
Abstract
Instruction
Preablation transesophageal echocardiography (TEE) is dispensable for the patients with planned catheter ablation for atrial fibrillation (AF) and having received at least a 3-week oral anticoagulation therapy according to the recommendations of the Venice Consensus. But the role of prior TEE and the effect of preablation short-term oral anticoagulation drugs (OACs) under the circumstance are still unclear.
Methods and Results
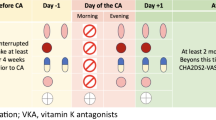
A total of 188 patients with planned catheter ablation for AF and without previous long-term oral anticoagulation, whose duration of AF exceeded 48 h, were randomly divided into receiving 3-week OACs (OACs group) before heparin bridging or receiving no prior OACs (N-OACs group). Follow-up was performed until a TEE had been performed on all the cases before ablation. Consequently, the prevalence of atrial thrombi is 6.3% and 11.7%, respectively (P < 0.05), and the prevalence of minor bleeding is 5.3% and 0%, respectively (P < 0.05), in OACs and N-OACs group. There was no thrombotic event, major hemorrhage, in both groups.
Conclusion
After a 3-week effective oral anticoagulation, atrial thrombi could be resolved partly but not completely in the patients with AF who had not received long-term oral anticoagulation previously. To ensure safety, prior TEE may be necessary for the patients with planned catheter ablation for AF.

Similar content being viewed by others

References
Kottkamp, H., Tanner, H., Kobza, R., Schirdewahn, P., Dorszewski, A., Gerds-Li, J. H., et al. (2004). Time courses and quantitative analysis of atrial fibrillation episode number and duration after circular plus linear left atrial lesions: Trigger elimination or substrate modification: Early or delayed cure. Journal of the American College of Cardiology, 44, 869–877.
Pappone, C., Rosanio, S., Augello, G., Gallus, G., Vicedomini, G., Mazzone, P., et al. (2003). Mortality, morbidity, and quality of life after circumferential pulmonary vein ablation for atrial fibrillation: Outcomes from a controlled nonrandomized long-term study. Journal of the American College of Cardiology, 42, 185–197.
Oral, H., Pappone, C., Chugh, A., Good, E., Bogun, F., Pelosi Jr, F., et al. (2006). Circumferential pulmonary-vein ablation for chronic atrial fibrillation. The New England Journal of Medicine, 354, 934–941.
Pappone, C., Manguso, F., Vicedomini, G., Gugliotta, F., Santinelli, O., Ferro, A., et al. (2004). Prevention of iatrogenic atrial tachycardia after ablation of atrial fibrillation: A prospective randomized study comparing circumferential pulmonary vein ablation with a modified approach. Circulation, 110, 3036–3042.
Di Biase, L., Fahmy, T. S., Wazni, O. M., Bai, R., Patel, D., Lakkireddy, D., et al. (2006). Pulmonary vein total occlusion following catheter ablation for atrial fibrillation: Clinical implications after long-term follow-up. Journal of the American College of Cardiology, 48, 2493–2499.
Fuster, V., Ryden, L. E., Cannom, D. S., Crijns, H. J., Curtis, A. B., Ellenbogen, K. A., et al. (2006). Acc/aha/esc 2006 guidelines for the management of patients with atrial fibrillation—executive summary: A report of the American college of cardiology/American heart association task force on practice guidelines and the European society of cardiology committee for practice guidelines (writing committee to revise the 2001 guidelines for the management of patients with atrial fibrillation). Journal of the American College of Cardiology, 48, 854–906.
Natale, A., Raviele, A., Arentz, T., Calkins, H., Chen, S. A., Haissaguerre, M., et al. (2007). Venice chart international consensus document on atrial fibrillation ablation. Journal of Cardiovascular Electrophysiology, 18, 560–580.
Manning, W. J., Silverman, D. I., Gordon, S. P., Krumholz, H. M., & Douglas, P. S. (1993). Cardioversion from atrial fibrillation without prolonged anticoagulation with use of transesophageal echocardiography to exclude the presence of atrial thrombi. The New England Journal of Medicine, 328, 750–755.
Liu, X., Dong, J., Mavrakis, H. E., Hu, F., Long, D., Fang, D., et al. (2006). Achievement of pulmonary vein isolation in patients undergoing circumferential pulmonary vein ablation: A randomized comparison between two different isolation approaches. Journal of Cardiovascular Electrophysiology, 17, 1263–1270.
Palareti, G., Leali, N., Coccheri, S., Poggi, M., Manotti, C., D'Angelo, A., et al. (1996). Bleeding complications of oral anticoagulant treatment: An inception-cohort, prospective collaborative study (iscoat). Italian study on complications of oral anticoagulant therapy. Lancet, 348, 423–428.
Sun, Y. H. H. D. (2004). The efficiency and safety of anticoagulation therapy in atrial fibrillation in Chinese. Chinese Journal of Internal Medicine, 43, 258–260 in Chinese.
Xue, J. P. H. B., Wang, L. Q., et al. (2004). Clinical study of oral anticoagulation with warfarin for nonvascular atrial fibrillation. Clinical Focus [In Chinese], 19, 875–876.
Douketis, J. D., Johnson, J. A., & Turpie, A. G. (2004). Low-molecular-weight heparin as bridging anticoagulation during interruption of warfarin: Assessment of a standardized periprocedural anticoagulation regimen. Archives of Internal Medicine, 164, 1319–1326.
Kovacs, M. J., Kearon, C., Rodger, M., Anderson, D. R., Turpie, A. G., Bates, S. M., et al. (2004). Single-arm study of bridging therapy with low-molecular-weight heparin for patients at risk of arterial embolism who require temporary interruption of warfarin. Circulation, 110, 1658–1663.
Klein, A. L., Jasper, S. E., Katz, W. E., Malouf, J. F., Pape, L. A., Stoddard, M. F., et al. (2006). The use of enoxaparin compared with unfractionated heparin for short-term antithrombotic therapy in atrial fibrillation patients undergoing transoesophageal echocardiography-guided cardioversion: Assessment of cardioversion using transoesophageal echocardiography (acute) II randomized multicentre study. European Heart Journal, 27, 2858–2865.
Hirsh, J. (1992). Oral anticoagulant therapy. Urgent need for standardization. Circulation, 86, 1332–1335.
Collins, L. J., Silverman, D. I., Douglas, P. S., & Manning, W. J. (1995). Cardioversion of nonrheumatic atrial fibrillation. Reduced thromboembolic complications with 4 weeks of precardioversion anticoagulation are related to atrial thrombus resolution. Circulation, 92, 160–163.
Corrado, G., Tadeo, G., Beretta, S., Tagliagambe, L. M., Manzillo, G. F., Spata, M., et al. (1999). Atrial thrombi resolution after prolonged anticoagulation in patients with atrial fibrillation. Chest, 115, 140–143.
Newcombe, R. G. (1998). Two-sided confidence intervals for the single proportion: Comparison of seven methods. Statistics in Medicine, 17, 857–872.
Antonielli, E., Pizzuti, A., Gandolfo, N., Sclavo, M., Tanga, M., Riva, G., et al. (1997). [anticoagulation and electrical cardioversion of chronic atrial fibrillation: Proposal for an abbreviated protocol]. Giornale Italiano di Cardiologia, 27, 803–810.
Klein, A. L., Murray, R. D., Grimm, R. A., Li, J., Apperson-Hansen, C., Jasper, S. E., et al. (2003). Bleeding complications in patients with atrial fibrillation undergoing cardioversion randomized to transesophageal echocardiographically guided and conventional anticoagulation therapies. The American Journal of Cardiology, 92, 161–165.
Jaber, W. A., Prior, D. L., Thamilarasan, M., Grimm, R. A., Thomas, J. D., Klein, A. L., et al. (2000). Efficacy of anticoagulation in resolving left atrial and left atrial appendage thrombi: A transesophageal echocardiographic study. American Heart Journal, 140, 150–156.
Yamaguchi, T. (2000). Optimal intensity of warfarin therapy for secondary prevention of stroke in patients with nonvalvular atrial fibrillation: A multicenter, prospective, randomized trial. Japanese nonvalvular atrial fibrillation-embolism secondary prevention cooperative study group. Stroke, 31, 817–821.
Gage, B. F., Fihn, S. D., & White, R. H. (2000). Management and dosing of warfarin therapy. The American Journal of Medicine, 109, 481–488.
Manning, W. J., Silverman, D. I., Keighley, C. S., Oettgen, P., & Douglas, P. S. (1995). Transesophageal echocardiographically facilitated early cardioversion from atrial fibrillation using short-term anticoagulation: Final results of a prospective 4.5-year study. Journal of the American College of Cardiology, 25, 1354–1361.
Stoddard, M. F., Dawkins, P. R., Prince, C. R., & Ammash, N. M. (1995). Left atrial appendage thrombus is not uncommon in patients with acute atrial fibrillation and a recent embolic event: A transesophageal echocardiographic study. Journal of the American College of Cardiology, 25, 452–459.
Sadler, D. B. J. (1991). Left atrial thrombi in nonrheumatic atrial fibrillation: Assessment of prevalence by transesophageal echocardiography. Circulation, 84, II693 abstract.
Seidl, K., Rameken, M., Drogemuller, A., Vater, M., Brandt, A., Schwacke, H., et al. (2002). Embolic events in patients with atrial fibrillation and effective anticoagulation: Value of transesophageal echocardiography to guide direct-current cardioversion. Final results of the Ludwigshafen Observational Cardioversion Study. Journal of the American College of Cardiology, 39, 1436–1442.
Klein, A. L., Grimm, R. A., Jasper, S. E., Murray, R. D., Apperson-Hansen, C., Lieber, E. A., et al. (2006). Efficacy of transesophageal echocardiography-guided cardioversion of patients with atrial fibrillation at 6 months: A randomized controlled trial. American Heart Journal, 151, 380–389.
Klein, A. L., Grimm, R. A., Murray, R. D., Apperson-Hansen, C., Asinger, R. W., Black, I. W., et al. (2001). Use of transesophageal echocardiography to guide cardioversion in patients with atrial fibrillation. The New England Journal of Medicine, 344, 1411–1420.
Klein, A. L., Murray, R. D., Becker, E. R., Culler, S. D., Weintraub, W. S., Jasper, S. E., et al. (2004). Economic analysis of a transesophageal echocardiography-guided approach to cardioversion of patients with atrial fibrillation: The acute economic data at eight weeks. Journal of the American College of Cardiology, 43, 1217–1224.
de Luca, I., Sorino, M., De Luca, L., Colonna, P., Del Salvatore, B., & Corliano, L. (2005). Pre- and post-cardioversion transesophageal echocardiography for brief anticoagulation therapy with enoxaparin in atrial fibrillation patients: A prospective study with a 1-year follow-up. International Journal of Cardiology, 102, 447–454.
Acknowledgments
This work was supported by the Beijing Anzhen Hospital, Capital University of Medical Sciences, and Beijing Institute of Heart Lung and Blood Vessel Diseases. We thank Dr Guangxia Wei for her valuable suggestions regarding echocardiography.
Funding
This work was supported by grants from Beijing “Ten, hundred and thousand” Medical Talented Man Project Special Fund (NO 06-003).
Conflict of interest
None declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
He, H., Kang, J., Tao, H. et al. Conventional oral anticoagulation may not replace prior transesophageal echocardiography for the patients with planned catheter ablation for atrial fibrillation. J Interv Card Electrophysiol 24, 19–26 (2009). https://doi.org/10.1007/s10840-008-9322-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-008-9322-2