
Abstract
Background
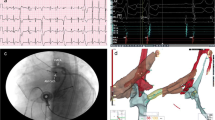
Intraprocedural coronary angiography (CA) is recommended in patients undergoing ablation in aortic cusps to assess the relation of catheter tip and coronary ostia. In this report, we aimed to compare selective coronary angiography (SCA) through the contact force (CF)-sensing radiofrequency catheter with conventional coronary angiography (CCA) to guide ablation of premature ventricular contractions (PVC).
Methods
This was a retrospective observational cohort study of prospectively collected data of 87 consecutive patients undergoing PVC ablation at a single institution between February 2016 and June 2021. Forty-six patients (53%) underwent SCA and forty-one patients (47%) underwent CCA. Data were consecutively collected case-by-case and entered into a computerized database. Procedural characteristics, complications, and clinical outcomes were compared between the SCA and CCA groups.
Results
Successful ablation was achieved in seventy-seven (89%) patients. Total procedure and fluoroscopy time and radiation dose were significantly lower in SCA group (93 ± 22 min vs 102 ± 20 min, p = 0.042; 12 ± 3 min vs 14 ± 4 min, p = 0.030; 3292 ± 1221 μGy m2 vs 3880 ± 1229 μGy m2, p = 0.028, respectively). Median ambulation time was significantly longer in CCA group (6.8 ± 1 h vs 17.8 ± 1.8 h, p = 0.006).
Conclusions
Selective coronary angiography through the CF-sensing ablation catheter to assess the relation between the ablation site and the coronary ostia is feasible and safe. This technique precludes the requirement of an additional arterial access and decreases the total procedure and fluoroscopy time and radiation dose.

Similar content being viewed by others


References
Anderson RD, Kumar S, Parameswaran R, Wong G, Voskoboinik A, Sugumar H, et al. Differentiating right- and left-sided outflow tract ventricular arrhythmias: classical ECG signatures and prediction algorithms. Circ Arrhythm Electrophysiol. 2019;12(6):e007392.
Kodali S, Santangeli P, Garcia FC. Mapping and ablation of arrhythmias from uncommon sites (aortic cusp, pulmonary artery, and left ventricular summit). Card Electrophysiol Clin. 2019;11(4):665–74.
Yamada T. Twelve-lead electrocardiographic localization of idiopathic premature ventricular contraction origins. J Cardiovasc Electrophysiol. 2019;30(11):2603–17.
Chun KR, Satomi K, Kuck KH, Ouyang F, Antz M. Left ventricular outflow tract tachycardia including ventricular tachycardia from the aortic cusps and epicardial ventricular tachycardia. Herz. 2007;32(3):226–32.
Daniels DV, Lu YY, Morton JB, Santucci PA, Akar JG, Green A, et al. Idiopathic epicardial left ventricular tachycardia originating remote from the sinus of Valsalva: electrophysiological characteristics, catheter ablation, and identification from the 12-lead electrocardiogram. Circulation. 2006;113(13):1659–66.
Gorenek B, Fisher JD, Kudaiberdieva G, Baranchuk A, Burri H, Campbell KB, et al. Premature ventricular complexes: diagnostic and therapeutic considerations in clinical practice: A state-of-the-art review by the American College of Cardiology Electrophysiology Council. J Interv Card Electrophysiol. 2020;57(1):5–26.
Zou S, Jia R, Zhou X, Hao Y, Lu S, Guo R, et al. Merging three-dimensional CT with electroanatomic mapping facilitates ablation of ventricular arrhythmias originating from aortic root and great cardiac vein. J Interv Card Electrophysiol. 2021;60(1):101–8.
Jularic M, Akbulak RÖ, Schäffer B, Moser J, Nuehrich J, Meyer C, et al. Image integration into 3-dimensional-electro-anatomical mapping system facilitates safe ablation of ventricular arrhythmias originating from the aortic root and its vicinity. Europace. 2018;20(3):520–7.
Roca-Luque I, Rivas N, Francisco J, Perez J, Acosta G, Oristrell G, et al. Selective angiography using the radiofrequency catheter: an alternative technique for mapping and ablation in the aortic cusps. J Cardiovasc Electrophysiol. 2017;28(1):126–31.
Celikyurt U, Acar B, Karauzum I, Hanci K, Vural A, Agacdiken A. Selective angiography through radiofrequency catheter during ablation of premature ventricular contractions originating from aortic cusp: a single-centre experience. Indian Pacing Electrophysiol J. 2022;22(4):195–9.
Ishikawa E, Miyazaki S, Mukai M, Aoyama D, Nodera M, Hasegawa K, et al. Femoral vascular complications after catheter ablation in the current era: the utility of computed tomography imaging. J Cardiovasc Electrophysiol. 2020;31(6):1385–93.
Castillo-Sang M, Tsang AW, Almaroof B, Cireddu J, Sferra J, Zelenock GB, et al. Femoral artery complications after cardiac catheterization: a study of patient profile. Ann Vasc Surg. 2010;24(3):328–35.
Alonso M, Tascón J, Hernández F, Andreu J, Albarrán A, Velázquez MT. Complications with femoral access in cardiac cathetization. Impact of previous systematic femoral angiography and hemostasis with VasoSeal-ES collagen plug. Rev Esp Cardiol. 2003;56(6):569–77.
Zeb I, Abbas N, Nasir K, Budoff MJ. Coronary computed tomography as a cost-effective test strategy for coronary artery disease assessment - a systematic review. Atherosclerosis. 2014;234(2):426–35.
Kosiuk J, Fiedler L, Ernst S, Duncker D, Pavlović N, Guarguagli S, et al. Fluoroscopy usage in contemporary interventional electrophysiology: insights from a European registry. Clin Cardiol. 2021;44(1):36–42.
Heidbuchel H, Wittkampf FH, Vano E, Ernst S, Schilling R, Picano E, et al. Practical ways to reduce radiation dose for patients and staff during device implantations and electrophysiological procedures. Europace. 2014;16(7):946–64.
Yu HT, Shin DG, Shim J, Nam GB, Yoo WW, Lee JH, et al. Unilateral versus bilateral groin puncture for atrial fibrillation ablation: multi-center prospective randomized study. Yonsei Med J. 2019;60(4):360–7.
Hoffmayer KS, Dewland TA, Hsia HH, Badhwar N, Hsu JC, Tseng ZH, et al. Safety of radiofrequency catheter ablation without coronary angiography in aortic cusp ventricular arrhythmias. Heart Rhythm. 2014;11(7):1117–21.
Turchetti G, Kroes MA, Lorenzoni V, Trieste L, Chapman AM, Sweet AC, et al. The cost-effectiveness of diagnostic cardiac imaging for stable coronary artery disease. Expert Rev Pharmacoecon Outcomes Res. 2015;15(4):625–33.
Acknowledgements
The authors wish to thank Adem Koc (Biosense Webster, Istanbul, Turkey) for technical support during catheter ablation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
The study was approved by the Local Ethical Committee of the university hospital (2022/210).
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Celikyurt, U., Acar, B., Agacdiken, A. et al. Comparison of selective coronary angiography through the ablation catheter versus conventional coronary angiography to guide ablation of premature ventricular contractions originating from aortic cusp. J Interv Card Electrophysiol 65, 711–715 (2022). https://doi.org/10.1007/s10840-022-01324-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-022-01324-8