
Abstract
Purpose
There are few reports describing ventricular arrhythmias (VAs) from the crux and the corresponding endocardial site, i.e., the basal inferior segment of the interventricular septum (IVS). We aimed to investigate a distinct clinical group of VAs arising from the endocardium at this area in patients with structural heart diseases (SHD).
Methods
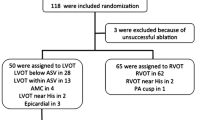
We included 17 patients with SHD and clinically documented VAs. Thirteen patients underwent endocardial mapping only. Three patients underwent both epicardial and endocardial approaches and one had only epicardial mapping. Eighteen VAs were identified, 14 focal and 4 reentrant VAs, confirmed by entrainment.
Results
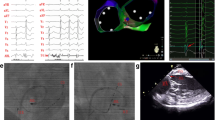
There were 2 VAs from the crux, 5 VAs from the corresponding endocardial site in the right ventricle (RV), and 11 from the site in the left ventricle (LV). Compared with the VAs from RV endocardium, VAs from LV endocardium had a higher R wave in V3 than V2 (V2R/V3R ratio, 1.83 ± 0.84 vs. 0.86 ± 0.38, P = 0.008) and a higher V3 transition ratio percentage (2.16 ± 2.07 vs. 0.58 ± 0.62, P = 0.008). Combining all 16 patients with endocardial mapping, there were also lower bipolar voltages (1.21 ± 1.05 vs. 3.10 ± 2.65 mv, P < 0.0001), lower unipolar voltages (4.05 ± 1.92 vs. 5.75 ± 2.90 mv, P < 0.0001), and longer local electrocardiogram (EGM) lateness (157.6 ± 47.9 vs.140.3 ± 52.5 ms, P = 0.0001) in the dominant chambers.
Conclusions
In VAs from the crux and the corresponding endocardial site, the complete ECG V2R/V3R ratio and V3 transition ratio percentage could differentiate the VAs from the RV or LV endocardium. The lower unipolar, bipolar voltage mapping, and longer EGM lateness are helpful to identify the abnormal substrate in the endocardium in these patients.






Similar content being viewed by others

References
Bunch TJ, Day JD. Right meets left: a common mechanism underlying right and left ventricular outflow tract tachycardias. J Cardiovasc Electrophysiol. 2006;17:1059–61.
Coggins DL, Lee RJ, Sweeney J, Chein WW, Van Hare G, Epstein L, et al. Radiofrequency catheter ablation as a cure for idiopathic tachycardia of both left and right ventricular origin. J Am Coll Cardiol. 1994;23:1333–41.
Doppalapudi H, Yamada T, McElderry HT, Plumb VJ, Epstein AE, Kay GN. Ventricular tachycardia originating from the posterior papillary muscle in the left ventricle: a distinct clinical syndrome. Circ Arrhythm Electrophysiol. 2008;1:23–9.
Tada H, Ito S, Naito S, Kurosaki K, Kubota S, Sugiyasu A, et al. Idiopathic ventricular arrhythmia arising from the mitral annulus. a distinct subgroup of idiopathic ventricular arrhythmias J Am Coll Cardiol. 2005;45:877–86.
Tada H, Tadokoro K, Ito S, Naito S, Hashimoto T, Kaseno K, et al. Idiopathic ventricular arrhythmias originating from the tricuspid annulus: prevalence, electrocardiographic characteristics, and results of radiofrequency catheter ablation. Heart Rhythm. 2007;4:7–16.
Zhu DW, Maloney JD, Simmons TW, Nitta J, Fitzgerald DM, Trohman RG, et al. Radiofrequency catheter ablation for management of symptomatic ventricular ectopic activity. J Am Coll Cardiol. 1995;26:843–9.
Doppalapudi H, Yamada T, Ramaswamy K, Ahn J, Kay GN. Idiopathic focal epicardial ventricular tachycardia originating from the crux of the heart. Heart Rhythm. 2009;6:44–50.
Kawamura M, Gerstenfeld EP, Vedantham V, Rodrigues DM, Burkhardt JD, Kobayashi Y, et al. Idiopathic ventricular arrhythmia originating from the cardiac crux or inferior septum: epicardial idiopathic ventricular arrhythmia. Circ Arrhythm Electrophysiol. 2014;7:1152–8.
Kawamura M, Hsu JC, Vedantham V, Marcus GM, Hsia HH, Gerstenfeld EP, et al. Clinical and electrocardiographic characteristics of idiopathic ventricular arrhythmias with right bundle branch block and superior axis: comparison of apical crux area and posterior septal left ventricle. Heart Rhythm. 2015;12:1137–44.
Komatsu Y, Daly M, Sacher F, Derval N, Pascale P, Roten L, et al. Electrophysiologic characterization of local abnormal ventricular activities in postinfarction ventricular tachycardia with respect to their anatomic location. Heart Rhythm. 2013;10:1630–7.
Betensky BP, Park RE, Marchlinski FE, Hutchinson MD, Garcia FC, Dixit S, et al. The V(2) transition ratio. a new electrocardiographic criterion for distinguishing left from right ventricular outflow tract tachycardia origin J Am Coll Cardiol. 2011;57:2255–62.
Yoshida N, Yamada T, McElderry HT, Inden Y, Shimano M, Murohara T, et al. A novel electrocardiographic criterion for differentiating a left from right ventricular outflow tract tachycardia origin: the V2S/V3R index. J Cardiovasc Electrophysiol. 2014;25:747–53.
Valles E, Bazan V, Marchlinski FE. ECG criteria to identify epicardial ventricular tachycardia in nonischemic cardiomyopathy. Circ Arrhythm Electrophysiol. 2010;3:63–71.
Tung R, Mathuria N, Michowitz Y, Yu R, Buch E, Bradfield J, et al. Functional pace-mapping responses for identification of targets for catheter ablation of scar-mediated ventricular tachycardia. Circ Arrhythm Electrophysiol. 2012;5:264–72.
Polin GM, Haqqani H, Tzou W, Hutchinson MD, Garcia FC, Callans DJ, et al. Endocardial unipolar voltage mapping to identify epicardial substrate in arrhythmogenic right ventricular cardiomyopathy/dysplasia. Heart Rhythm. 2011;8:76–83.
Hutchinson MD, Gerstenfeld EP, Desjardins B, Bala R, Riley MP, Garcia FC, et al. Endocardial unipolar voltage mapping to detect epicardial ventricular tachycardia substrate in patients with nonischemic left ventricular cardiomyopathy. Circ Arrhythm Electrophysiol. 2011;4:49–55.
Sacher F, Lim HS, Derval N, Denis A, Berte B, Yamashita S, et al. Substrate mapping and ablation for ventricular tachycardia: the LAVA approach. J Cardiovasc Electrophysiol. 2015;26:464–71.
Lacroix D, Klug D, Grandmougin D, Jarwe M, Kouakam C, Kacet S. Ventricular tachycardia originating from the posteroseptal process of the left ventricle with inferior wall healed myocardial infarction. Am J Cardiol. 1999 Jul 15;84(2):181–6.
Chopra N, Tokuda M, Ng J, Reichlin T, Nof E, John RM, et al. Relation of the unipolar low-voltage penumbra surrounding the endocardial low-voltage scar to ventricular tachycardia circuit sites and ablation outcomes in ischemic cardiomyopathy. J Cardiovasc Electrophysiol. 2014 Jun;25(6):602–8.
Funding
Taipei Veterans General Hospital (V102B-002, V102E7-003, V103C-042, V103C-126, V103E7-002, VGHUST103-G1-3-1, V104C-131, V104E7-003, VA105C-60), Ministry of Science and Technology (NSC 101-2911-I-008-001, NSC 102-2325-B-010-005, MOST 103-2314-B-075-062-MY3, MOST 104-2314-B-075-065-MY2), and Research Foundation of Cardiovascular Medicine (RFCM 100-02-011, 101-01-001, 104-01-009-01).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All patients gave written informed consent prior to the ablation procedures in accordance with institutional guidelines of the Taipei Veteran General Hospital. The study has been approved by the Institutional Review Board committee of Taipei Veterans General Hospital (IRB No: 2017-06-001 BC).
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Institutional Review Board committee of Taipei Veterans General Hospital (IRB No: 2017-06-001 BC).
Rights and permissions
About this article

Cite this article
Lin, CH., Lo, LW., Lin, YJ. et al. Ventricular arrhythmias originating from the cardiac crux and the basal inferior segment of the interventricular septum in the patients with structural heart diseases: characteristics, mapping, and electrophysiological properties. J Interv Card Electrophysiol 52, 225–236 (2018). https://doi.org/10.1007/s10840-018-0350-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-018-0350-2