, reporting, service access, service utilization, or any other aspect or stage of help-seeking (Walsh et al., 2010). While barriers are typically operationalized as reasons for not seeking services, victim-survivors may also face barriers related to initial engagement, extent of engagement, and re-engagement with services (Robinson et al., 2020). This study therefore considers help-seeking needs, behaviors, and barriers as three distinct yet interrelated constructs.
Prevalence of Help-Seeking
Research consistently demonstrates that the prevalence of formal help-seeking for IPFV is much lower than that of informal help-seeking (e.g., Ansara & Hindin, 2010; Goodson & Hayes, 2021; Ingram, 2007). Population-based surveys indicate that, in the US, only 30% of IPV victim-survivors have sought help from police and 20% from a doctor or psychiatrist (Kaukinen, 2004), and in Canada, 39% have sought help from a counsellor, 32% from a doctor or nurse, 30% from police, and 24% from a lawyer (Barrett & St Pierre, 2011). Data from the Australian Bureau of Statistics (ABS) 2016 Personal Safety Survey indicate that, among women who have experienced violence from a previous partner, only 21% have sought help from police, 16% from a general practitioner, 16% from a counsellor or support worker, 9% from a legal service, and 4% from a financial service (percentages calculated using data in ABS, 2018b). While few studies have examined IPFV victim-survivors’ perceived need for services, those that have indicate substantial discrepancies between perceived need and help-seeking behavior (Dichter & Rhodes, 2011; Lövestad et al., 2021; Satyen et al., 2018, 2021b). For example, in a recent Australian study of trends in IPV and help-seeking over a four-year period, between 53% and 71% (median = 64%) of women reported needing help from services, yet only 38–59% (median = 47%) reported seeking help from these services (Satyen et al., 2021b).
As per the broader literature on violence among tertiary students, the literature on help-seeking for violence in this subpopulation is largely focused on sexual assault (for a review, see Sabina & Ho, 2014). Yet, emerging evidence suggests that students’ rates of formal disclosure and help-seeking for IPV are even lower than for sexual and other forms of violence (Ameral et al., 2020; Demers et al., 2018; Mennicke et al., 2021). For example, in a recent analysis of data from over 8,000 US undergraduate students, Mennicke et al. (2021) found that 14% of those who experienced dating violence in the past year had disclosed this to a formal source, compared to 17% who experienced sexual harassment, 25% who experienced sexual violence, and 25% who experienced stalking. Although these different forms of victimization overlap, such findings highlight the need for greater attention to students’ help-seeking for violence within their relationships. Recent studies of US college student victim-survivors of IPV have reported overall rates of formal disclosure between 2% and 14% (Demers et al., 2018; Edwards et al., 2012; Mennicke et al., 2021) and overall rates of formal help-seeking between 9% and 23% (Addington, 2021; Ameral et al., 2020; Cho & Huang, 2017), depending on the types of violence and services included. These students appear to most frequently seek help from medical and mental health professionals (6–29%) and social workers (4–24%), and less frequently from police and lawyers (4–13%; Addington, 2021; Cho & Huang, 2017; Choi et al., 2021). However, estimates of student victim-survivors’ perceived need for assistance are lacking, rendering the extent of unmet need in this group unclear.
Barriers to Help-Seeking
A variety of barriers may underpin the low rates of help-seeking among IPFV victim-survivors. A systematic review of barriers to formal help-seeking for IPV in the US identified six key themes: lack of awareness (e.g., of IPV, of services), access challenges (e.g., location, time), fear of consequences (e.g., increased violence, consequences for partner or family), lack of material resources (e.g., housing, finances, transportation), personal barriers (e.g., self-blame, mental health concerns), and systemic failures (e.g., not feeling believed, lack of concern from services; Robinson et al., 2020). An earlier global review of factors facilitating and inhibiting help-seeking for IPV also identified barriers related to perceptions of violence, patriarchal norms and values, and social stigma (Lelaurain et al., 2017). The former included perceiving the violence as normal, not serious, or not severe enough; the latter included rigid gender roles, idealization of the family, and normalization of violence in relationships, which in turn contribute to feelings of shame, fear of blame and stigmatization, and taboo and silence around IPV. In Australia, the 2016 Personal Safety Survey found that women’s most common reasons for not seeking advice or support about IPV were feeling that they could deal with it themselves, not perceiving the problem as serious enough to seek help, shame or embarrassment, and not wanting or needing help (ABS, 2018a, 2018c).
Research on barriers to help-seeking for IPFV among tertiary students is scarce. The limited existing data from US college student victim-survivors of IPV indicate that the most common reasons for not seeking help are perceiving the matter as private or personal (45–56%) and perceiving the violence as not serious or important enough (17–56%; Ameral et al., 2020; Cho et al., 2020a; Choi et al., 2021). Other barriers reported by substantial minorities (5–15%) include concerns about consequences for the perpetrator, fear of retaliation, inconvenience, expectations that services would be ineffective or biased, and shame or embarrassment (Ameral et al., 2020; Cho et al., 2020a; Choi et al., 2021). Thus, as per the general population (e.g., ABS, 2018a, 2018c), the most pervasive barriers to help-seeking among students appear to be attitudinal or normative in nature (e.g., perceptions of violence, social stigma), though structural and environmental barriers (e.g., resources, accessibility) are also common. Of course, not all victim-survivors face the same obstacles to seeking support, and their experiences and challenges are shaped by sociocultural contexts and processes (Liang et al., 2005).
Theoretical Frameworks and the Role of Culture
Two theoretical frameworks that are key to understanding women’s experiences of and responses to IPFV are intersectionality and social-ecological models (Our Watch, 2021; Satyen et al., 2021a; Vaughan et al., 2015). Intersectionality, first coined by Crenshaw (1991), suggests that an individual’s or group’s identity is shaped by multiple intersecting factors including gender, sexuality, age, race, ethnicity, and class, and these intersections are associated with different forms of oppression and discrimination or power and privilege. An intersectional analysis of IPFV considers how these overlapping identities and oppressions produce different experiences of violence (The Equality Institute, 2017; Our Watch, 2021). Social-ecological models suggest that an individual’s experience is shaped by an interplay of factors operating at multiple levels, including the individual and relationship, community and organizational, system and institutional, and societal levels (Our Watch, 2021). A social-ecological analysis of IPFV considers how the norms, practices, and structures at each of these levels shape the context of violence (UN Women, 2015). Combining an intersectional and social-ecological approach allows us to conceptualize how factors operating at multiple levels can give rise to differences in IPFV and help-seeking across diverse individuals and communities.
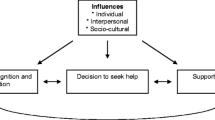
Help-seeking itself is complex and multidimensional, and several conceptual models have been proposed to explain the stages and processes involved (for a review, see Day et al., 2018). One of the most widely recognized is Liang et al.’s (2005) model of help-seeking for IPV, which delineates three stages: problem definition and appraisal, the decision to seek help, and the selection of a help provider. The first stage refers to the process of interpreting one’s experience of violence, including defining the problem and evaluating its severity. The second stage refers to the process of deciding to disclose the violence and seek help, which stems from problem recognition and continually shifts in line with one’s appraisal of their situation and external circumstances. The third stage refers to the process of identifying a source of support, which involves weighing the potential costs and benefits of formal and informal options. Each of these processes is shaped by individual, interpersonal, and sociocultural factors (Liang et al., 2005).
With advances in understandings of IPFV and help-seeking, there has been increased consideration of the role of culture. Culture can be broadly defined as the shared beliefs, values, norms, and practices of a group (Ung, 2015; Webster et al., 2019). While culture can apply to any group based on any common characteristic, it is most often associated with country, race, and ethnicity (Webster et al., 2019). In the US, the term ‘racial/ethnic minority’ is commonly used to refer to all racial/ethnic groups other than the White/European American majority (Kasturirangan et al., 2004). In Australia, the term ‘culturally and linguistically diverse’ (CALD) is used to refer to all non-Indigenous ethnic groups other than the Anglo-Saxon English-speaking majority (Sawrikar & Katz, 2009). In practice, CALD is usually defined as people born overseas, particularly in non-main English-speaking countries (Pham et al., 2021). Regardless of the terminology and definitions used, it is critical to acknowledge that cultural minorities are not homogeneous; on the contrary, they comprise diverse individuals and groups with varied identities and experiences (Kasturirangan et al., 2004). At the same time, cultural minority women may share common influences in relation to IPFV and help-seeking, including experiences of disadvantage and discrimination from both within their communities and the dominant society (Kasturirangan et al., 2004; Sokoloff & Dupont, 2005).
Indeed, the intersection of gender and cultural identity can present compounded and unique challenges to seeking help for IPFV (for reviews, see Femi-Ajao et al., 2020; Hulley et al., 2022; Vaughan et al., 2015). At the systemic and societal levels, cultural prejudice and discrimination contributes to a climate in which violence against cultural minority women is condoned (The Equality Institute, 2017; Our Watch, 2021). Stereotypes of some cultures as being inherently more oppressive or violent can serve to decrease the accountability of perpetrators and disempower victim-survivors, and women may refrain from seeking help for fear of misrepresenting and reinforcing negative stereotypes about their communities (Kasturirangan et al., 2004; Multicultural Centre for Women’s Health, 2020; Sokoloff & Dupont, 2005). Structural inequalities can give rise to additional barriers to accessing and utilizing services, including financial insecurity and dependence, fear and distrust of government agencies and authorities, immigration status and fear of deportation, language difficulties, lack of information about legal rights and service systems, and lack of culturally appropriate or culturally specific services (Femi-Ajao et al., 2020; Hulley et al., 2022; Kasturirangan et al., 2004; Lu et al., 2020; Mitra-Kahn et al., 2016; State of Victoria, 2016; Vaughan et al., 2015). At the community level, sociocultural norms regarding gender, sexuality, marriage, and family may also impede help-seeking (Department of Social Services, 2015). These include beliefs about gender roles and responsibilities, the permanence of marriage and shame of divorce, the importance of family privacy and honor, and the prioritization of family and community over personal safety, health, and wellbeing (Department of Social Services, 2015; Mitra-Kahn et al., 2016; Satyen, 2021; Satyen et al., 2020; Vaughan et al., 2015). While many of these barriers also apply to women in the dominant society, the experiences of cultural minority women are uniquely shaped by their membership of a marginalized cultural group (Lu et al., 2020).
Cross-Cultural Differences in Help-Seeking
Research indeed suggests that the nature and extent of help-seeking for IPFV varies across cultures. A systematic review of cross-cultural differences in women’s help-seeking behavior for IPV found that White women are more likely to utilize mental health and social services, while Black/African American and Latinx/Hispanic women are more likely to utilize emergency departments and law enforcement services (Satyen et al., 2019). The latter may reflect greater severity and impacts of violence and/or the delaying of help-seeking until escalation and crisis points (Satyen et al., 2019; Vaughan et al., 2015). Similarly, immigrant and refugee women in Australia are generally less likely than non-immigrant women to report IPFV to authorities and access mainstream services, yet are overrepresented as users of crisis services (Vaughan et al., 2015). A recent Australian study found that while the rate of perceived need for services did not differ between migrant (68%) and non-migrant (71%) IPV victim-survivors, the rate of help-seeking from these services was significantly lower among migrants (51% vs. 67%; Satyen et al., 2021b). This may reflect increased barriers to requesting and obtaining professional assistance even after recognizing the problem and need for such support (Liang et al., 2005).
Exploratory research on help-seeking for IPV among cultural minority students indicates a general reluctance to engage with formal services (Forbes-Mewett & McCulloch, 2016; Joshi et al., 2013; Sears, 2021). In a qualitative study of service providers working with international students in the US and Australia, Forbes-Mewett and McCulloch (2016) identified barriers including fear of deportation, fear for personal and family’s safety, shame of not living up to family expectations, lack of knowledge of services and, in Australia specifically, the lack of gender-based violence education and support programs on campus. In a qualitative study of African college women in the US, Sears (2021) identified barriers related to gender norms and collectivism, including the secrecy of romantic relationships during college, pressure to secure a partner for the future, and handling problems within family networks. However, very little research has examined cross-cultural differences in tertiary students’ help-seeking needs or behaviors. A recent study reported similar rates of formal disclosure of dating violence among White (13%), Black (15%), Hispanic (12%), and other race/ethnicity (15%) college students in the US (Mennicke et al., 2021). Three of the other above-mentioned US studies included race (typically White vs. non-White) as one demographic predictor and found no significant association with the overall likelihood of help-seeking for IPV (Ameral et al., 2020; Cho & Huang, 2017; Choi et al., 2021). Beyond these broad racial comparisons, there is a paucity of data on cross-cultural patterns of help-seeking for IPFV among tertiary students nationally or internationally.
The Current Study
Despite the high prevalence and adverse impacts of IPFV among tertiary students, little research has explored help-seeking in this population and cross-cultural differences therein. Most prior work in this area has been limited to sexual assault and dating violence, overlooking the broader spectrum of violence in students’ intimate and familial relationships. In Australia, the stark lack of data on tertiary students’ help-seeking for IPFV hinders our capacity to improve intervention programs and services, and thus help mitigate the effects of victimization, in this vulnerable group. Given the immense cultural diversity of the Australian student subpopulation and population at large, an understanding of cross-cultural patterns in help-seeking is needed to improve service accessibility and utilization across diverse groups. Further, cross-cultural research should attempt to move beyond broad comparisons based on race, ethnicity, or country of birth, which do not necessarily signify affiliation with a culture. Victim-survivors’ self-identified culture may more closely reflect their alignment with a cultural group and associated norms, values, and practices, which may in turn be more closely associated with help-seeking.
To address these gaps in the literature, the current study sought to investigate formal help-seeking among women tertiary student victim-survivors of IPFV in Australia. The primary objectives were to assess the nature, extent, and cross-cultural differences in perceived need, help-seeking, and barriers to help-seeking from formal service providers. Additionally, to expand upon and advance prior research, this study aimed to examine help-seeking for IPFV defined broadly, including physical, sexual, psychological, and financial abuse from intimate partners and family members, and to assess cultural differences based on personal cultural identification.
Methods
Study Design and Sample
A quantitative cross-sectional research design was employed. Data were drawn from an online survey of tertiary students’ experiences of IPFV victimization and help-seeking since the age of 18 years. Eligibility criteria for participation were identifying as woman/female, being aged 18 years or older, currently studying at a tertiary education institution (e.g., university, college, or technical and further education [TAFE] institute) in Australia, and having sufficient English language proficiency to complete the questionnaire. The original sample comprised 1,938 participants, with 1,862 remaining after exclusions based on incorrect or missing gender, age, student status, and cultural identity. This sample was generally representative of the population of adult female tertiary education students in Australia in terms of age, state, area type, country of birth, and Indigenous status. A larger study examined the prevalence and cross-cultural differences in IPFV victimization in the full sample (Zark et al., in press). The current study focuses on help-seeking for IPFV and therefore includes the subsample of participants who reported any IPFV victimization (i.e., physical, sexual, psychological, and/or financial abuse from an intimate partner and/or family member since the age of 18). Participants who did not complete the help-seeking questionnaire (n = 10) were excluded from this study. The current sample therefore comprised 1,606 tertiary student victim-survivors of IPFV.
Measures
Sociodemographic Characteristics
Participants were asked to provide sociodemographic information including their gender identity, age, state, residential area type, employment status, tertiary institution type, domestic student status, country of birth, and cultural identity. Cultural identity was collected in free text format and categorized by Anglo status (Anglo, non-Anglo, or multicultural) and geographic region (African, American, Asian, European, Oceanian, or multicultural). Participants were classified as ‘Anglo’ if they identified with the majority culture of one or more countries in the core ‘Anglosphere’ (i.e., Australia, Canada, New Zealand, United Kingdom, US), as ‘non-Anglo’ if they identified with the culture of one or more countries outside the Anglosphere or as Indigenous, and as ‘multicultural’ if they identified with a mix of Anglo and non-Anglo cultures. Region-based classifications were determined using the United Nations geoscheme (United Nations Statistics Division, n.d.). Participants were classified as ‘multicultural’ if they identified with the cultures of multiple regions. Free text data were cleaned and coded by one author (LZ) and confirmed with a second author (LS).
Intimate Partner and Family Violence Victimization
The IPFV questionnaire was adapted from the Family and Relationship Experiences and Attitudes Among College Students Survey (Gover et al., 2008) and the 2016 Personal Safety Survey (ABS, 2017). Intimate partners were defined in the survey as “Anyone you have or had an intimate relationship with, for example: husbands, wives, boyfriends, girlfriends, dating partners, and sexual partners”, and family members were defined as “Anyone in your immediate or extended family, for example: fathers, mothers, grandfathers, grandmothers, sons, daughters, grandsons, granddaughters, brothers, sisters, uncles, aunties, nephews, nieces, cousins, in-laws, and people who are like family”. Participants were asked “Since the age of 18 years, has a partner or family member done any of the following things to you?”, followed by a list of behavioral items that assessed: physical abuse (e.g., “Thrown something at you that could hurt”, “Pushed or shoved you”); sexual abuse, including sexual assault (e.g., “Used force (like hitting, holding down, or using a weapon) to make you have sex”) and sexual harassment (e.g., “Indecently exposed themselves to you”); psychological abuse, including verbal abuse (e.g., “Insulted or swore at you”) and controlling behavior (e.g., “Prevented you from seeing family or friends”); and financial abuse, including control of finances (e.g., “Controlled or tried to control your income or assets”) and property damage (e.g., “Damaged, destroyed or stolen any of your property”). Participants could select “Partner”’ and/or “Family member” or “Neither” for each item. For the current study, perpetrator type was categorized into three groups: intimate partner(s) only, family member(s) only, and intimate partner(s) and family member(s). Due to small numbers of participants reporting only one form of abuse, abuse type was also categorized into three groups: physical/sexual abuse only, psychological/financial abuse only, and physical/sexual and psychological/financial abuse.
Help-Seeking
The Help-Seeking Behavior Scale was adapted from Lewis (2002). To assess formal help-seeking needs and behaviors, participants were asked “With regards to your relationship or family situation, have you ever needed any of the following types of services and have you ever sought out (asked for) any of them?”, followed by a list of 10 service providers (e.g., “Psychologist/counsellor”; “Doctor”, “Lawyer”). Participants could select “Needed” and/or “Asked” for each item, producing a score of 0 (No) or 1 (Yes) for Perceived Need and Help-Seeking for individual service providers and overall. If participants reported that they had sought help from a service, they were assumed to have also needed help from that service and received a score of 1 for both variables. The Perceived Need variable therefore denotes having needed help regardless of whether help was sought, while the Help-Seeking variable denotes having needed and sought help. The discrepancy between Perceived Need and Help-Seeking represents those who needed but did not seek help. Both scales demonstrated good reliability in the current sample: Perceived Need α = 0.87; Help-Seeking α = 0.82.
To assess barriers to help-seeking, participants were asked “If you were or are not willing to ask for assistance for your relationship or family situation, please indicate the reasons why”, followed by a list of 23 barriers (e.g., “You feared/fear an increase in violence”, “You were/are embarrassed”, “You were/are worried about your finances”). Participants could select all options that applied, producing a score of 0 (No) or 1 (Yes) for individual barriers and overall. Barriers were categorized as attitudinal/normative or structural/environmental: the former included perceptions and beliefs about the violence, perceptions and beliefs about the perpetrator, and social stigma; the latter included lack of knowledge/information, lack of material resources, and potential consequences. The Barriers scale also demonstrated high internal consistency: α = 0.87.
Procedure
Ethics approval was obtained from the Deakin University Human Research Ethics Committee. The survey was administered online using Qualtrics software and was open from February to September 2020. Participants were recruited via posts in student Facebook groups. During the first half of the recruitment period, general student groups were targeted (e.g., groups associated with major universities and TAFEs in each state); during the second half of the recruitment period, ethnic minority and international student groups were targeted to increase the cultural diversity of the sample. Participants were required to read a plain language statement explaining the research aims and voluntary nature of participation before providing their informed consent. Several measures were put in place to minimize potential risks and maximize potential benefits of participation, including displaying an “Exit Survey” button at the top of each page, allowing participants to skip any question, not storing any data prior to survey submission, providing contact details for relevant helplines before and after the survey, and providing an electronic information sheet about IPFV services and resources in Australia.
Data Analysis
Data were analyzed using SPSS Statistics version 27. Missing data were excluded and the sample sizes for analyses are presented in the results tables. Descriptive statistics were calculated for all variables. Pearson’s chi-square tests and post-hoc z-tests with Bonferroni corrections were used to analyze differences in the rates of perceived need and help-seeking as a function of the type of perpetrator and type of abuse. Unadjusted cultural differences in perceived need, help-seeking, and barriers to help-seeking were analyzed using a series of bivariate logistic regressions with cultural identity (by Anglo status or by region) as the predictor variable and the majority cultural group (Anglo or Oceanian) as the referent category. Adjusted cultural differences were analyzed using multivariate logistic regressions including the cultural identity variables and other sociodemographic variables (i.e., gender identity, age group, residential area type, employment status, and tertiary institution type) as predictors. Other cultural variables (i.e., migrant status, domestic student status, and Indigenous status) were not included to prevent multicollinearity with the primary predictors. All predictors were entered into the models simultaneously and associations were assessed using Wald statistics, odds ratios (ORs), and 95% confidence intervals (CIs). For individual service providers and barriers, only broad chi-square comparisons between the majority (Anglo) and minority (non-Anglo and multicultural) groups were performed due to small cell sizes. Results were considered statistically significant if p < .05, except for post-hoc pairwise comparisons where Bonferroni corrections were applied.
Assumptions for chi-square and logistic regression analyses were verified prior to testing. All expected cell frequencies were greater than one and at least 80% were greater than five. Regression diagnostics confirmed the absence of outliers (standardized residuals > ±1.96) and influential cases (Cook’s distance > 1.00 or DFBeta > ±1.00; Field, 2018). The standard errors of beta coefficients were within normal ranges, confirming the absence of complete separation and overdispersion (Field, 2018). Collinearity diagnostics confirmed the absence of multicollinearity in the multivariate models (variance inflation factors ≥ 10, condition indices ≥ 30, and variance proportions ≥ 50%; Belsley et al., 1980; Field, 2018). As the two cultural identity variables (i.e., Anglo status and region) were not collinear, both were included in the same multivariate models to assess their relative predictive utility for the help-seeking outcomes.
Results
Participants
The sample characteristics are presented in Table 1. Participants were aged 18 to 70 years (M = 27.24, SD = 8.57), with half (50.6%) aged 18 to 24 years. Most were cisgender women (96.9%), living in urban areas (73.8%), studying at a university or college (89.8%), and employed part-time or casually (48.2%) or unemployed (35.7%). Most (70.5%) participants identified with Anglo cultures, while 23.2% identified with non-Anglo cultures and 5.5% identified with a mix of Anglo and non-Anglo cultures. Geographically, most participants identified with Oceanian cultures (70.0%), followed by Asian (14.4%), European (5.3%), American (1.7%) and African (1.4%) cultures, and 6.9% identified with the cultures of multiple regions. The sociodemographic characteristics of this subsample of IPFV victim-survivors generally reflect those of the full sample including victims and non-victims (see Zark et al., in press).
Perceived Need and Help-Seeking
The rates of perceived need and help-seeking from service providers are presented in Table 2 in descending order of frequency. Two thirds (66.2%) of participants perceived a need for formal help, yet less than half (48.7%) had sought such help. This left 17.6% of the sample, and 26.5% of those who perceived a need for help, not having sought any services despite feeling they needed them. Psychologists and counsellors were by far the most common source of support, with approximately three in five (59.2%) participants having needed and two in five (37.5%) having sought their help. This was followed by financial services, doctors, police, and domestic violence helplines, each of which were needed by 23–30% and sought by 10–19% of the sample. Fewer participants reported needing or seeking help from support groups, legal aid, lawyers, women’s shelters, and hospitals (9–18% needed, 5–10% sought). Cultural minority students were significantly less likely to have needed and sought help from psychologists/counsellors (p < .001), doctors (p = .036), police (p < .001), lawyers (p = .013), legal aid (p = .005), and financial services (p < .001) than the majority.
The rates of perceived need and help-seeking by the type of perpetrator and type of abuse are presented in Table 3. Perpetrator type was significantly associated with perceived need and help-seeking (both ps < .001). Participants who reported violence by a family member(s) only were significantly less likely to perceive a need for help (52.5%) and to seek help (37.0%) than those who reported violence by an intimate partner(s) only (68.6% needed, 49.5% sought) and those who reported violence by both an intimate partner(s) and family member(s) (71.0% needed, 54.6% sought; all Bonferroni-corrected ps < .017). Abuse type was also significantly associated with perceived need and help-seeking (both ps < .001). Participants who reported both physical/sexual and psychological/financial abuse were significantly more likely to perceive a need for help (73.4%) and to seek help (54.0%) than those who reported physical/sexual abuse only (31.0% needed, 22.4% sought) and those who reported psychological/financial abuse only (40.9% needed, 30.2% sought; all Bonferroni-corrected ps < .017).
Cultural identity was a significant predictor of perceived need and help-seeking in the bivariate logistic regression analyses (Table 4). Non-Anglo-identifying students had 41% lower odds (p < .001) of perceiving a need for help and 44% lower odds (p < .001) of seeking help than Anglo-identifying students, while multicultural students did not significantly differ from the majority. With regard to regional groups, Asian-identifying students had 54% lower odds (p < .001) of perceiving a need for help and 57% lower odds (p < .001) of seeking help than Oceanian-identifying students. Additionally, African-identifying students had 72% lower odds (p = .013), and American-identifying students had 67% lower odds (p = .012), of seeking help than Oceanian-identifying students, despite no significant differences in their perceived need. European and multicultural-identifying students did not significantly differ from the majority.
Cultural differences based on regional groupings, but not Anglo groupings, remained significant in the multivariate analyses of perceived need and help-seeking adjusted for gender identity, age group, residential area type, employment status, and tertiary institution type (Table 5). The odds of perceiving a need for help were 57% lower among Asian-identifying students (p = .011) compared to Oceanian-identifying students. The odds of seeking help were 75% lower among African-identifying students (p = .018), 71% lower among American-identifying students (p = .010), and 62% lower among Asian-identifying students (p = .002), compared to Oceanian-identifying students. Beyond culture, the multivariate models indicated that gender, age, employment, and institution were significant predictors of perceived need and help-seeking. Specifically, trans and non-binary women, 25–34 and 35-44-year-olds, and full-time workers were significantly more likely to have needed help and to have sought help than cisgender women, 18-24-year-olds, and part-time/casual/self-employed workers, respectively. Over 45-year-olds and TAFE students were significantly more likely to have needed help than 18-24-year-olds and university/college students, though their likelihood of seeking help did not significantly differ.
Barriers to Help-Seeking
The rates of barriers to help-seeking are presented in Table 6 in descending order of frequency. Most (65.5%) participants endorsed at least one barrier to seeking services. Three in five (62.1%) reported attitudinal/normative barriers, the most common being not perceiving the violence as serious enough (38.4%), embarrassment (32.5%), and love for the perpetrator (28.4%). Two in five (41.9%) reported structural/environmental barriers, the most common being concerns about finances (22.2%), fear of increased violence (21.8%), and not knowing how to contact the service (13.9%). Among participants who had needed but not sought help, 85.2% endorsed any barriers (80.6% reported attitudinal/normative barriers and 58.3% reported structural/environmental barriers). The most common barriers in this subgroup were consistent with those in the full sample, though reported at higher rates (see Table 6).
Anglo-identifying students were significantly more likely than non-Anglo and multicultural-identifying students to report the following barriers to seeking help: not perceiving the violence as serious enough (p = .002), embarrassment (p < .001), concerns about not being believed (p < .001), fear of increased violence (p = .005), potential harm from the perpetrator (p = .003), and fear of losing children (p = .018). Conversely, non-Anglo and multicultural-identifying students were significantly more likely than Anglo-identifying students to report the following barriers: concerns about losing respect from other members of their culture, religious or moral beliefs, fear of deportation, visa concerns, and lack of access to culturally appropriate services (all ps < .001). The rates of the remaining barriers did not significantly differ between the majority and minority cultural groups (see Table 6).
Cultural identity did not have a significant effect on barriers to help-seeking in the bivariate or multivariate logistic regression analyses (Tables 4 and 5). The multivariate model including other sociodemographic variables indicated that trans and non-binary women, older women (25–34, 35–44, and ≥ 45-year-old), and TAFE students were significantly more likely to report any barriers to help-seeking than cisgender women, 18-24-year-olds, and university/college students, respectively.
Discussion
This paper presents the first study of formal help-seeking among women tertiary student victim-survivors of IPFV in Australia. Less than half (48.7%) of participants reported that they had sought help from services, despite a larger proportion (66.2%) indicating that they needed such help. Two thirds (65.5%) of participants reported experiencing barriers to help-seeking. Cultural minority students were generally less likely to report having needed and sought help than the majority. The findings are interpreted and integrated with the current literature below.
Perceived Need, Help-Seeking, and Barriers
The overall rates of perceived need and help-seeking from this study are consistent with those from a recent Australian population-based study of women’s help-seeking for IPV, wherein a median of 64% reported needing services and 47% reported seeking services over a four-year period (Satyen et al., 2021b). However, the overall rate of formal help-seeking found here is higher than that reported in US studies of college student victim-survivors of IPV (9–23%; Addington, 2021; Ameral et al., 2020; Cho & Huang, 2017), which may be partially attributable to the wider range of services examined here.
The pattern of help-seeking from different service providers in our sample is consistent with international data indicating that student victim-survivors more frequently seek help from health and counselling professionals and less frequently from police and legal professionals (e.g., Cho & Huang, 2017; Choi et al., 2021). The observed rates of help-seeking from doctors, police, lawyers, helplines, and shelters are similar to those among IPV victim-survivors in the general Australian population, while the rates of help-seeking from psychologists/counsellors and financial services are considerably higher (38% vs. 16% and 19% vs. 4%, respectively; ABS, 2018b). This may reflect greater emotional and financial strain and/or greater mental health awareness in the student subpopulation. However, variability in findings may also be due to methodological differences, particularly our broader examination of help-seeking for IPFV rather than only IPV, and for any incident of violence rather than only the most recent.
The type of perpetrator and type of abuse appeared to influence students’ help-seeking perceptions and behaviors. Rates of perceived need and help-seeking were lower among those who had been victimized by family members than those who had been victimized by intimate partners, which may reflect poorer recognition of family violence and thus the need for increased research and public attention to the issue. Rates of perceived need and help-seeking were similar among those who had experienced physical/sexual abuse only and those who had experienced psychological/financial abuse only, and higher among those who had experienced both physical/sexual and psychological/financial abuse. On the one hand, these findings are promising given that polyvictimization increases the likelihood of adverse health outcomes (e.g., Sabina & Straus, 2008) and thus the importance of professional assistance; on the other hand, they highlight opportunities to promote students’ rights to seek support for any victimization experience, and thus potentially decrease the risk of multiple exposures and cumulative impacts.
The majority of participants identified specific barriers to formal help-seeking, which were more often attitudinal or normative (62.1%) than structural or environmental (41.9%) in nature. The most common barriers were the perception that the violence was not serious enough, embarrassment, love for the perpetrator, and a desire to keep the matter private. This was consistent for the full sample and for the subgroup who indicated that they had needed but not sought any help. Additionally, lack of perceived need can itself be conceptualized as a barrier; as per Liang et al.’s (2005) model, recognition of the problem and need for assistance is an important precursor to help-seeking. The most prevalent barriers in the current study overlap with those found in previous IPV research: among women in Australia, these include not perceiving the problem as serious enough, feeling they could deal with it themselves, not wanting or needing help, and shame or embarrassment (ABS, 2018a, 2018c); among American college students, these include perceiving the matter as private or personal and perceiving the violence as not serious or important enough for services (Ameral et al., 2020; Cho et al., 2020a; Choi et al., 2021). These individual perceptions and attitudes towards IPFV likely reflect broader social norms, practices, and structures supportive of violence against women at the community, system, and societal levels (UN Women, 2015; Webster et al., 2018).
Cross-Cultural Differences
The overall rates of perceived need and help-seeking differed by cultural identity. Students who identified as non-Anglo were less likely to report having needed and sought help than those who identified as Anglo in the unadjusted analyses. Students who identified as African, American, and Asian were less likely to report having sought help than those who identified as Oceanian in the unadjusted and adjusted analyses. Interpreted in the context of Liang et al.’s (2005) model, some cultural minority students may be less likely to appraise IPFV as a problem that requires professional assistance (Stage 1), leading to lower rates of perceived need; and even after perceiving such need, an interplay of factors may lead to the decision not to seek help (Stage 2), or at least not from formal services (Stage 3), and thus lower rates of help-seeking.
As this study examined cross-cultural differences based on participants’ cultural identification rather than their race, ethnicity, or country of birth, the results cannot be directly compared to past research. In general, however, cultural differences appear to be more prominent here than in previous studies. In Australia, Satyen et al. (2021b) found lower crude rates of help-seeking for IPV among migrant women compared to non-migrant women, but no such differences in perceived need. Further, migrant status did not have a significant effect on either outcome in the multivariate analysis adjusted for other sociodemographic factors (Satyen et al., 2021b). In the US, recent studies have reported no association between race/ethnicity and help-seeking for IPV in the general population (e.g., Cho et al., 2020b) and student population (e.g., Choi et al., 2021; Mennicke et al., 2021). It is therefore possible that cultural self-identification is more closely associated with help-seeking than such other cultural variables. Of course, an individual’s cultural identity is multifaceted and may be shaped by a range of factors including their race, ethnicity, nationality, language, religion, and subscription to cultural norms, values, and practices. Further research is therefore needed to clarify the specific aspects of culture that influence victim-survivors’ help-seeking for IPFV.
In relation to help-seeking from different service types, the extant literature indicates that women from cultural minority backgrounds are generally less likely to utilize mental health and social services, yet more likely to utilize law enforcement and emergency services, than the majority (Satyen et al., 2019; Vaughan et al., 2015). However, this distinction was not evident in our results, as non-Anglo and multicultural-identifying students were less likely to have sought help from almost all service providers (psychologists/counsellors, doctors, police, lawyers, legal aid, and financial services) than Anglo-identifying students, and equally unlikely to have sought help from the less commonly utilized services (helplines, support groups, hospitals, and shelters). This study is the first to analyze cross-cultural variation in tertiary students’ help-seeking from different service providers, and patterns in this cohort may differ from the general population. Still, it is possible that cultural minority students, as per cultural minority women more broadly, are more likely to delay help-seeking until escalation and crisis (Satyen et al., 2019; Vaughan et al., 2015), and their pathways to help-seeking from different services require further study.
Given the observed cultural differences in help-seeking behavior, it is surprising that cultural identity was not associated with the likelihood of reporting any barriers to help-seeking. While cultural differences in perceived need may also contribute to these discrepancies, some minority groups demonstrated lower rates of help-seeking despite similar rates of perceived need to the majority, suggesting that other factors are at play. Of course, only a selection of common barriers was assessed in this study. Students who identified as non-Anglo or multicultural were more likely than those who identified as Anglo to endorse barriers related to respect from other members of their culture, religious or moral beliefs, visa status, fear of deportation, and lack of culturally appropriate services. Yet, many other structural and sociocultural barriers were not examined, including fear of cultural misrepresentation and stereotyping, fear and distrust of authorities and services, language difficulties, cultural norms regarding gender roles and relations, family expectations and community pressures, and social isolation. More broadly, it is difficult to operationalize and quantitatively analyze the intersecting forms of oppression and discrimination that contribute to cultural inequalities in IPFV and help-seeking (Our Watch, 2021). Nevertheless, all efforts to understand and address these disparities must remain cognizant of this broader social context.
Limitations
The findings from this study must be in the interpreted in the context of its limitations. First, the use of a convenience sample limits the generalizability of the results to the wider population of women tertiary students in Australia. Our recruitment methods restricted the sample to students with internet access, an active Facebook profile, and active participation in targeted Facebook groups. The survey examined help-seeking from formal services only, yet informal help-seeking may be particularly important for students and cultural minority groups (Cho et al., 2020b; Sabina & Ho, 2014) and warrants further research in the Australian context. It should also be noted that this study examined IPFV victimization and help-seeking during adulthood (≥18 years) in order to maintain focus on violence against women without incorporating child abuse. Still, such violence, particularly that perpetrated by family members, may have begun prior to age 18, and further research is needed to understand women’s pathways to help-seeking in the context of prolonged victimization. While men can also experience all forms of IPFV, the dynamics and drivers of such violence fundamentally differ (Our Watch, 2021), and men’s victimization and help-seeking were therefore not examined here.
Several cultural limitations of this study must also be considered. Some cultural identity groups in the sample had low numbers, particularly the African (n = 22) and American (n = 28) groups, and their results should therefore be interpreted with caution. Each minority group was compared to the majority group only, and for individual service providers and barriers, only broad comparisons between students identifying as Anglo and as non-Anglo or multicultural were made due to small cell sizes. It is important to reiterate that these groups are by no means homogeneous, and while cultural minority status may give rise to some shared influences and challenges in relation to IPFV and help-seeking, there is immense diversity between and within minority groups (Kasturirangan et al., 2004). Finally, our cross-sectional data provide evidence of association only and do not support causal inferences; further research is needed to clarify the factors and processes that mediate associations between cultural identity and help-seeking.
Implications
Policy and Practice
The findings from this study highlight the need for concerted efforts to increase formal help-seeking among student victim-survivors of IPFV. Tertiary education providers have an important role to play in this through education, advocacy, and service provision. Education campaigns and programs have the potential to improve awareness of violence and help-seeking (Donovan & Vlais, 2005) and may therefore constitute an important foundational step. Such programs should address the nature and impacts of IPFV comprehensively, attending to less well recognized forms (e.g., violence from family members, psychological and financial abuse) and emphasizing the seriousness of any incidence of violence. Students should be made aware of the available support options and how to access them. Given the wide-ranging impacts of IPFV, including on physical, psychological, social, occupational, and academic functioning (e.g., AIHW, 2019; Brewer et al., 2018; Dillon et al., 2013), a wide range of services should be promoted with explanations of the types of assistance they can provide. Continued efforts are needed to improve the accessibility and effectiveness of support services for student victim-survivors of IPFV. Staff in these services, particularly health and counselling services, should be trained in screening for IPFV, providing trauma-informed responses to disclosure, and providing referrals and supporting students in navigating complex service systems.
The lower rates of help-seeking among cultural minority students may place this group at increased risk of further victimization and its cumulative impacts. Given the immense cultural diversity of the Australian tertiary student population, addressing cultural inequalities in help-seeking and improving the cultural responsiveness of support services should be of high priority. Students should be informed about culturally specific services and, where applicable, the cultural sensitivity of mainstream services. Minority students should see themselves represented in IPFV services and resources, for example, through culturally inclusive terminology and images, the provision of information in a range of languages, and culturally diverse personnel. Cultural competence and cultural humility are critical for professionals working with culturally diverse victim-survivors (Bent-Goodley, 2005; Kasturirangan et al., 2004; Sokoloff & Dupont, 2005), and our findings suggest that this may be particularly important for psychologists and counsellors as the most highly sought service providers among minority students. Cultural competence requires an understanding of the intersectional factors that shape minority women’s experiences of IPFV and help-seeking, including not only cultural characteristics, norms, values, and practices, but relevant historical, social, and structural forces including discrimination and disadvantage (Our Watch, 2021; Sokoloff & Dupont, 2005). Service providers should ideally be trained in culturally sensitive assessment and intervention and equipped to provide referrals to culturally specific services and resources.
Research
Given the high national and international prevalence of IPFV among tertiary students (Chan et al., 2008; Zark et al., in press), ongoing research is needed to better understand formal help-seeking in this population and thus improve service systems’ capacity to intervene and mitigate harms. Given the co-occurrence and commonalities between violence in intimate and familial relationships and among different forms of violence and abuse (Smith Slep & Heyman, 2001; Tolan et al., 2006), more integrative research on help-seeking for IPFV is needed to inform holistic understandings and combined service responses. Research should continue to clarify the individual, relationship, community/organizational, system/institutional, and societal-level factors that undermine students’ help-seeking for IPFV. Attitudinal and normative support for violence against women at all such levels may play an important role, shaping the responses of victim-survivors, perpetrators, community members, service providers, and organizations (Webster et al., 2018). Attitudinal acceptance of IPFV may contribute to low perceived need for help, low help-seeking, and many common barriers to help-seeking (Flood & Pease, 2009). Thus, examining students’ attitudes towards IPFV and cross-cultural differences therein may have important implications for understanding and improving help-seeking in this population.
Further research is needed to understand the factors that contribute to cross-cultural differences in help-seeking for IPFV, and how culture interacts with other axes of identity and oppression to shape help-seeking needs and behaviors. Research examining the role of culture should therefore consider sociodemographic and contextual factors that may mediate or moderate cross-cultural differences. Furthermore, beyond differences in the prevalence of help-seeking, research should seek to elucidate the nuances and complexities of help-seeking in cultural minority student communities, which may include culturally specific help-seeking strategies, pathways, barriers, and facilitators. Finally, most research in this area examines whether student victim-survivors have sought or utilized services, but not the outcomes of doing so. We therefore have limited insight into the effectiveness of formal supports for this population. Longitudinal research is needed to assess the effects of service use on students’ safety, health, and wellbeing. Students’ perspectives on service utility and limitations can also provide important insights for service improvement. Such insights are needed to respond more effectively to IPFV in this cohort and potentially lead change in wider society.
References
Addington, L. A. (2021). Exploring help seeking patterns for emerging adult victims using the National Intimate Partner and Sexual Violence Survey. Violence Against Women. Advance online publication. https://doi.org/10.1177/10778012211014552
Ameral, V., Palm Reed, K., & Hines, D. (2020). An analysis of help-seeking patterns among college student victims of sexual assault, dating violence, and stalking. Journal of Interpersonal Violence, 35(23–24), 5311–5335. https://doi.org/10.1177/0886260517721169
Ansara, D. L., & Hindin, M. J. (2010). Formal and informal help-seeking associated with women’s and men’s experiences of intimate partner violence in Canada. Social Science & Medicine, 70(7), 1011–1018. https://doi.org/10.1016/j.socscimed.2009.12.009
Australian Bureau of Statistics. (2017). 2016 Personal safety survey (PSS): Question specifications (Cat. No. 4906.0.55.003). https://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/C897D50E421A3E45CA2581D1000C3B49/$File/4906055003%202016%20personal%20safety%20survey%20questionnaire.pdf
Australian Bureau of Statistics. (2018a). Table 17.3: Experience of current partner violence since age 15, by sex of respondent, proportion of persons. Personal safety, Australia, 2016. https://www.abs.gov.au/statistics/people/crime-and-justice/personal-safety-australia/latest-release#. Accessed 5 Nov 2021
Australian Bureau of Statistics. (2018b). Table 18.1: Experience of previous partner violence since age 15, by sex of respondent, estimate. Personal safety, Australia, 2016. https://www.abs.gov.au/statistics/people/crime-and-justice/personal-safety-australia/latest-release#. Accessed 5 Nov 2021
Australian Bureau of Statistics. (2018c). Table 18.3: Experience of previous partner violence since age 15, by sex of respondent, proportion of persons. Personal safety, Australia, 2016. https://www.abs.gov.au/statistics/people/crime-and-justice/personal-safety-australia/latest-release#. Accessed 5 Nov 2021
Australian Human Rights Commission. (2014). Violence against women. https://humanrights.gov.au/our-work/sex-discrimination/projects/violence-against-women
Australian Institute of Health and Welfare. (2019). Family, domestic and sexual violence in Australia: Continuing the national story 2019 (Cat. No. FDV 3). https://www.aihw.gov.au/getmedia/b0037b2d-a651-4abf-9f7b-00a85e3de528/aihw-fdv3-FDSV-in-Australia-2019.pdf.aspx?inline=true
Banyard, V. L., Demers, J. M., Cohn, E. S., Edwards, K. M., Moynihan, M. M., Walsh, W. A., & Ward, S. K. (2020). Academic correlates of unwanted sexual contact, intercourse, stalking, and intimate partner violence: An understudied but important consequence for college students. Journal of Interpersonal Violence, 35(21–22), 4375–4392. https://doi.org/10.1177/0886260517715022
Barrett, B. J., & St Pierre, M. (2011). Variations in women’s help seeking in response to intimate partner violence: Findings from a Canadian population-based study. Violence Against Women, 17(1), 47–70. https://doi.org/10.1177/1077801210394273
Belsley, D. A., Kuh, E., & Welsch, R. E. (1980). Regression diagnostics: Identifying influential data and sources of collinearity. Wiley.
Bent-Goodley, T. B. (2005). Culture and domestic violence: Transforming knowledge development. Journal of Interpersonal Violence, 20(2), 195–203. https://doi.org/10.1177/0886260504269050
Brewer, N., Thomas, K. A., & Higdon, J. (2018). Intimate partner violence, health, sexuality, and academic performance among a national sample of undergraduates. Journal of American College Health, 66(7), 683–692. https://doi.org/10.1080/07448481.2018.1454929
Chan, K. L., Straus, M. A., Brownridge, D. A., Tiwari, A., & Leung, W. C. (2008). Prevalence of dating partner violence and suicidal ideation among male and female university students worldwide. Journal of Midwifery & Women’s Health, 53(6), 529–537. https://doi.org/10.1016/j.jmwh.2008.04.016
Cho, H., & Huang, L. (2017). Aspects of help seeking among collegiate victims of dating violence. Journal of Family Violence, 32(4), 409–417. https://doi.org/10.1007/s10896-016-9813-3
Cho, H., Seon, J., Choi, G. Y., An, S., Kwon, I., Choi, Y. J., & Yun, S. H. (2020a). Gender differences in intimate partner violence victimization, help-seeking, and outcomes among college students. Advances in Social Work, 20(1), 22–44. https://doi.org/10.18060/23675
Cho, H., Shamrova, D., Han, J. B., & Levchenko, P. (2020b). Patterns of intimate partner violence victimization and survivors’ help-seeking. Journal of Interpersonal Violence, 35(21/22), 4558–4582. https://doi.org/10.1177/0886260517715027
Choi, Y. J., Rai, A., Cho, H., Son, E., An, S., & Yun, S. H. (2021). Help-seeking behaviors for intimate partner violence among college students: Implications for intimate partner violence prevention and intervention. Violence and Victims, 36(4), 548–564. https://doi.org/10.1891/VV-D-20-00124
Coker, A. L., Watkins, K. W., Smith, P. H., & Brandt, H. M. (2003). Social support reduces the impact of partner violence on health: Application of structural equation models. Preventive Medicine, 37(3), 259–267. https://doi.org/10.1016/s0091-7435(03)00122-1
Crenshaw, K. (1991). Mapping the margins: Intersectionality, identity politics, and violence against women of color. Stanford Law Review, 43(6), 1241–1299
Day, A., Casey, S., Gerace, A., Oster, C., & O’Kane, D. (2018). The forgotten victims: Prisoner experience of victimisation and engagement with the criminal justice system (Research Report, 01/2018). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/02/Day-et-al-Research-Report-The-Forgotten-Victims-1.pdf
Demers, J. M., Ward, S. K., Walsh, W. A., Banyard, V. L., Cohn, E. S., Edwards, K. M., & Moynihan, M. M. (2018). Disclosure on campus: Students’ decisions to tell others about unwanted sexual experiences, intimate partner violence, and stalking. Journal of Aggression, Maltreatment & Trauma, 27(1), 54–75. https://doi.org/10.1080/10926771.2017.1382631
Department of Social Services. (2015). Hearing her voice: Report from the kitchen table conversations with culturally and linguistically diverse women on violence against women and their children. Commonwealth of Australia. https://plan4womenssafety.dss.gov.au/wp-content/uploads/2015/07/cald_womens_safety_report.pdf
Dichter, M. E., & Rhodes, K. V. (2011). Intimate partner violence survivors’ unmet social service needs. Journal of Social Service Research, 37(5), 481–489. https://doi.org/10.1080/01488376.2011.587747
Dillon, G., Hussain, R., Loxton, D., & Rahman, S. (2013). Mental and physical health and intimate partner violence against women: A review of the literature. International Journal of Family Medicine, 2013, 313909. https://doi.org/10.1155/2013/313909
Donovan, R. J., & Vlais, R. (2005). VicHealth review of communication components of social marketing/public education campaigns focusing on violence against women.Victorian Health Promotion Foundation. https://www.vichealth.vic.gov.au/-/media/ProgramsandProjects/DiscriminationandViolence/ViolenceAgainstWomen/CAS_Paper2_SocialMarketing.pdf?la=en&hash=E3ACDD35D61F32047979415F214A4A42637A9DD6
Duval, A., Lanning, B. A., & Patterson, M. S. (2020). A systematic review of dating violence risk factors among undergraduate college students. Trauma, Violence, & Abuse, 21(3), 567–585. https://doi.org/10.1177/1524838018782207
Edwards, K. M., Dardis, C. M., & Gidycz, C. A. (2012). Women’s disclosure of dating violence: A mixed methodological study. Feminism & Psychology, 22(4), 507–517. https://doi.org/10.1177/0959353511422280
Femi-Ajao, O., Kendal, S., & Lovell, K. (2020). A qualitative systematic review of published work on disclosure and help-seeking for domestic violence and abuse among women from ethnic minority populations in the UK. Ethnicity & Health, 25(5), 732–746. https://doi.org/10.1080/13557858.2018.1447652
Field, A. (2018). Discovering statistics using IBM SPSS statistics (5th ed.). Sage.
Flood, M., & Pease, B. (2009). Factors influencing attitudes to violence against women. Trauma, Violence, & Abuse, 10(2), 125–142. https://doi.org/10.1177/1524838009334131
Forbes-Mewett, H., & McCulloch, J. (2016). International students and gender-based violence. Violence Against Women, 22(3), 344–365. https://doi.org/10.1177/1077801215602344
Goodson, A., & Hayes, B. E. (2021). Help-seeking behaviors of intimate partner violence victims: A cross-national analysis in developing nations. Journal of Interpersonal Violence, 36(9–10). NP4705-NP4727. https://doi.org/10.1177/0886260518794508.NP4705-NP4727
Gover, A. R., Kaukinen, C., & Fox, K. A. (2008). The relationship between violence in the family of origin and dating violence among college students. Journal of Interpersonal Violence, 23(12), 1667–1693. https://doi.org/10.1177/0886260508314330
Hulley, J., Bailey, L., Kirkman, G., Gibbs, G. R., Gomersall, T., Latif, A., & Jones, A. (2022). Intimate partner violence and barriers to help-seeking among Black, Asian, minority ethnic and immigrant women: A qualitative metasynthesis of global research. Trauma, Violence, & Abuse. Advance online publication. https://doi.org/10.1177/15248380211050590
Ingram, E. M. (2007). A comparison of help seeking between Latino and non-Latino victims of intimate partner violence. Violence Against Women, 13(2), 159–171. https://doi.org/10.1177/1077801206296981
Joshi, M., Thomas, K. A., & Sorenson, S. B. (2013). Domestic violence and international students: An exploratory study of the practices and role of US university international offices. Journal of College Student Development, 54(5), 527–533. https://doi.org/10.1353/csd.2013.0080
Kasturirangan, A., Krishnan, S., & Riger, S. (2004). The impact of culture and minority status on women’s experience of domestic violence. Trauma, Violence, & Abuse, 5(4), 318–332. https://doi.org/10.1177/1524838004269487
Kaukinen, C. (2004). The help-seeking strategies of female violent-crime victims: The direct and conditional effects of race and the victim-offender relationship. Journal of Interpersonal Violence, 19(9), 967–990. https://doi.org/10.1177/0886260504268000
Kaukinen, C. (2014). Dating violence among college students: The risk and protective factors. Trauma, Violence, & Abuse, 15(4), 283–296. https://doi.org/10.1177/1524838014521321
Lelaurain, S., Graziani, P., & Lo Monaco, G. (2017). Intimate partner violence and help-seeking: A systematic review and social psychological tracks for future research. European Psychologist, 22(4), 263–281. https://doi.org/10.1027/1016-9040/a000304
Lewis, S. F. (2002). An investigation of help-seeking behavior in battered women [Doctoral dissertation, West Virginia University]. ProQuest Dissertations Publishing.
Liang, B., Goodman, L., Tummala-Narra, P., & Weintraub, S. (2005). A theoretical framework for understanding help-seeking processes among survivors of intimate partner violence. American Journal of Community Psychology, 36(1/2), 71–84. https://doi.org/10.1007/s10464-005-6233-6
Lövestad, S., Vaez, M., Löve, J., Hensing, G., & Krantz, G. (2021). Intimate partner violence, associations with perceived need for help and health care utilization: A population-based sample of women in Sweden. Scandinavian Journal of Public Health, 49(3), 268–276. https://doi.org/10.1177/1403494820930952
Lu, M., Mangahas, X., & Nimmo, J. (2020). Domestic and family violence in Culturally and Linguistically Diverse (CALD) communities. University of Queensland Pro Bono Centre. https://law.uq.edu.au/files/53963/Domestic%20%26%20Family%20Violence%20in%20CALD%20Communities.pdf
McCart, M. R., Smith, D. W., & Sawyer, G. K. (2010). Help seeking among victims of crime: A review of the empirical literature. Journal of Traumatic Stress, 23(2), 198–206. https://doi.org/10.1002/jts.20509
Mennicke, A., Coates, C. A., Jules, B., & Langhinrichsen-Rohling, J. (2021). Who do they tell? College students’ formal and informal disclosure of sexual violence, sexual harassment, stalking, and dating violence by gender, sexual identity, and race. Journal of Interpersonal Violence. Advance online publication. https://doi.org/10.1177/08862605211050107
Mitra-Kahn, T., Newbigin, C., & Hardefeldt, S. (2016). Invisible women, invisible violence: Understanding and improving data on the experiences of domestic and family violence and sexual assault for diverse groups of women: State of knowledge paper (ANROWS Landscapes, DD01/2016). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/02/DiversityData_UPDATED191216.pdf
Moylan, C. A., & Javorka, M. (2020). Widening the lens: An ecological review of campus sexual assault. Trauma, Violence, & Abuse, 21(1), 179–192. https://doi.org/10.1177/1524838018756121
Multicultural Centre for Women’s Health. (2020). Challenging myths about culture and violence. https://www.mcwh.com.au/wp-content/uploads/Challenging-Myths-210617-FINAL.pdf
Our Watch. (2021). Change the story: A shared framework for the primary prevention of violence against women in Australia (2nd ed.). https://media-cdn.ourwatch.org.au/wp-content/uploads/sites/2/2021/11/23131846/Change-the-story-Our-Watch-AA.pdf
Pham, T. T. L., Berecki-Gisolf, J., Clapperton, A., O’Brien, K. S., Liu, S., & Gibson, K. (2021). Definitions of Culturally and Linguistically Diverse (CALD): A literature review of epidemiological research in Australia. International Journal of Environmental Research and Public Health, 18(2), 737–760. https://doi.org/10.3390/ijerph18020737
Ravi, K. E., Robinson, S. R., & Schrag, R. V. (2021). Facilitators of formal help-seeking for adult survivors of IPFV in the United States: A systematic review. Trauma, Violence, & Abuse. Advance online publication. https://doi.org/10.1177/1524838021995954
Rennison, C. M., & Addington, L. A. (2014). Violence against college women: A review to identify limitations in defining the problem and inform future research. Trauma, Violence, & Abuse, 15(3), 159–169. https://doi.org/10.1177/1524838014520724
Rickwood, D., Deane, F. P., Wilson, C. J., & Ciarrochi, J. (2014). Young people’s help-seeking for mental health problems. Australian e-Journal for the Advancement of Mental Health, 4(3), 218–251. https://doi.org/10.5172/jamh.4.3.218
Robinson, S. R., Ravi, K., & Voth Schrag, R. J. (2020). A systematic review of barriers to formal help seeking for adult survivors of IPV in the United States, 2005–2019. Trauma, Violence, & Abuse. Advance online publication. https://doi.org/10.1177/1524838020916254
Sabina, C., & Ho, L. Y. (2014). Campus and college victim responses to sexual assault and dating violence: Disclosure, service utilization, and service provision. Trauma, Violence, & Abuse, 15(3), 201–226. https://doi.org/10.1177/1524838014521322
Sabina, C., & Straus, M. A. (2008). Polyvictimization by dating partners and mental health among U.S. college students. Violence and Victims, 23(6), 667–682. https://doi.org/10.1891/0886-6708.23.6.667
Satyen, L. (2021). Gender norms in the Indian migrant community in Australia: Family, community, and work roles. Journal of Gender Studies, 30(4), 452–464. https://doi.org/10.1080/09589236.2021.1884535
Satyen, L., Dort, J., & Yin, S. (2020). Gender norms in the Chinese community in Melbourne, Australia: Family and community roles. Australian Psychologist, 55(1), 50–61. https://doi.org/10.1111/ap.12402
Satyen, L., Piedra, S., Ranganathan, A., & Golluccio, N. (2018). Intimate partner violence and help-seeking behavior among migrant women in Australia. Journal of Family Violence, 33(7), 447–456. https://doi.org/10.1007/s10896-018-9980-5
Satyen, L., Rogic, A. C., & Supol, M. (2019). Intimate partner violence and help-seeking behaviour: A systematic review of cross-cultural differences. Journal of Immigrant and Minority Health, 21(4), 879–892. https://doi.org/10.1007/s10903-018-0803-9
Satyen, L., Supol, M., Ranganathan, A., & Toumbourou, J. W. (2021a). International and cross-cultural research on men’s violence against female intimate partners. In T. K. Shacklelford (Ed.), The SAGE handbook of domestic violence (pp.40–60). SAGE Publications. https://doi.org/10.4135/9781529742343.n3
Satyen, L., Toumbourou, J. W., Heerde, J., Supol, M., & Ranganathan, A. (2021b). The Royal Commission into Family Violence: Trends in the reporting of intimate partner violence and help-seeking behavior. Journal of Interpersonal Violence, 36(23–24), 11009–11034. https://doi.org/10.1177/0886260519897341
Sawrikar, P., & Katz, I. (2009). How useful is the term “Culturally and Linguistically Diverse (CALD)” in the Australian social policy discourse?. University of New South Wales Social Policy Research Centre. https://apo.org.au/sites/default/files/resource-files/2009-07/apo-nid17673.pdf
Scherer, H. L., Snyder, J. A., & Fisher, B. S. (2016). Intimate partner victimization among college students with and without disabilities: Prevalence of and relationship to emotional well-being. Journal of Interpersonal Violence, 31(1), 49–80. https://doi.org/10.1177/0886260514555126
Sears, K. P. (2021). Cultural beliefs related to intimate partner violence help-seeking among African college women. Journal of Aggression, Maltreatment & Trauma, 30(7), 972–989. https://doi.org/10.1080/10926771.2021.1912874
Smith Slep, A. M., & Heyman, R. E. (2001). Where do we go from here? Moving toward an integrated approach to family violence. Aggression and Violent Behavior, 6(2–3), 353–356. https://doi.org/10.1016/S1359-1789(00)00028-8
Sokoloff, N., & Dupont, I. (2005). Domestic violence at the intersections of race, class, and gender: Challenges and contributions to understanding violence against marginalized women in diverse communities. Violence Against Women, 11(1), 38–64. https://doi.org/10.1177/1077801204271476
State of Victoria. (2016). Royal Commission into Family Violence: Report and recommendations (Vol V, Parliamentary Paper No 132). http://rcfv.archive.royalcommission.vic.gov.au/MediaLibraries/RCFamilyViolence/Reports/Final/RCFV-Vol-V.pdf
Sylaska, K. M., & Edwards, K. M. (2014). Disclosure of intimate partner violence to informal social support network members: A review of the literature. Trauma, Violence, & Abuse, 15(1), 3–21. https://doi.org/10.1177/1524838013496335
The Equality Institute. (2017). Family violence primary prevention: Building a knowledge base and identifying gaps for all manifestations of family violence. Victorian State Government. https://www.equalityinstitute.org/media/pages/projects/example-project-c/2788087480-1595397560/dpc_eqi_fv_report.pdf
Tolan, P., Gorman-Smith, D., & Henry, D. (2006). Family violence. Annual Review of Psychology, 57, 557–583. https://doi.org/10.1146/annurev.psych.57.102904.190110
UN Women. (2015). A framework to underpin action to prevent violence against women. https://www.unwomen.org/sites/default/files/Headquarters/Attachments/Sections/Library/Publications/2015/Prevention_Framework_unwomen_nov2015.pdf
Ung, S. (2015, August 31). Integrating culture into psychological research. Observer, 28(7). https://www.psychologicalscience.org/observer/integrating-culture-into-psychological-research
United Nations Statistics Division. (n.d.). Methodology: Standard country or area codes for statistical use (M49). https://unstats.un.org/unsd/methodology/m49/
Vaughan, C., Davis, E., Murdolo, A., Chen, J., Murray, L., Block, K. … Warr, D. (2015). Promoting community-led responses to violence against immigrant and refugee women in metropolitan and regional Australia: The ASPIRE Project: State of knowledge paper (ANROWS Landscapes, 12/2015). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/02/12_1.2-Landscapes-ASPIRE-web.pdf
Walsh, W. A., Banyard, V. L., Moynihan, M. M., Ward, S., & Cohn, E. S. (2010). Disclosure and service use on a college campus after an unwanted sexual experience. Journal of Trauma & Dissociation, 11(2), 134–151. https://doi.org/10.1080/15299730903502912
Webster, K., Diemer, K., Honey, N., Mannix, S., Mickle, J., Morgan, J. … Ward, A. (2018). Australians’ attitudes to violence against women and gender equality: Findings from the 2017 National Community Attitudes towards Violence against Women Survey (NCAS) (Research Report, 03/2018). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/12/anr001-NCAS-report-WEB-1019.pdf
Webster, K., Vaughan, C., Yasmin, R., Diemer, K., Honey, N., Mickle, J. … Ward, A. (2019). Attitudes towards violence against women and gender equality among people from non English speaking countries: Findings from the 2017 National Community Attitudes towards Violence against Women Survey (NCAS) (ANROWS Insights, 02/2019). ANROWS. https://20ian81kynqg38bl3l3eh8bf-wpengine.netdna-ssl.com/wp-content/uploads/2019/12/2017NCAS_NMESC_Report.1.pdf
World Health Organization. (2021). Violence against women prevalence estimates, 2018: Global, regional and national prevalence estimates for intimate partner violence against women and global and regional prevalence estimates for non-partner sexual violence against women. https://www.who.int/publications/i/item/9789240022256
Zark, L., Toumbourou, J. W., & Satyen, L. (in press). Intimate partner and family violence among women tertiary students in Australia: Prevalence and cross-cultural differences. Violence Against Women.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. Laura Zark is supported by the Lina Ricciardelli Memorial Scholarship from the School of Psychology at Deakin University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zark, L., Toumbourou, J.W. & Satyen, L. Help-Seeking for Intimate Partner and Family Violence Among Tertiary Students in Australia: Nature, Extent, and Cross-Cultural Differences. J Fam Viol 38, 491–508 (2023). https://doi.org/10.1007/s10896-022-00406-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10896-022-00406-5