
Abstract
Background
Patients with ventricular tachycardia (VT) who require VT ablation are at high risk for readmission. This study aimed to identify the causes and outcomes of 30-day readmission after VT ablation and to analyze the predictors of recurrent VT that required rehospitalization.
Methods
Using the Nationwide Readmission Database, our study included patients aged ≥ 18 years who underwent VT catheter ablation between 2017 and 2020. Based on the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM), we identified the causes of 30-day readmission by organ systems and analyzed their outcomes. Additional analysis was performed to determine the independent predictors of 30-day readmission for recurrent VT.
Results
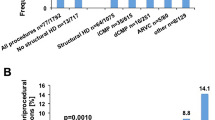
Of the 4228 patients who underwent VT ablation, 14.2% were readmitted within 30 days of the procedure. The most common cause of readmission was cardiac events (73.6%). Among the cardiac-related readmissions, recurrent VT (47.7%) and congestive heart failure (CHF) (12.9%) were the most common etiologies. Among the readmissions, patients readmitted for CHF had the highest rate of readmission mortality (9.2%). Of the patients readmitted within 30 days of the procedure, 278 patients (6.8%) were readmitted for recurrent VT. Via multivariable analysis, CHF (OR: 1.97; 95% CI: 1.12–3.47; P = 0.02) and non-elective index admissions (OR: 1.63; 95% CI: 1.04–2.55; P = 0.03) were identified as the independent predictors predictive of 30-day readmissions for recurrent VT.
Conclusions
Recurrent VT was the most common cause of readmission after the VT ablation procedure, and CHF and non-elective index admissions were the significant predictors of these early readmissions. Readmission due to CHF had the highest mortality rate during readmission.



Similar content being viewed by others


Data Availability
We confirm that the data supporting the findings of this study are available within the article.
Abbreviations
- AHRQ:
-
Agency for Healthcare Research and Quality
- CHF:
-
Congestive heart failure
- HCUP:
-
Healthcare Cost and Utilization Project
- ICD-10-CM:
-
International Classification of Diseases, Tenth Revision, Clinical Modification
- IQR:
-
Interquartile range
- NRD:
-
Nationwide Readmission Database
- OR:
-
Odds ratio
- VT:
-
Ventricular tachycardia
References
Al-Khatib SM, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2018;72(14):1677–749.
Sapp JL, et al. Ventricular tachycardia ablation versus escalation of antiarrhythmic drugs. N Engl J Med. 2016;375(2):111–21.
Tung R, et al. First-line catheter ablation of monomorphic ventricular tachycardia in cardiomyopathy concurrent with defibrillator implantation: the PAUSE-SCD randomized trial. Circulation. 2022;145(25):1839–49.
Cheung JW, et al. Outcomes, costs, and 30-day readmissions after catheter ablation of myocardial infarct-associated ventricular tachycardia in the real world: Nationwide Readmissions Database 2010 to 2015. Circ Arrhythm Electrophysiol. 2018;11(11):e006754.
Briceno DF, et al. Catheter ablation of ventricular tachycardia in nonischemic cardiomyopathy: a propensity score-matched analysis of in-hospital outcomes in the United States. J Cardiovasc Electrophysiol. 2018;29(5):771–9.
(2018) Introduction to the NRD. Healthcare Cost and Utilization Project (HCUP) April 2021. Available from: www.hcup-us.ahrq.gov/db/nation/nrd/Introduction_NRD_2010-2018.jsp.
(2019) Introduction to the NRD. Healthcare Cost and Utilization Project (HCUP). October 2021. Available from: www.hcup-us.ahrq.gov/db/nation/nrd/Introduction_NRD_2019.jsp.
(2020) Introduction to the NRD. Healthcare Cost and Utilization Project (HCUP). November 2022. Available from: www.hcup-us.ahrq.gov/db/nation/nrd/Introduction_NRD_2020.jsp.
Tung R, et al. Freedom from recurrent ventricular tachycardia after catheter ablation is associated with improved survival in patients with structural heart disease: an International VT Ablation Center Collaborative Group study. Heart Rhythm. 2015;12(9):1997–2007.
Nazarian S, et al. Magnetic resonance assessment of the substrate for inducible ventricular tachycardia in nonischemic cardiomyopathy. Circulation. 2005;112(18):2821–5.
Santangeli P, et al. Management of ventricular arrhythmias in patients with advanced heart failure. J Am Coll Cardiol. 2017;69(14):1842–60.
Yokokawa M, et al. The characteristics and distribution of the scar tissue predict ventricular tachycardia in patients with advanced heart failure. Pacing Clin Electrophysiol. 2009;32(3):314–22.
Becher RD, et al. A critical assessment of outcomes in emergency versus nonemergency general surgery using the American College of Surgeons National Surgical Quality Improvement Program database. Am Surg. 2011;77(7):951–9.
Willems S, et al. Preventive or deferred ablation of ventricular tachycardia in patients with ischemic cardiomyopathy and implantable defibrillator (BERLIN VT): a multicenter randomized trial. Circulation. 2020;141(13):1057–67.
Lee JZ, et al. Causes of early mortality after ventricular tachycardia ablation in patients with reduced ejection fraction. JACC Clin Electrophysiol. 2022
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
Not applicable.
Informed consent
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Tan, M.C., Ang, Q.X., Yeo, Y.H. et al. Thirty-day readmission after catheter ablation for ventricular tachycardia: associated factors and outcomes. J Interv Card Electrophysiol 67, 513–521 (2024). https://doi.org/10.1007/s10840-023-01614-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-023-01614-9