
Abstract
Background
An acute cryothermal ablation lesion contains both reversible and irreversible elements. However, differences in lesions created with cryoballoon pulmonary vein isolation (PVI) between the acute and chronic phases have not been fully elucidated.
Methods
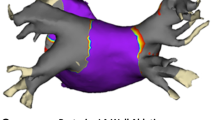
We retrospectively analyzed 23 consecutive patients with atrial fibrillation who underwent cryoballoon PVI during the initial procedure followed by a second ablation procedure. In all patients, cryoballoon PVI lesions were evaluated with high-resolution voltage mapping just after PVI (acute phase) and during the second session (chronic phase). We compared the area and width of the non-isolated left atrial posterior wall (NI-LAPW) with voltage ≥ 0.5 mV during both sessions.
Results
PVI was successfully achieved in all patients. Cryoballoon PVI lesions were re-evaluated at 11 [2–17] months post-procedure. During the chronic phase, NI-LAPW width became significantly larger at the level of the roof (change, 5.8 ± 5.5 mm; p < 0.001) and at the level of the carina (change, 3.3 ± 7.0 mm; p < 0.05), and NI-LAPW area became significantly larger (change, 1.5 ± 1.9 cm2; p < 0.001) compared with the acute phase. Eight patients without any PV reconnections also had larger NI-LAPW areas (change, 1.3 ± 1.2 cm2; p < 0.05) during the chronic phase. Conduction resumption confined to the right carina was observed in 1 (4.3%) patient who presented with circumferential PVI that included the carina during the first session.
Conclusion
Acute cryoballoon PVI lesions significantly regressed during the chronic phase. PV reconnections and the isolation area should be carefully re-evaluated during the second procedure.





Similar content being viewed by others


Availability of data and material
Upon reasonable request.
References
Nogami A, Kurita T, Abe H, et al. JCS/JHRS 2019 guideline on non-pharmacotherapy of cardiac arrhythmias. J Arrhythm. 2021;37(4):709–870.
Wazni OM, Dandamudi G, Sood N, et al. Cryoballoon ablation as initial therapy for atrial fibrillation. N Engl J Med. 2021;384(4):316–24.
Providencia R, Defaye P, Lambiase PD, et al. Results from a multicentre comparison of cryoballoon vs. radiofrequency ablation for paroxysmal atrial fibrillation: is cryoablation more reproducible? Europace. 2017;19(1):48–57
Avitall B, Kalinski A. Cryotherapy of cardiac arrhythmia: from basic science to the bedside. Heart Rhythm. 2015;12(10):2195–203.
Chaumont C, Mirolo A, Savouré A, et al. Very long-term outcomes after catheter ablation of atrioventricular nodal reentrant tachycardia: how does cryoenergy differ from radiofrequency? J Cardiovasc Electrophysiol. 2020;31(12):3215–22.
Bravo L, Atienza F, Eidelman G, et al. Safety and efficacy of cryoablation vs. radiofrequency ablation of septal accessory pathways: systematic review of the literature and meta-analyses. Europace. 2018;20(8):1334–1342
Mukai M, Miyazaki S, Hasegawa K, et al. Cryothermal atrial linear ablation in patients with atrial fibrillation: an insight from the comparison with radiofrequency atrial linear ablation. J Cardiovasc Electrophysiol. 2020;31(5):1075–82.
Sørensen SK, Johannessen A, Worck R, Hansen ML, Hansen J. Radiofrequency versus cryoballoon catheter ablation for paroxysmal atrial fibrillation: durability of pulmonary vein isolation and effect on atrial fibrillation burden: the RACE-AF Randomized Controlled Trial. Circ Arrhythm Electrophysiol 2021;14(5):e009573.
Wang Y, Wang W, Yao J, Chen L, Yi S. Second-generation cryoballoon vs. contact-force sensing radiofrequency catheter ablation in atrial fibrillation: a meta-analysis of randomized controlled trials. J Interv Card Electrophysiol 2021;60(1):9–19.
Miyazaki S, Hachiya H, Nakamura H, et al. Pulmonary vein isolation using a second-generation cryoballoon in patients with paroxysmal atrial fibrillation: one-year outcome using a single big-balloon 3-minute freeze technique. J Cardiovasc Electrophysiol. 2016;27(12):1375–80.
Chierchia GB, Di Giovanni G, Sieira-Moret J, et al. Initial experience of three-minute freeze cycles using the second-generation cryoballoon ablation: acute and short-term procedural outcomes. J Interv Card Electrophysiol. 2014;39(2):145–51.
Su W, Kowal R, Kowalski M, et al. Best practice guide for cryoballoon ablation in atrial fibrillation: the compilation experience of more than 3000 procedures. Heart Rhythm. 2015;12(7):1658–66.
Miyazaki S, Taniguchi H, Hachiya H, et al. Quantitative analysis of the isolation area during the chronic phase after a 28-mm second-generation cryoballoon ablation demarcated by high-resolution electroanatomic mapping. Circ Arrhythm Electrophysiol. 2016;9(5):e003879.
Kawamura I, Neuzil P, Shivamurthy P, et al. How does the level of pulmonary venous isolation compare between pulsed field ablation and thermal energy ablation (radiofrequency, cryo, or laser)? EP Europace. 2021.
Inamura Y, Nitta J, Inaba O, et al. Differences in the electrophysiological findings of repeat ablation between patients who first underwent cryoballoon ablation and radiofrequency catheter ablation for paroxysmal atrial fibrillation. J Cardiovasc Electrophysiol. 2019;30(10):1792–800.
Kuck K-H, Albenque J-P, Chun KRJ, et al. Repeat ablation for atrial fibrillation recurrence post cryoballoon or radiofrequency ablation in the FIRE AND ICE Trial. Circ Arrhythm Electrophysiol 2019;12(6):e007247.
Kenigsberg DN, Martin N, Lim HW, Kowalski M, Ellenbogen KA. Quantification of the cryoablation zone demarcated by pre- and postprocedural electroanatomic mapping in patients with atrial fibrillation using the 28-mm second-generation cryoballoon. Heart Rhythm. 2015;12(2):283–90.
Chikata A, Kato T, Usuda K, et al. Impact of left atrial size on isolation area in the acute phase of pulmonary vein isolation using 28 mm cryoballoon. Pacing Clin Electrophysiol. 2018;41(7):700–6.
Nanbu T, Yotsukura A, Sano F, et al. A relation between ablation area and outcome of ablation using 28-mm cryoballon ablation: importance of carina region. J Cardiovasc Electrophysiol. 2018;29(9):1221–9.
Aryana A, Di Biase L, Pujara DK, et al. Long-term durability of posterior wall isolation using the cryoballoon in patients with persistent atrial fibrillation: a multicenter analysis of repeat catheter ablations. J Intervl Card Electrophysiol. 2021;62(1):161–9.
Miyazaki S, O’Connell H, Maus B. Parameters associated with acute morphometric lesion dimensions created by cryocatheters. J Interv Card Electrophysiol. 2019;54(2):109–18.
Acknowledgements
We greatly appreciate our hospital’s clinical engineers.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
The study protocol was approved by the hospital’s institutional review board (approval number 20180040). The study complied with the Declaration of Helsinki.
Conflict of interest
Dr. Miyazaki belonged to a department endowed by Medtronic, Boston, Abbott, and Japan Lifeline.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Sekihara, T., Miyazaki, S., Aoyama, D. et al. Evaluation of cryoballoon pulmonary vein isolation lesions during the acute and chronic phases using a high-resolution mapping system. J Interv Card Electrophysiol 65, 123–131 (2022). https://doi.org/10.1007/s10840-022-01225-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-022-01225-w