
Abstract
Purpose
Since subcutaneous implantable cardioverter defibrillator (S-ICD) introduction, the pre-implant screening based on a dedicated manual ECG tool (MST) was required to assure adequate sensing by the S-ICD. A novel automated screening tool (AST) has been recently developed. We assessed and compared the pass rate with AST and MST, and we measured the agreement between screening tools.
Methods
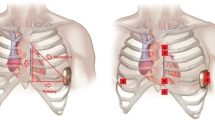
Three electrodes were positioned at locations mimicking the placement of the S-ICD, and ECG recordings were collected in the supine and standing postures at rest. The three sensing vectors were analyzed with the MST and the AST. Eligibility was defined by the presence of at least one or two appropriate vectors in both postures.
Results
A total of 235 patients with an indication to ICD and no need for permanent pacing were enrolled. At least one suitable vector was identified in 214 (91%) patients with MST and 221 (94%) patients with AST (p = 0.219). At least two vectors were appropriate in 162 (69%) patients with MST and 187 (80%) patients with AST (p = 0.008). Overall, out of 1587 ECG analyzed, 1035 (65%) qualifying leads were identified with MST and 1111 (70%) with AST (p = 0.004). The agreement between the results of MST and AST ECG analysis was moderate (Kappa = 0.570; standard error = 0.022; CI = 0.526–0.613). The results were consistent regardless of the underlying cardiomyopathy. The most frequent reason for screening failure with MST was a high-amplitude T-wave (31% of failures). With AST, 23% of recordings that failed with MST for high-amplitude T-wave were classified as acceptable.
Conclusion
The AST is associated with higher pass rate than the standard MST. It seems more tolerant of high-amplitude T-waves. Consequently, the agreement between MST and AST findings was only moderate.




Similar content being viewed by others


References
Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, Kirchhof P, Kjeldsen K, Kuck KH, Hernandez-Madrid A, Nikolaou N, Norekvål TM, Spaulding C, Van Veldhuisen DJ; Task Force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC). 2015 ESC guidelines for the Management of Patients with ventricular arrhythmias and the prevention of sudden cardiac death: the task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC) endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Europace 2015; 17:1601–87.
Weiss R, Knight BP, Gold MR, Leon AR, Herre JM, Hood M, et al. Safety and efficacy of a totally subcutaneous implantable-cardioverter defibrillator. Circulation. 2013;128:944–53.
Lee DS, Krahn AD, Healey JS, Birnie D, Crystal E, Dorian P, et al. Investigators of the Ontario ICD database.. Evaluation of early complications related to de novo cardioverter defibrillator implantation insights from the Ontario ICD database. J Am Coll Cardiol. 2010;55:774–82.
Zeb M, Curzen N, Allavatam V, Wilson D, Yue A, Roberts P, et al. Sensitivity and specificity of the subcutaneous implantable cardioverter defibrillator pre-implant screening tool. Int J Cardiol. 2015;195:205–9.
Brouwer TF, Kooiman KM, Olde Nordkamp LR, van Halm VP, Knops RE. Algorithm-based screening may improve patient selection for the subcutaneous implantable defibrillator. JACC: Clinical Electrophysiology. 2016;2:605–14.
Olde Nordkamp LR, Warnaars JL, Kooiman KM, de Groot JR, Rosenmöller BR, Wilde AA, et al. Which patients are not suitable for a subcutaneous ICD: incidence and predictors of failed QRS-T-wave morphology screening. J Cardiovasc Electrophysiol. 2014;25:494–9.
Randles DA, Hawkins NM, Shaw M, Patwala AY, Pettit SJ, Wright DJ. How many patients fulfil the surface electrocardiogram criteria for subcutaneous implantable cardioverter-defibrillator implantation? Europace. 2014;16:1015–21.
Groh CA, Sharma S, Pelchovitz DJ, Bhave PD, Rhyner J, Verma N, et al. Use of an electrocardiographic screening tool to determine candidacy for a subcutaneous implantable cardioverter-defibrillator. Heart Rhythm. 2014;11:1361–6.
Ziacchi M, Corzani A, Diemberger I, Martignani C, Marziali A, Mazzotti A, et al. Electrocardiographic eligibility for subcutaneous implantable cardioverter defibrillator: evaluation during bicycle exercise. Heart Lung Circ. 2016;25:476–83.
Okamura H, McLeod CJ, DeSimone CV, Webster TL, Bonnichsen CR, Grogan M, et al. Right parasternal lead placement increases eligibility for subcutaneous implantable cardioverter defibrillator therapy in adults with congenital heart disease. Circ J. 2016;80:1328–35.
Wilson DG, Zeb M, Veldtman G, Dimitrov BD, Morgan JM. Left and right parasternal sensing for the S-ICD in adult congenital heart disease patients and normal controls. Pacing Clin Electrophysiol. 2016;39:282–90.
Francia P, Adduci C, Palano F, Semprini L, Serdoz A, Montesanti D, et al. Eligibility for the subcutaneous implantable cardioverter-defibrillator in patients with hypertrophic cardiomyopathy. J Cardiovasc Electrophysiol. 2015;26:893–9.
Maurizi N, Olivotto I, Olde Nordkamp LR, Baldini K, Fumagalli C, Brouwer TF, et al. Prevalence of subcutaneous implantable cardioverter-defibrillator candidacy based on template ECG screening in patients with hypertrophic cardiomyopathy. Heart Rhythm. 2016;13:457–63.
Srinivasan NT, Patel KH, Qamar K, Taylor A, Bacà M, Providência R, Tome-Esteban M, Elliott PM, Lambiase PD. Disease severity and exercise testing reduce subcutaneous implantable cardioverter-defibrillator left sternal ECG screening success in hypertrophic cardiomyopathy. Circ Arrhythm Electrophysiol. 2017;10(4). https://doi.org/10.1161/CIRCEP.117.004801.
Santini L, Pappalardo A, Schirripa V, Danisi N, Forleo GB, Ammirati F. Oversensing of an unexpected atrial flutter. A new tool to improve detection of supraventricular arrhythmias in subcutaneous implantable cardioverter-defibrillators. Heart Rhythm Case Rep. 2017;3:286–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
P. Francia served as consultant and received speaker’s fees from Boston Scientific. S. Valsecchi and M. Lovecchio are employees of Boston Scientific. The other authors report no conflicts.
Ethical approval
The study was approved by the Local Ethics Committee.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Francia, P., Ziacchi, M., De Filippo, P. et al. Subcutaneous implantable cardioverter defibrillator eligibility according to a novel automated screening tool and agreement with the standard manual electrocardiographic morphology tool. J Interv Card Electrophysiol 52, 61–67 (2018). https://doi.org/10.1007/s10840-018-0326-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-018-0326-2