
Abstract
Purpose
Catheter ablation is less successful for non-paroxysmal atrial fibrillation (NPAF) according to numerous follow-up studies. The choice of ablation strategy for patients with NPAF remains controversial. The objective of the study was to explore the clinical efficacy of the “ICE-FIRE” ablation.
Methods
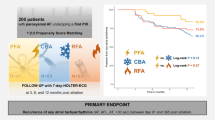
Ninety NPAF patients were enrolled. Patients were randomly divided into RF (treated with circumferential pulmonary vein isolation (CPVI) and additional substrate modification by radiofrequency ablation) group and I-F (treated with CPVI by cryoablation and additional substrate modification by radiofrequency ablation) group. After CPVI and cardioversion to sinus rhythm, high-density mapping was performed. Eight-one of 90 participants restored to sinus rhythm. Seventy-four of 81 NPAF patients showed low-voltage zone. Substrates with low-voltage zone were targeted for further modification. Participants were followed at baseline, 3, 6, 9, and 12 months after the initial ablation.
Results
The I-F group shared more X-ray exposure (I-F, 264.4 ± 97.4 mGy; RF, 224.9 ± 62.0 mGy; P = 0.039) and less duration of the procedure (I-F, 150.3 ± 27.5 min; RF, 174.2 ± 38.5 min; P = 0.003) compared to RF group. The freedom from atrial arrhythmia recurrence at 12 months post-ablation was similar between the RF and I-F groups (RF, 57.1%; I-F, 71.8%; P = 0.197). However, I-F group experienced lower rehospitalization rate of AF recurrence (RF, 42.9%; I-F, 20.5%; P = 0.038).
Conclusions
In NPAF patients requiring substrate mapping and modification, the “ICE-FIRE” ablation demonstrated non-inferior clinical efficacy and lower rehospitalization rate of AF recurrence when compared with pure radiofrequency ablation strategy.



Similar content being viewed by others

References
Benjamin EJ, Wolf PA, D'Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham heart study. Circulation. 1998;98(10):946–52.
Wattigney WA, Mensah GA, Croft JB. Increasing trends in hospitalization for atrial fibrillation in the United States, 1985 through 1999: implications for primary prevention. Circulation. 2003;108(6):711–6.
Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, et al. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace. 2012;14(4):528–606.
Rolf S, Kircher S, Arya A, Eitel C, Sommer P, Richter S, et al. Tailored atrial substrate modification based on low-voltage areas in catheter ablation of atrial fibrillation. Circ Arrhythm Electrophysiol. 2014;7(5):825–33.
Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017;14(10):e275.
Kuck KH, Furnkranz A, Chun KR, Metzner A, Ouyang F, Schlüter M, et al. Cryoballoon or radiofrequency ablation for symptomatic paroxysmal atrial fibrillation: reintervention, rehospitalization, and quality-of-life outcomes in the FIRE AND ICE trial. Eur Heart J. 2016;37(38):2858–65.
Kuck KH, Brugada J, Furnkranz A, Metzner A, Ouyang F, Chun KR, et al. Cryoballoon or radiofrequency ablation for paroxysmal atrial fibrillation. N Engl J Med. 2016;374(23):2235–45.
Kuniss M, Greiss H, Pajitnev D, Akkaya E, Deubner N, Hain A, et al. Cryoballoon ablation of persistent atrial fibrillation: feasibility and safety of left atrial roof ablation with generation of conduction block in addition to antral pulmonary vein isolation. Europace. 2017;19(7):1109–15.
Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace. 2016;18(11):1609–78.
Tilz RR, Rillig A, Thum AM, Arya A, Wohlmuth P, Metzner A, et al. Catheter ablation of longstanding persistent atrial fibrillation: 5-year outcomes of the Hamburg sequential ablation strategy. J Am Coll Cardiol. 2012;60:1921–9.
Vogler J, Willems S, Sultan A, Schreiber D, Lüker J, Servatius H, et al. Pulmonary vein isolation versus defragmentation: the CHASE-AF clinical trial. J Am Coll Cardiol. 2015;66(24):2743–52.
Wynn GJ, Panikker S, Morgan M, Hall M, Waktare J, Markides V, et al. Biatrial liner ablation in sustained nonpermanent AF: results of the substrate modification with ablation and antiarrhythmic drugs in nonpermanent atrial fibrillation (SMAN-PAF) trial. Heart Rhythm. 2016;13(2):399–406.
Bai R, Di Biase L, Mohanty P, et al. Proven isolation of the pulmonary vein antrum with or without left atrial posterior wall isolation in patients with persistent atrial fibrillation. Heart Rhythm. 2016;13(1):132–40.
Oakes RS, Badger TJ, Kholmovski EG, Akoum N, Burgon NS, Fish EN, et al. Detection and quantification of left atrial structural remolding with delayed-enhancement magnetic resonance imaging in patients with atrial fibrillation. Circulation. 2009;119(13):1758–67.
Yang G, Yang B, Wei Y, et al. Catheter ablation of nonparoxysmal atrial fibrillation using electrophysiologically guided substrate modification during sinus rhythm after pulmonary vein isolation. Circ Arrhythm Electrophysiol. 2016;9(2):e3382.
Yang B, Jiang C, Lin Y, et al. STABLE-SR (Electrophysiological Substrate Ablation in the Left Atrium During Sinus Rhythm) for the Treatment of Nonparoxysmal Atrial Fibrillation: A Prospective, Multicenter Randomized Clinical Trial. Circ Arrhythm Electrophysiol. 2017;10:e005405.
Reissmann B, Metzner A, Kuck KH. Cryoballoon ablation versus radiofrequency ablation for atrial fibrillation. Trends Cardiovasc Med. 2017;27(4):271–7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional (medical ethics committee of Second Hospital of Tianjin Medical University, KL2019K013) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Xu, G., Cai, J., Liu, Z. et al. Clinical efficacy of “ICE-FIRE” ablation for non-paroxysmal atrial fibrillation. J Interv Card Electrophysiol 60, 205–211 (2021). https://doi.org/10.1007/s10840-020-00725-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-020-00725-x