
Abstract
Purpose
Dual-site epicardial left ventricular (LV) pacing represents one strategy to improve acute cardiac resynchronization therapy (CRT) response. However, the feasibility of this approach in the longer term may be hindered by system complexity. We assessed chronic outcomes of patients receiving dual-site LV pacing.
Methods
Twenty patients with conventional CRT criteria were implanted with dual-site epicardial LV leads connected with bifurcating adapter. Mean energy required to capture the LV was calculated using threshold, impedance and pulse width. Values were obtained during implant and the following day. Follow-up data included lead parameters, ventricular arrhythmias and mortality.
Results
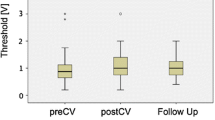
Nineteen patients had successful dual LV lead placement. Mean age was 66 ± 11 years, mean left ventricular ejection fraction (LVEF) 26 % ± 8 and 50 % ischemic etiology. Mean energy to capture the LV was 1.95 μJ for LV1 during implant, rising to 8.61 μJ at day 1, p = 0.03. The energy required for LV2 was 2.37 μJ during implant, 11.55 μJ the next day, p = 0.004. Eleven percent had LV2 turned off during the implant due to high thresholds and/or a worsened acute hemodynamic response. Eleven percent had LV2 turned off day 1 post implant due to inability to capture LV2 at maximum output. All remaining 15 patients had LV2 programmed off, with a mean time of 255 days from implant. Thirty-two percent of patients received ATP or shock, and sixteen percent died over a mean follow-up of 1271 days. Thirty-seven percent of patients required generator replacement with mean longevity of 42 months, far shorter than the suggested lifespan of the device (58 months), p = 0.006.
Conclusion
Multisite epicardial LV lead placement may be acutely feasible and demonstrate beneficial hemodynamic results at implantation. Long-term delivery of this therapy is however problematic due to technical issues with pacing through the bifurcating adapter. This suggests the feasibility of this form of multisite CRT is limited.




Similar content being viewed by others


References
Cleland, J. F. G., Daubert, J.-C., Erdnabb, E., Freemantle, E., Gras, D., Kappenberger, L., Tavazzi, L., & CARE-HF Study Investigators. (2005). The effect of cardiac resynchronization on morbidity and mortality in heart failure. New England Journal of Medicine, 352, 1539–1549.
Cazeau, S., Leclercq, C., Lavergne, T., Walker, S., Varma, C., Linde, C., et al. (2001). Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. New England Journal of Medicine, 344(12), 873–880.
Bristow, M. R., Saxon, L. A., Boehmer, J., Krueger, S., Kass, D. A., De Marco, T., et al. (2004). Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. New England Journal of Medicine, 350(21), 2140–2150.
Derval, N., Steendijk, P., Gula, L. J., Deplagne, A., Laborderie, J., Sacher, F., et al. (2010). Optimizing hemodynamics inHeart failure patients by systematic screening of left ventricular pacing sites. Journal of the American College of Cardiology, 55(6), 566–575.
Leclercq, C., & Kass, D. A. (2002). Retiming the failing heart: principles and current clinical status of cardiac resynchronization. Journal of the American College of Cardiology, 39(2), 194–201.
Mullens, W., Grimm, R. A., Verga, T., Dresing, T., Starling, R. C., Wilkoff, B. L., & Tang, W. H. W. (2009). Insights from a cardiac resynchronization optimization clinic as part of a heart failure disease management program. Journal of the American College of Cardiology, 53(9), 765–773.
Bleeker, G. B. (2006). Effect of posterolateral scar tissue on clinical and echocardiographic improvement after cardiac resynchronization therapy. Circulation, 113(7), 969–976.
Khan, F. Z., Virdee, M. S., Palmer, C. R., Pugh, P. J., O’Halloran, D., Elsik, M., et al. (2012). Targeted left ventricular lead placement to guide cardiac resynchronization therapy. Journal of the American College of Cardiology, 59(17), 1509–1518.
Adelstein, E., Alam, M. B., Schwartzman, D., Jain, S., Marek, J., Gorcsan, J., & Saba, S. (2014). Effect of echocardiography-guided left ventricular lead placement for cardiac resynchronization therapy on mortality and risk of defibrillator therapy for ventricular arrhythmias in heart failure patients (from the Speckle Tracking Assisted Resynchronization Therapy for Electrode Region [STARTER] trial). The American Journal of Cardiology, 113(9), 1518–1522.
Ploux, S., Strik, M., van Hunnik, A., van Middendorp, L., Kuiper, M., & Prinzen, F. W. (2014). Acute electrical and hemodynamic effects of multisite left ventricular pacing for cardiac resynchronization therapy in the dyssynchronous canine heart. Heart Rhythm, 11(1), 119–125.
Lenarczyk, R., Kowalski, O., Kukulski, T., Pruszkowska-Skrzep, P., Sokal, A., Szulik, M., et al. (2009). Mid-term outcomes of triple-site vs. conventional cardiac resynchronization therapy: a preliminary study. International Journal of Cardiology, 133(1), 87–94.
Lenarczyk, R., Kowalski, O., Kukulski, T., Szulik, M., Pruszkowska-Skrzep, P., Zielinska, T., et al. (2007). Triple-site biventricular pacing in patients undergoing cardiac resynchronization therapy: a feasibility study. Europace, 9(9), 762–767.
Leclercq, C., Gadler, F., Kranig, W., Ellery, S., Gras, D., Lazarus, A., et al. (2008). A randomized comparison of triple-site versus dual-site ventricular stimulation in patients with congestive heart failure. Journal of the American College of Cardiology, 51(15), 1455–1462.
Rogers, D. P. S., Lambiase, P. D., Lowe, M. D., & Chow, A. W. C. (2014). A randomized double-blind crossover trial of triventricular versus biventricular pacing in heart failure. European Journal of Heart Failure, 14(5), 495–505.
Ginks, M. R., Duckett, S. G., Kapetanakis, S., Bostock, J., Hamid, S., Shetty, A., et al. (2012). Multi-site left ventricular pacing as a potential treatment for patients with postero-lateral scar: insights from cardiac magnetic resonance imaging and invasive haemodynamic assessment. Europace, 14(3), 373–379.
Sohal, M., Duckett, S. G., Zhuang, X., Shi, W., Ginks, M., Shetty, A., et al. (2014). A prospective evaluation of cardiovascular magnetic resonance measures of dyssynchrony in the prediction of response to cardiac resynchronization therapy. Journal of cardiovascular magnetic resonance: official journal of the Society for Cardiovascular Magnetic Resonance, 16(1), 58.
Ypenburg, C., Roes, S. D., Bleeker, G. B., Kaandorp, T. A. M., de Roos, A., Schalij, M. J., et al. (2007). Effect of total scar burden on contrast-enhanced magnetic resonance imaging on response to cardiac resynchronization therapy. The American Journal of Cardiology, 99(5), 657–660.
Singh, J. P., Klein, H. U., Huang, D. T., Reek, S., Kuniss, M., Quesada, A., et al. (2011). Left ventricular lead position and clinical outcome in the multicenter automatic defibrillator implantation trial-cardiac resynchronization therapy (MADIT-CRT) trial. Circulation, 123(11), 1159–1166.
SJM CRM. (2007). Frontier™ II Model 5586 Model 5596, Biventricular Cardiac Resynchronization Device with AF Suppression™ Algorithm User’s Manual© 2007
SJM CRM. Atlas® II Models V-168, V-265, V-365 Atlas® II+ Models V-268, V-366 Cardiac Resynchronization Device, Implantable Cardioverter-Defibrillator User’s Manual © 2007
SJM. CRM. Bradycardia and Tachycardia Devices Merlin™ Patient Care System Help Manual. [For the following devices: Accent™, Accent™ RF, Accent™ ST, Accent ™ ST MRI Allure™, Allure Quadra™, Allure Quadra™ RF, Allure™ RF AnalyST™, AnalyST Accel™ Anthem™, Anthem™ RF Assurity™, Assurity™ + Auricle™ Current™, Current™ RF, Current™+, Current Accel™ Ellipse™ Endurity™ Fortify™, Fortify™ ST, Fortify Assura™ Promote™, Promote™ RF, Promote™+, Promote™ LAP, Promote Accel™, Promote™ Q, Promote Quadra™ Quadra Allure MP™, Quadra Allure MP™ RF, Quadra Assura™, Quadra Assura MP™ Unify™, Unify Quadra™, Unify Quadra MP™, Unify Assura™] 2014 St. Jude Medical, Inc.
Shetty, A. K., Duckett, S. G., Bostock, J., Roy, D., Ginks, M., Hamid, S., et al. (2011). Initial single-center experience of a quadripolar pacing lead for cardiac resynchronization therapy. Pacing and Clinical Electrophysiology: PACE, 34(4), 484–489.
Forleo, G. B., Rocca Della, D. G., Papavasileiou, L. P., Molfetta, A. D., Santini, L., & Romeo, F. (2011). Left ventricular pacing with a new quadripolar transvenous lead for CRT: early results of a prospective comparison with conventional implant outcomes. Heart Rhythm, 8(1), 31–37.
Sperzel, J., Dänschel, W., Gutleben, K.-J., Kranig, W., Mortensen, P., Connelly, D., et al. (2012). First prospective, multi-centre clinical experience with a novel left ventricular quadripolar lead. Europace, 14(3), 365–372.
Tomassoni, G., Baker, J., Corbisiero, R., Love, C., Martin, D., Niazi, I., et al. (2013). Postoperative performance of the quartet ®left ventricular heart lead. Journal of Cardiovascular Electrophysiology, 24(4), 449–456.
Shetty, A. K., Duckett, S. G., Ma, Y. L., Kapetanakis, S., Ginks, M., Bostock, J., et al. (2012). The acute hemodynamic response to LV pacing within individual branches of the coronary sinus using a quadripolar lead. Pacing and Clinical Electrophysiology, 35(2), 196–203.
Asbach, S., Hartmann, M., Wengenmayer, T., Graf, E., Bode, C., & Biermann, J. (2013). Vector selection of a quadripolar left ventricular pacing lead affects acute hemodynamic response to cardiac resynchronization therapy: a randomized cross-over trial. PloS One, 8(6), e67235.
Pappone, C., Calović, Z., Vicedomini, G., Cuko, A., McSpadden, L. C., Ryu, K., et al. (2014). Multipoint left ventricular pacing improves acute hemodynamic response assessed with pressure-volume loops in cardiac resynchronization therapy patients. Heart Rhythm, 11(3), 394–401.
Niederer, S. A., Shetty, A. K., Plank, G., Bostock, J., Razavi, R., Smith, N. P., & Rinaldi, C. A. (2011). Biophysical modeling to simulate the response to multisite left ventricular stimulation using a quadripolar pacing lead. Pacing and Clinical Electrophysiology, 35(2), 204–214.
Acknowledgments
JMB acknowledges support from the Biomedical Research Centre at Guy’s and St Thomas’s NHS Foundation Trust and the Rosetrees Trust. MG, MS and SC have received educational grants from St Jude Medical Ltd. TJ has received a research grant from Medtronic. CAR is consultant to St Jude Medical Ltd, Medtronic and Spectranetics and receives research funding from St Jude Medical and Medtronic.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix S1
Individual patient capture threshold voltages for LV1 and LV2 demonstrating a large variation between cases. (DOCX 26 kb)
Rights and permissions
About this article

Cite this article
Behar, J.M., Bostock, J., Ginks, M. et al. Limitations of chronic delivery of multi-vein left ventricular stimulation for cardiac resynchronization therapy. J Interv Card Electrophysiol 42, 135–142 (2015). https://doi.org/10.1007/s10840-014-9971-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-014-9971-2