
Abstract
Introduction
Clinical trials have failed to reliably show improved outcomes with utilization of contact-force sensing (CFS) radiofrequency (RF) ablation catheters. It is unknown whether the unfavorable outcomes observed in these trials are attributable to inexperience with CFS technology.
Objectives
To compare catheter ablation outcomes of stepwise linear ablation with versus without CFS technology and to assess the impact of operator experience with CFS technology on procedural outcomes.
Methods
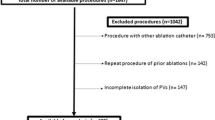
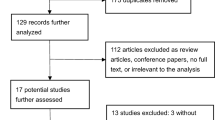
Clinical outcomes were evaluated in 228 consecutive NPAF patients undergoing first-time left atrial ablation using a stepwise linear approach. Arrhythmia recurrence was assessed using 2-week event monitors at 3-month intervals following index ablation.
Results
A total of 228 patients were included in our study. There was no statistically significant difference in risk of recurrent atrial arrhythmias at 12 and 24 months between CFS and non-CFS patients (p = 0.5 and p = 0.169). The time to recurrence of atrial arrhythmias at 24 months in the second half of CFS patients was significantly lower when compared to both the first half of CFS patients (p = 0.002) and non-CFS patients (p = 0.005).
Conclusion
While there was no difference in overall outcomes between CFS and non-CFS ablation using a stepwise linear approach in patients with NPAF, procedural efficacy of the second half of CFS patients was significantly improved compared to both the first half of CFS patients and all non-CFS patients. Lack of benefit seen in clinical trials using CFS technology may be related to operator inexperience with CFS ablation catheters at the time of the trials.


Similar content being viewed by others

References
Verma A, Jiang C, Betts TR, Chen J, Deisenhofer I, Mantovan R, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372:1812–22.
January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:e199–267.
Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, et al. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace. 2012;14:528–606.
Vogler J, Willems S, Sultan A, Schreiber D, Lüker J, Servatius H, et al. Pulmonary vein isolation versus defragmentation: The CHASE-AF Clinical Trial. J Am Coll Cardiol. 2015;66:2743–52.
Reichlin T, Lane C, Nagashima K, Nof E, Chopra N, Ng J, et al. Feasibility, efficacy, and safety of radiofrequency ablation of atrial fibrillation guided by monitoring of the initial impedance decrease as a surrogate of catheter contact. J Cardiovasc Electrophysiol. 2015;26:390–6.
Ullah W, Hunter RJ, Baker V, Dhinoja MB, Sporton S, Earley MJ, et al. Target indices for clinical ablation in atrial fibrillation: insights from contact force, electrogram, and biophysical parameter analysis. Circ Arrhythm Electrophysiol. 2014;7:63–8.
Natale A, Reddy VY, Monir G, Wilber DJ, Lindsay BD, McElderry H, et al. Paroxysmal AF catheter ablation with a contact force sensing catheter: results of the prospective, multicenter SMART-AF trial. J Am Coll Cardiol. 2014;64:647–56.
Kuck K-H, Reddy VY, Schmidt B, Natale A, Neuzil P, Saoudi N, et al. A novel radiofrequency ablation catheter using contact force sensing: Toccata study. Heart Rhythm. 2012;9:18–23.
Nair GM, Yeo C, MacDonald Z, Ainslie MP, Alqarawi WA, Nery PB, et al. Three-year outcomes and reconnection patterns after initial contact force guided pulmonary vein isolation for paroxysmal atrial fibrillation. J Cardiovasc Electrophysiol. 2017;28:984–93.
Steven D, Sultan A, Reddy V, Luker J, Altenburg M, Hoffmann B, et al. Benefit of pulmonary vein isolation guided by loss of pace capture on the ablation line: results from a prospective 2-center randomized trial. J Am Coll Cardiol. 2013;62:44–50.
Lin H, Chen Y-H, Hou J-W, Lu Z-Y, Xiang Y, Li Y-G. Role of contact force-guided radiofrequency catheter ablation for treatment of atrial fibrillation: a systematic review and meta-analysis. J Cardiovasc Electrophysiol. 2017;28:994–1005.
Wynn GJ, Das M, Bonnett LJ, Panikker S, Wong T, Gupta D. Efficacy of catheter ablation for persistent atrial fibrillation: a systematic review and meta-analysis of evidence from randomized and nonrandomized controlled trials. Circ Arrhythm Electrophysiol. 2014;7:841–52.
Hussein AA, Barakat AF, Saliba WI, et al. Persistent atrial fibrillation ablation with or without contact force sensing. J Cardiovasc Electrophysiol. 2017;28:483–8.
Dong J-Z, Sang C-H, Yu R-H, Long D-Y, Tang R-B, Jiang C-X, et al. Prospective randomized comparison between a fixed “2C3L” approach vs. stepwise approach for catheter ablation of persistent atrial fibrillation. Europace. 2015;17:1798–806.
Scherr D, Khairy P, Miyazaki S, Aurillac-Lavignolle V, Pascale P, Wilton SB, et al. Five-year outcome of catheter ablation of persistent atrial fibrillation using termination of atrial fibrillation as a procedural endpoint. Circ Arrhythm Electrophysiol. 2015;8:18–24.
Galmén K, Harbut P, Freedman J, Jakobsson JG. High frequency jet ventilation for motion management during ablation procedures, a narrative review. Acta Anaesthesiol Scand. 2017;61:1066–74.
Steven D, Reddy VY, Inada K, Roberts-Thomson KC, Seiler J, Stevenson WG, et al. Loss of pace capture on the ablation line: a new marker for complete radiofrequency lesions to achieve pulmonary vein isolation. Heart Rhythm. 2010;7:323–30.
Conti S, Weerasooriya R, Novak P, Champagne J, Lim H, Macle L, Khaykin Y, Pantano A, Verma A. DOI PII: Contact force sensing for ablation of persistent atrial fibrillation: a randomized, Multicenter Trial.
Ullah W, McLean A, Tayebjee MH, Gupta D, Ginks MR, Haywood GA, et al. UK multicentre trials group**: randomized trial comparing pulmonary vein isolation using the SmartTouch catheter with or without real-time contact force data. Heart Rhythm. 2016;13:1761–7.
Kautzner J, Neuzil P, Lambert H, Peichl P, Petru J, Cihak R, et al. EFFICAS II: optimization of catheter contact force improves outcome of pulmonary vein isolation for paroxysmal atrial fibrillation. Europace. 2015;17:1229–35.
Piorkowski C, Kottkamp H, Gerds-Li J-H, Arya A, Sommer P, Dagres N, et al. Steerable sheath catheter navigation for ablation of atrial fibrillation: a case-control study. Pacing Clin Electrophysiol. 2008;31:863–73.
Barbhaiya CR, Baldinger SH, Kumar S, Chinitz JS, Enriquez AD, John R, Stevenson WG, Michaud GF. Downstream overdrive pacing and intracardiac concealed fusion to guide rapid identification of atrial tachycardia after atrial fibrillation ablation. Europace. 2017.
Macle L, Khairy P, Verma A, Weerasooriya R, Willems S, Arentz T, et al. Adenosine following pulmonary vein isolation to target dormant conduction elimination (ADVICE): methods and rationale. Can J Cardiol. 2012;28:184–90.
Villacastin J, Almendral J, Arenal A, Castellano NP, Gonzalez S, Ortiz M, et al. Usefulness of unipolar electrograms to detect isthmus block after radiofrequency ablation of typical atrial flutter. Circulation. 2000;102:3080–5.
van Workum F, Stenstra MHBC, Berkelmans GHK, et al. Learning curve and associated morbidity of minimally invasive esophagectomy: a retrospective multicenter study. Ann Surg. 2017.
ASGE Technology Committee, Maple JT, Abu Dayyeh BK, Chauhan SS, Hwang JH, Komanduri S, et al. Endoscopic submucosal dissection. Gastrointest Endosc. 2015;81:1311–25.
Koedam TWA, Veltcamp Helbach M, van de Ven PM, Kruyt PM, van Heek NT, Bonjer HJ, et al. Transanal total mesorectal excision for rectal cancer: evaluation of the learning curve. Tech Coloproctol. 2018;22:279–87.
Gunda S, Reddy M, Pillarisetti J, Atoui M, Badhwar N, Swarup V, et al. Differences in complication rates between large bore needle and a long micropuncture needle during epicardial access: time to change clinical practice? Circ Arrhythm Electrophysiol. 2015;8:890–5.
Funding
Relationships to industry are all modest and less than $10,000. Dr. Barbhaiya has received speaking fees/honoraria from Abbott, Inc., Biotronik, Inc., Medtronic, Inc., and Zoll, Inc., and received research support from Biotronik, Inc. Dr. Holmes has research support from Abbott. Dr. Aizer has served as a consultant for Biosense Webster, Inc., received research support from Abbott Inc., and Sentreheart, Inc., and received fellowship support from Abbott, Inc., Biotronik, Inc., Boston Scientific, Inc., and Medtronic, Inc. Dr. Chinitz has received speaking fees/honoraria from Abbott, Medtronic, Biotronik, Biosense and Fellowship/Research from Medtronic, Biotronik, and Biosense.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Barbhaiya, C.R., Knotts, R.J., Bockstall, K. et al. Contact-force radiofrequency ablation of non-paroxysmal atrial fibrillation: improved outcomes with increased experience. J Interv Card Electrophysiol 58, 69–75 (2020). https://doi.org/10.1007/s10840-019-00618-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-019-00618-8