
Abstract
Background
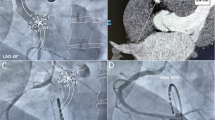
His Bundle ablation (HBA) with permanent pacemaker (PPM) implantation is an effective strategy for controlling heart rate in symptomatic patients with rapid atrial fibrillation (AF), resistant to pharmacologic therapy. The standard double vein (DV) approach involves mapping and HBA from a femoral approach to achieve complete heart block (CHB), while single chamber (SC), dual chamber (DC), or biventricular (BiV) PPM is then placed via a subclavian approach.
Methods
We compared 7 patients with drug-resistant rapid AF who underwent the standard DV approach to 8 patients who underwent a single vein (SV) approach, in which HBA and PPM implantation were performed through the subclavian vein. The two groups were compared for acute success in creating CHB, total procedure and fluoroscopy times and patient discomfort. Results are expressed as mean ± standard error (SEM).
Results
The procedure times for the SV versus DV were 70.4 ± 11.4 v 100.0 ± 19.2 min, and the fluoroscopy times, 13.9 ± 3.1 (SV) v 13.0 ± 2.9 (DV). All patients were discharged in stable condition with CHB and SC, DC pacemaker or BiV/Implantable Cardioverter Defibrillator (ICD). CHB with symptomatic improvement was maintained in all patients over a mean follow-up period of 22.6 months (SV), and 9.6 months (DV).
Conclusion
The SV approach for HBA combined with PPM implantation was at least as effective and may be more efficient than the classic DV approach, and should be considered as an alternative to DV technique to reduce procedural time and patient discomfort.

Similar content being viewed by others


References
Feinberg, W. M., Blackshear, J. L., Laupacis, A., et al. (1995). Prevalence, age distribution, and gender of patients with atrial fibrillation: Analysis and implications. Archives of Internal Medicine, 155, 469–473.
Maisel, W. H., & Stevenson, L. W. (2003). Atrial fibrillation in heart failure: epidemiology, pathophysiology and rationale for therapy. The American Journal of Cardiology, 91, 2D–8D.
Grogan, M., Smith, H. C., Gersh, B. J., & Wood, D. L. (1992). Left Ventricular dysfunction due to atrial fibrillation in patients initially believed to have idiopathic dilated cardiomyopathy. The American Journal of Cardiology, 69, 1570–1573.
Wyse, D. G., Waldo, A. L., DiMarco, J. P., Domanski, M. J., Rosenberg, Y., Scron, E. B., et al. (2002). Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) Investigators. A comparison of rate control and rhythm control in patients with atrial fibrillation. The New England Journal of Medicine, 347, 1825–1833.
McNamara, R. L., et al. (2003). Management of atrial fibrillation: review of the evidence for the role of pharmacologic therapy, electrical cardioversion and echocardiography. Annals of Internal Medicine, 139, 1018–1033.
AFFIRM Investigators (2003). First antiarrhythmic drug substudy. Maintenance of sinus rhythm in patients with atrial fibrillation. Journal of the American College of Cardiology, 42, 20–29.
Neal, G. K., Ellenbogen, K. A., Giudici, M., Redfield, M. M., Jenkins, L. S., Mianulli, M., & Wilkoff, B. (1998). The Ablate and Pace Trial (APT): a prospective trial of catheter ablation of the AV conduction system and permanent pacemaker implantation for treatment of atrial fibrillation. Journal of Interventional Cardiac Electrophysiology, 2, 121–135.
Weerasooriya, R., Davis, M., Powell, A., Szili-Torok, T., Shah, C., Whally, D., et al. (2003). The Australian Intervention Randomized Control of Rate in Atrial Fibrillation Trial (AIRCRAFT). Journal of the American College of Cardiology, 41, 1697–1702.
Feld, G. K. (2007). Atrioventricular node modification and ablation for ventricular rate control in atrial fibrillation. Heart Rhythm, 4(3), S80–S83.
Williamson, B. D., Man, K. C., Daoud, E., Niebauer, M., Stirckberger, S. A., & Morady, F. (1995). Radiofrequency catheter modification of atrioventricular conduction to control the ventricular rate during atrial fibrillation. The New England Journal of Medicine, 332, 479.
Kindermann, M., Hennen, B., Jung, J., Geisel, G., Bohm, M., & Frohlig, G. (2006). Biventricular versus conventional right ventricular stimulation for patients with standard pacing indication and left ventricular dysfunction. The Homburg Biventricular Pacing Evaluation (HOBIPACE). Journal of the American College of Cardiology, 47, 1927–1937.
Doshi, R. N., Daoud, E. G., Fellows, C., Turk, K., Duran, A., Hamdan, M. H., et al. (2005). Left ventricular-based cardiac stimulation post AV nodal ablation evaluation (the PAVE Study). Journal of Cardiovascular Electrophysiology, 16, 1160–1165.
Steinhoff, J. P., & Sheahan, R. G. (2005). Tachycardia-induced cardiomyopathy: atrial fibrillation and congestive heart failure. The American Journal of the Medical Sciences, 329(1), 25–28.
Lee, S. H., Chen, S. A., Tai, C. T., Chiang, C. E., Wen, Z. C., Cheng, J. J., et al. (1998). Comparisons of quality of life and cardiac performance after complete atrioventricular junction ablation and atrioventricular junction modification in patients with medically refractory atrial fibrillation. Journal of the American College of Cardiology, 31, 637–644.
Issa, Z. F. (2007). An approach to “Ablate and Pace”: AV Junction ablation and pacemaker implantation performed concurrently from the same venous access site. Pacing and Clinical Electrophysiology, 30(9), 1116–1120.
Financial Disclosure
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kalaga, R., Kahr, R., Migeed, M. et al. Comparison of single and double vein approaches for His bundle ablation and pacemaker placement for symptomatic rapid atrial fibrillation. J Interv Card Electrophysiol 24, 113–117 (2009). https://doi.org/10.1007/s10840-008-9319-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-008-9319-x