
Abstract
Purpose
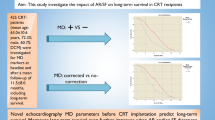
Response to cardiac resynchronization therapy (CRT) in patients with heart failure with reduced ejection fraction (HFrEF) depends on the degree of correction of interventricular (VV) electromechanical dyssynchrony between the left and right ventricles (LV, RV). Wide (> 130 ms [ms]) QRS interval is used as a qualifying ECG parameter for CRT device implantation. In this study, we aimed to evaluate myocardial strain (S) and myocardial strain patterns (SP) and strain rate (SR) by speckle tracking echocardiography (STE) and mechanical characteristics at different VV intervals in acute settings and long-term outcome from “sequential LV-RV” pacing programming in patients with narrow (< 130 ms) and wide (> 130 ms) QRS complexes as a basis for extending CRT in select patients with narrow QRS.
Methods
From a previously established cohort of patients who had undergone CRT device implantation, we identified patients with narrow (< 130 ms) and wide (> 130 ms) QRS complexes, groups A and B respectively. In all patients, we assessed myocardial SP and SR by STE, and mechanical characteristics at VV intervals: “LV Off,” “VV0,” “VV60,” and “RV Off” to provide “RV-only,” “simultaneous BiV,” “sequential LV-RV,” and “LV-only” pacing in the acute settings, and subsequently long-term clinical outcomes with CRT devices programmed to VV60. We compared acute STE characteristics and long-term clinical outcomes between the groups.
Results
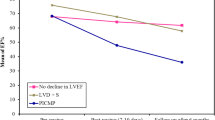
The study cohort comprised 271 patients (age 69.2 ± 10.3 years [mean ± SD], male—60%). Group A (n = 69) and group B (n = 202) were well matched for the clinical variables, including distribution of patients with ischemic versus non-ischemic cardiomyopathies. QRS width and left ventricular ejection fraction (LVEF) in groups A and B were 120.1 ± 12.3 ms and 152.1 ± 12.9 ms (p < 0.05), and 22.3 ± 9.4%, and 23.3 ± 10.2% (p = not significant [NS]). With VV0, VV60, and LV-only timings, corresponding LVEF rates in the acute settings were 31.45 ± 10.9%, 40.08 ± 8.3%, and 44.32 ± 7.98% (p < 0.01) in group A, and 38.94 ± 8.5%, 46.91 ± 7.33%, and 49.9 ± 8.94% (p < 0.01) in group B, and accounted for similar incremental percentage increase in LVEF compared to baseline in group A (43.2 ± 51.7%, 80.9 ± 61.4%, and 93.4 ± 65.6% respectively) and group B (67.3 ± 82.0%, 100.6 ± 94.3%, and 112.9 ± 95.7% respectively) (p = NS). Abnormal SP and SR were consistently observed with RV pacing that improved with VV60 and LV-only pacing in both groups. Strain scores at different VV timings were similar between the groups (p = NS). At 1-year follow-up, LVEF improved from 22.4 ± 8.0% to 39.8 ± 11.5% (p ≤ 0.001) for the total cohort with similar increments observed in both groups (p = NS). There were fewer NYHA III–IV class patients at 1 year in both groups.
Conclusions
Comparable myocardial SP and SR characteristics and LVEF improvement with VV60 and LV-only pacing in the acute setting and long-term outcome of CRT by “sequential LV-RV” pacing seen in patients with both narrow and wide QRS duration suggest that CRT device implantation may be justified in select patients with HFrEF and narrow QRS duration (< 130 ms) who have demonstrable dyssynchrony and abnormal myocardial SP and SR characteristics.



Similar content being viewed by others

Data availability
Our manuscript has no associated data that need deposition in data repository, and data sharing is not applicable to this article.
References
Daubert JC, Saxon L, Adamson PB, Auricchio A, Berger RD, Beshai JF, Breithard O, Brignole M, Cleland J, Delurgio DB, Dickstein K, Exner DV, Gold M, Grimm RA, Hayes DL, Israel C, Leclercq C, Linde C, Lindenfeld J, Merkely B, Mont L, Murgatroyd F, Prinzen F, Saba SF, Shinbane JS, Singh J, Tang AS, Vardas PE, Wilkoff BL, Zamorano JL. 2012 EHRA/HRS expert consensus statement on cardiac resynchronization therapy in heart failure: implant and follow-up recommendations and management. Europace. 2012; 14, 1236–1286. Heart Rhythm. 2012;9(9):1524–76. https://doi.org/10.1016/j.hrthm.2012.07.025.
McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez-Sanchez M, Jaarsma T, Køber L, Lip GYH, Maggioni AP, Parkhomenko A, Pieske BM, Popescu BA, Rønnevik PK, Rutten FH, Schwitter, Seferovic JP, Stepinska J, Trindade PT, Voors AA, Zannad F, Zeiher A, ESC Committee for Practice Guidelines. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33(14):1787–847.
Hsu JC, Solomon SC, Bourgoun M, McNitt S, Goldenberg I, Klein H, Moss AJ, Foster E, MADIT-CRT Executive Committee. Predictors of super-response to cardiac resynchronization therapy and associated improvement in clinical outcome. (The MADIT-CRT study). J Am Coll Cardiol. 2012;59:2366–73.
Tanaka H, Nesser HJ, Buck T, Oyenuga O, Jánosi RA, Winter S, Saba S, Gorcsan J 3rd. Dyssynchrony by speckle-tracking echocardiography and response to cardiac resynchronization therapy: results of the Speckle Tracking and Resynchronization (STAR) study. Eur Heart J. 2010;31:1690–700.
Gorcsan J 3rd, Abraham T, Agler DA, Bax JJ, Derumeaux G, Grimm RA, Martin R, Steinberg JS, Sutton MS, Yu CM; American Society of Echocardiography Dyssynchrony Writing Group. Echocardiography for cardiac resynchronization therapy: recommendations for performance and reporting--a report from the American Society of Echocardiography Dyssynchrony Writing Group endorsed by the Heart Rhythm Society. J Am Soc Echocardiogr. 2008;21(3):191–213. https://doi.org/10.1016/j.echo.2008.01.003.
Singh A, Karnik R, Shah AN, Chutani S, Kantharia BK. Myocardial strain characteristics at different interventricular pacing timings: implication for device programming and long-term clinical outcomes in patients with cardiac resynchronization therapy. Acta Cardiol. 2021;76(1):46–55. https://doi.org/10.1080/00015385.2019.1690261.
Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise JS, Solomon SD, Spencer KT, Sutton MS, Stewart WJ; Chamber Quantification Writing Group; American Society of Echocardiography’s Guidelines and Standards Committee; European Association of Echocardiography. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18(12):1440–63.
Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, Tavazzi L. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539–49.
Oyenuga O, Hara H, Tanaka H, Kim HN, Adelstein EC, Saba S, Gorcsan J 3rd. Usefulness of echocardiographic dyssynchrony in patients with borderline QRS duration to assist with selection for cardiac resynchronization therapy. J Am Coll Cardiol Img. 2010;3:132–40.
Seo Y, Ishizu T, Machino-Ohtsuka T, Yamamoto M, Machino T, Kuroki K, Yamasaki H, Sekiguchi Y, Nogami A, Aonuma K. Incremental value of speckle tracking echocardiography to predict cardiac resynchronization therapy (CRT) responders. J Am Heart Assoc. 2016;5(10): e003882. https://doi.org/10.1161/JAHA.116.003882.
Goldenberg I, Moss AJ, Hall WJ, Foster E, Goldberger JJ, Santucci P, Shinn T, Solomon S, Steinberg JS, Wilber D, Barsheshet A, McNitt S, Zareba W, Klein H. Predictors of response to cardiac resynchronization therapy in the multicenter automatic defibrillator implantation trial with cardiac resynchronization therapy (MADIT-CRT). Circulation. 2011;124:1527–36.
Ruschitzka F, Abraham WT, Singh JP, Bax JJ, Borer JS, Brugada J, Dickstein K, Ford I, Gorcsan J 3rd, Gras D, Krum H, Sogaard P, Holzmeister J; EchoCRT Study Group. Cardiac-resynchronization therapy in heart failure with a narrow QRS complex. N Engl J Med. 2013;369(15):1395–405.
van Bommel RJ, Tanaka H, Delgado V, Bertini M, Borleffs CJ, Ajmone Marsan N, Holzmeister J, Ruschitzka F, Schalij MJ, Bax JJ, Gorcsan J 3rd. Association of intraventricular mechanical dyssynchrony with response to cardiac resynchronization therapy in heart failure patients with a narrow QRS complex. Eur Heart J. 2010;31(24):3054–62.
Tanaka H, Hirata K. Is speckle tracking actually helpful for cardiac resynchronization therapy? J Echocardiogr. 2016;14(2):53–60. https://doi.org/10.1007/s12574-016-0275-7.
Chung ES, Leon AR, Tavazzi L, Sun JP, Nihoyannopoulos P, Merlino J, Abraham WT, Ghio S, Leclercq C, Bax JJ, Yu CM, Gorcsan J 3rd, St John Sutton M, De Sutter J, Murillo J. Results of the Predictors of Response to CRT (PROSPECT) trial. Circulation. 2008;117(20):2608–16. https://doi.org/10.1161/CIRCULATIONAHA.107.743120.
Marwick TH. Hype and hope in the use of echocardiography for selection for cardiac resynchronization therapy: the Tower of Babel revisited. Circulation. 2008;117(20):2573–6. https://doi.org/10.1161/CIRCULATIONAHA.108.772475.
Ramanathan C, Jia P, Ghanem R, Ryu K, Rudy Y. Activation and repolarization of the normal human heart under complete physiological conditions. Proc Nat Acad of Sci. 2006;103:6309–14.
Boriani G, Kranig W, Donal E, Calo L, Castella M, Delarche N, Lozano IF, Ansalone G, Biffi M, Boulogne E, Leclercq C, A randomized double-blind comparison of biventricular versus left ventricular stimulation for cardiac resynchronization therapy: the biventricular versus left univentricular pacing with ICD back-up in heart failure patients ( B-Left HF) trial. Am Heart L. 2010;159:1052-58.e.
Thibault B, Ducharme A, Harel F, White Michel, O’Meara E, Guertin M-C, Lavoie J, Frasure-Smith N, Dubuc M, Guerra P, Macle L, Roy D, Rivard L, Talajic M, Khairy P. Left ventricular versus simultaneous biventricular pacing in patients with heart failure and a QRS complex≥120 milliseconds. Circulation.2011;124:2874–81.
Burns KV, Gage RM, Curtin AE, Gorcsan J 3rd, Bank AJ. Left ventricular-only pacing in heart failure patients with normal atrioventricular conduction improves global function and left ventricular regional mechanics compared with biventricular pacing: an adaptive cardiac resynchronization therapy sub-study. Eur J Heart Fail. 2017;19(10):1335–43. https://doi.org/10.1002/ejhf.906.
Blanc JJ, Bernault-Valls V, Fatemi M, Gilard M, Pennec PY, Etienne Y. Midterm benefits of left univentricular pacing in patients with congestive heart failure. Circulation. 2004;109:1741–4.
Birnie D, Lemke B, Aonuma K, Krum H, Lee KL-F, Gasparini M, Starling RC, Milasinovic G, Gorscan III J, Houmsse M, Abeyratne A, Sambelashvili A, Martin DO. Clinical outcomes with resynchronized left ventricular pacing: analysis of the adaptive CRT trial. Heart Rhythm 2013;10:1368-1374.
Author information
Authors and Affiliations
Contributions
All authors have met with the following authorship criteria: (1) substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published. All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation. BKK and AS conceived and designed the research. BKK, AS, and RK conducted the research, collected, and analyzed data. BN, LW, SC, and ANS analyzed data and contributed to writing the manuscript. BKK and AS wrote the manuscript. All authors read and approved the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Bharat K. Kantharia and Amarnauth Singh contributed equally to this work.
Rights and permissions
About this article

Cite this article
Kantharia, B.K., Singh, A., Narasimhan, B. et al. Cardiac resynchronization therapy in patients with heart failure and narrow QRS complexes (≤ 130 ms): role of speckle tracking echocardiography and different interventricular (VV) pacing intervals. J Interv Card Electrophysiol 63, 369–377 (2022). https://doi.org/10.1007/s10840-021-01021-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-021-01021-y