
Abstract
Background
Pulmonary vein (PV) isolation (PVI) has become the cornerstone of atrial fibrillation (AF) ablation in patients with paroxysmal AF (PAF). PVI durability is influenced by many factors including PVs anatomy. Data regarding the influence of PVs anatomical variations on the outcomes of PAF ablation in the era of contact force-sensing ablation catheters are scarce and contradictory.
Methods
Consecutive patients referred to our center for a first ablation of PAF using radiofrequency (RF) were included. PVs anatomy was classified into 3 groups: typical anatomy (4 distinct veins), left common ostium (LCO), and right accessory PV (RAPV). The primary outcome was recurrence of atrial arrhythmia episode during a 12-month follow-up after ablation.
Results
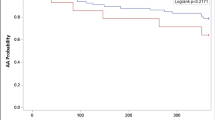
Two hundred twenty-three patients were included (mean age 58.4 ± 10.8 years and 70.9% male). Among this cohort, 141 patients (63.2%) had typical PV anatomy, 53 (23.8%) had a LCO, and 29 (13.0%) had a RAPV. The existence of a RAPV was not associated with a higher rate of AF recurrences (22 (14.3%) vs. 7 (10.1%), p = 0.519). After multivariate analysis, the presence of an LCO did not appear to be associated with the AF recurrence rate at 12 months (OR = 1.69, 95%CI 0.95–2.49, p = 0.098). Maintenance of antiarrhythmic drugs after ablation was the only factor independently associated with a decreased risk of AF recurrence at 12 months (OR = 0.76, 95%CI 0.60–0.97, p = 0.046).
Conclusion
This study suggests that the presence of an LCO or a RAPV is not associated with a higher rate of AF recurrence at 12 months after radiofrequency PVI using contact force-sensing catheters in PAF patients.




Similar content being viewed by others


Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- AAD:
-
Antiarrhythmic drugs
- AF:
-
Atrial fibrillation
- PAF:
-
Paroxysmal atrial fibrillation
- PV:
-
Pulmonary vein
- PVI:
-
Pulmonary vein isolation
- LA:
-
Left atrium
- LVEF:
-
Left ventricular ejection fraction
- CT:
-
Computed tomography
- LCO:
-
Left common ostium
- RAPV:
-
Right accessory pulmonary vein
- RF:
-
Radiofrequency
References
Kornej J, Börschel CS, Benjamin EJ, Schnabel RB. Epidemiology of atrial fibrillation in the 21st century: novel methods and new insights. Circ Res. 2020;127:4–20. https://doi.org/10.1161/CIRCRESAHA.120.316340.
Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2021;42:373–498. https://doi.org/10.1093/eurheartj/ehaa612.
January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC, et al. AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation. 2019;2019:140. https://doi.org/10.1161/CIR.0000000000000665.
Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339:659–66. https://doi.org/10.1056/NEJM199809033391003.
Verma A, Kilicaslan F, Pisano E, Marrouche NF, Fanelli R, Brachmann J, et al. Response of atrial fibrillation to pulmonary vein antrum isolation is directly related to resumption and delay of pulmonary vein conduction. Circulation. 2005;112:627–35. https://doi.org/10.1161/CIRCULATIONAHA.104.533190.
McLellan AJA, Ling L, Ruggiero D, Wong MCG, Walters TE, Nisbet A, et al. Pulmonary vein isolation: the impact of pulmonary venous anatomy on long-term outcome of catheter ablation for paroxysmal atrial fibrillation. Heart Rhythm. 2014;11:549–56. https://doi.org/10.1016/j.hrthm.2013.12.025.
Larsen JM, Deyell MW, Macle L, Champagne J, Sarrazin J, Leong-Sit P, et al. Impact of left common pulmonary veins in the contact force versus cryoballoon atrial fibrillation ablation (CIRCA-DOSE) study. J Cardiovasc Electrophysiol. 2020;31:2300–7. https://doi.org/10.1111/jce.14652.
Pichard C, Nicolas A, Galand V, Coquard C, Behar N, Chérel C, et al. Cryoballoon ablation of atrial fibrillation in patients with atypical right pulmonary vein anatomy. Arch Cardiovasc Dis. 2020;113:690–700. https://doi.org/10.1016/j.acvd.2020.05.008.
Benali K, Da Costa A, Macle L, Hammache N, Galand V, Romeyer C, et al. Distance between the descending aorta and the left inferior pulmonary vein as a determinant of biophysical parameters during paroxysmal atrial fibrillation cryoablation. J Cardiovasc Electrophysiol. 2021;32:2943–52. https://doi.org/10.1111/jce.15234.
Ronsoni RM, Silvestrini TL, Essebag V, Lopes RD, Lumertz Saffi MA, Luz Leiria TL. Association of the left common ostium with clinical outcome after pulmonary vein isolation in atrial fibrillation. Indian Pacing Electrophysiol J. 2021;21:95–100. https://doi.org/10.1016/j.ipej.2020.11.020.
Sohns C, Sohns JM, Bergau L, Sossalla S, Vollmann D, Luthje L, et al. Pulmonary vein anatomy predicts freedom from atrial fibrillation using remote magnetic navigation for circumferential pulmonary vein ablation. Europace. 2013;15:1136–42. https://doi.org/10.1093/europace/eut059.
den Uijl DW, Tops LF, Delgado V, Schuijf JD, Kroft LJM, de Roos A, et al. Effect of Pulmonary vein anatomy and left atrial dimensions on outcome of circumferential radiofrequency catheter ablation for atrial fibrillation. Am J Cardiol. 2011;107:243–9. https://doi.org/10.1016/j.amjcard.2010.08.069.
Neuzil P, Reddy VY, Kautzner J, Petru J, Wichterle D, Shah D, et al. Electrical reconnection after pulmonary vein isolation is contingent on contact force during initial treatment: results from the EFFICAS I Study. Circ Arrhythm Electrophysiol. 2013;6:327–33. https://doi.org/10.1161/CIRCEP.113.000374.
Kuck K-H, Reddy VY, Schmidt B, Natale A, Neuzil P, Saoudi N, et al. A novel radiofrequency ablation catheter using contact force sensing: Toccata study. Heart Rhythm. 2012;9:18–23. https://doi.org/10.1016/j.hrthm.2011.08.021.
Kimura M, Sasaki S, Owada S, Horiuchi D, Sasaki K, Itoh T, et al. Comparison of lesion formation between contact force-guided and non-guided circumferential pulmonary vein isolation: a prospective, randomized study. Heart Rhythm. 2014;11:984–91. https://doi.org/10.1016/j.hrthm.2014.03.019.
Marom EM, Herndon JE, Kim YH, McAdams HP. Variations in pulmonary venous drainage to the left atrium: implications for radiofrequency ablation. Radiology. 2004;230:824–9. https://doi.org/10.1148/radiol.2303030315.
Perino AC, Leef GC, Cluckey A, Yunus FN, Askari M, Heidenreich PA, et al. Secular trends in success rate of catheter ablation for atrial fibrillation: the SMASH-AF cohort. Am Heart J. 2019;208:110–9. https://doi.org/10.1016/j.ahj.2018.10.006.
Mlcochova H, Tintera J, Porod V, Peichl P, Cihak R, Kautzner J. Magnetic resonance angiography of pulmonary veins: implications for catheter ablation of atrial fibrillation. Pacing Clin Electrophysiol. 2005;28:1073–80. https://doi.org/10.1111/j.1540-8159.2005.00228.x.
Kaseno K, Tada H, Koyama K, Jingu M, Hiramatsu S, Yokokawa M, et al. Prevalence and characterization of pulmonary vein variants in patients with atrial fibrillation determined using 3-dimensional computed tomography. Am J Cardiol. 2008;101:1638–42. https://doi.org/10.1016/j.amjcard.2008.01.053.
Wittkampf FHM, Vonken E-J, Derksen R, Loh P, Velthuis B, Wever EFD, et al. Pulmonary vein ostium geometry: analysis by magnetic resonance angiography. Circulation. 2003;107:21–3. https://doi.org/10.1161/01.CIR.0000047065.49852.8F.
Kato R, Lickfett L, Meininger G, Dickfeld T, Wu R, Juang G, et al. Pulmonary vein anatomy in patients undergoing catheter ablation of atrial fibrillation: lessons learned by use of magnetic resonance imaging. Circulation. 2003;107:2004–10. https://doi.org/10.1161/01.CIR.0000061951.81767.4E.
Stanford W, Breen JF. CT evaluation of left atrial pulmonary venous anatomy. Int J Cardiovasc Imaging. 2005;21:133–9. https://doi.org/10.1007/s10554-004-5347-5.
Beiert T, Lodde PC, Linneborn LPT, Werner J, Prinz L, Stöckigt F, et al. Outcome in patients with left common pulmonary vein after cryoablation with second-generation cryoballoon. Pacing Clin Electrophysiol. 2018;41:22–7. https://doi.org/10.1111/pace.13247.
Kubala M, Hermida J-S, Nadji G, Quenum S, Traulle S, Jarry G. Normal pulmonary veins anatomy is associated with better AF-free survival after cryoablation as compared to atypical anatomy with common left pulmonary vein: COMMON LEFT PULMONARY VEIN. Pacing Clin Electrophysiol. 2011;34:837–43. https://doi.org/10.1111/j.1540-8159.2011.03070.x.
Mulder AAW, Wijffels MCEF, Wever EFD, Boersma LVA. Pulmonary vein anatomy and long-term outcome after multi-electrode pulmonary vein isolation with phased radiofrequency energy for paroxysmal atrial fibrillation. Europace. 2011;13:1557–61. https://doi.org/10.1093/europace/eur236.
Hof I, Chilukuri K, Arbab-Zadeh A, Scherr D, Dalal D, Nazarian S, et al. Does left atrial volume and pulmonary venous anatomy predict the outcome of catheter ablation of atrial fibrillation? J Cardiovasc Electrophysiol. 2009;20:1005–10. https://doi.org/10.1111/j.1540-8167.2009.01504.x.
Woźniak-Skowerska I, Skowerski M, Wnuk-Wojnar A, Hoffmann A, Nowak S, Gola A, et al. Comparison of pulmonary veins anatomy in patients with and without atrial fibrillation: analysis by multislice tomography. Int J Cardiol. 2011;146:181–5. https://doi.org/10.1016/j.ijcard.2009.06.047.
Lin W-S, Prakash VS, Tai C-T, Hsieh M-H, Tsai C-F, Yu W-C, et al. Pulmonary vein morphology in patients with paroxysmal atrial fibrillation initiated by ectopic beats originating from the pulmonary veins: implications for catheter ablation. Circulation. 2000;101:1274–81. https://doi.org/10.1161/01.CIR.101.11.1274.
Tsao H-M, Yu W-C, Cheng H-C, Wu M-H, Tai C-T, Lin W-S, et al. Pulmonary vein dilation in patients with atrial fibrillation: detection by magnetic resonance imaging. J Cardiovasc Electrophysiol. 2001;12:809–13. https://doi.org/10.1046/j.1540-8167.2001.00809.x.
Schwartzman D, Bazaz R, Nosbisch J. Common left pulmonary vein: a consistent source of arrhythmogenic atrial ectopy. J Cardiovasc Electrophysiol. 2004;15:560–6. https://doi.org/10.1046/j.1540-8167.2004.03351.x.
Bittner A, Monnig G, Vagt AJ, Zellerhoff S, Wasmer K, Kobe J, et al. Pulmonary vein variants predispose to atrial fibrillation: a case-control study using multislice contrast-enhanced computed tomography. Europace. 2011;13:1394–400. https://doi.org/10.1093/europace/eur145.
Satoh T, Zipes DP. Unequal atrial stretch in dogs increases dispersion of refractoriness conducive to developing atrial fibrillation. J Cardiovasc Electrophysiol. 1996;7:833–42. https://doi.org/10.1111/j.1540-8167.1996.tb00596.x.
Xu B, Xing Y, Xu C, Peng F, Sun Y, Wang S, et al. A left common pulmonary vein: anatomical variant predicting good outcomes of repeat catheter ablation for atrial fibrillation. J Cardiovasc Electrophysiol. 2019;30:717–26. https://doi.org/10.1111/jce.13876.
Aursulesei S, Cismaru G, Rosu R, Puiu M, Gusetu G, Zdrenghea D, Pop D. P995 The effect of pulmonary vein anatomy on outcome of catheter ablation for atrial fibrillation. Eur Heart J. 2018;39(suppl_1):ehy564.P995. https://doi.org/10.1093/eurheartj/ehy564.P995.
Khoueiry Z, Albenque J-P, Providencia R, Combes S, Combes N, Jourda F, et al. Outcomes after cryoablation vs. radiofrequency in patients with paroxysmal atrial fibrillation: impact of pulmonary veins anatomy. Europace. 2016;18:1343–51. https://doi.org/10.1093/europace/euv419.
Istratoaie S, Roşu R, Cismaru G, VesaŞtefan C, Puiu M, Zdrenghea D, et al. The impact of pulmonary vein anatomy on the outcomes of catheter ablation for atrial fibrillation. Medicina (Mex). 2019;55:727. https://doi.org/10.3390/medicina55110727.
Haïssaguerre M, Wright M, Hocini M, Jaïs P. The substrate maintaining persistent atrial fibrillation. Circ Arrhythm Electrophysiol. 2008;1:2–5. https://doi.org/10.1161/CIRCEP.108.764233.
Hunter RJ, Ginks M, Ang R, Diab I, Goromonzi FC, Page S, et al. Impact of variant pulmonary vein anatomy and image integration on long-term outcome after catheter ablation for atrial fibrillation. Europace. 2010;12:1691–7. https://doi.org/10.1093/europace/euq322.
Gerstenfeld EP. Contact force–sensing catheters: evolution or revolution in catheter ablation technology? Circ Arrhythm Electrophysiol. 2014;7:5–6. https://doi.org/10.1161/CIRCEP.114.001424.
Natale A, Reddy VY, Monir G, Wilber DJ, Lindsay BD, McElderry HT, et al. Paroxysmal AF catheter ablation with a contact force sensing catheter. J Am Coll Cardiol. 2014;64:647–56. https://doi.org/10.1016/j.jacc.2014.04.072.
Acknowledgements
We would like to thank Arthur Kohler and Maxime Tissier for their contribution to this work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
This study was approved by institutional ethics committee and all patients provided informed consent.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Benali, K., Lai, V.D., Hammache, N. et al. Impact of pulmonary veins anatomy on the outcomes of radiofrequency ablation for paroxysmal atrial fibrillation in the era of contact force-sensing ablation catheters. J Interv Card Electrophysiol 66, 931–940 (2023). https://doi.org/10.1007/s10840-022-01393-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-022-01393-9