
Abstract
Background: A complete line of block (CLOB) in the cavotricuspid isthmus (CTI) is the endpoint of typical atrial flutter ablation. Before CTI block is obtained, a progressive CTI conduction delay due to an incomplete line of block (InLOB) can be difficult to distinguish from CLOB. The purpose of this study was to assess a new simple approach based on the changes in atrio-ventricular (AV) conduction delays during septal and lateral right atrial pacing, to distinguish a CLOB from an InLOB during typical atrial flutter (AFL) ablation.
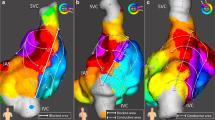
Methods and Results: Forty patients who presented an InLOB before a CLOB, and a stable (AV) conduction delay at 600 ms cycle length pacing (when in sinus rhythm), during AFL ablation were included in this study. A 24-pole mapping catheter was positioned so that 2 adjacent dipoles bracketed the targeted CTI line of block (LOB), with proximal dipoles lateral to the LOB and distal dipoles in the coronary sinus. Two pacing sites were lateral (position L1 and L2) and one was septal (position S) to the LOB, with locations L1 and S closest to the LOB. During L1, L2 and S site pacing, the delay between the pacing artefact and the peak of the R wave in a surface ECG (lead II) was measured.
We measured the following conduction delays (mean ± SD in ms), during InLOB versus CLOB: (L1 to R) 320.5 ± 68.0 versus 367.0 ± 62.0, p = 0.001; (L2 to R) 333.0 ± 59.0 versus 338.0 ± 62.0, p = 0.663, (S to R) 259.4 ± 51.5 versus 247.1 ± 55.5, p = 0.987. We calculated the following data during an InLOB versus a CLOB: (L1R–L2R) − 12.3 ± 7 versus 20.2 ± 12.7, p = 0.001; (L1R–SR) 51.1 ± 21.5 versus 120.1 ± 16.6, p < 0.05. The sensitivity, specificity, positive and negative predictive values for CLOB with (L1R-SR > 94 ms) and with (L1R-L2R > 0 ms) were respectively; 100%, 98%, 98% and 100%.
Conclusions: This study establishes that lateral versus septal right atrial pacing sites combined with the measure of AV conduction delay on a surface ECG can be useful to distinguish a CLOB from an InLOB during AFL ablation.
Similar content being viewed by others


References
Chen J, de Chillou C, Basiouny T, Sadoul N, Da Silva Filho J, Magnin-Poull I, Messier M, Aliot E. Cavotricuspid isthmus mapping to access bidirectional block during common atrial flutter radiofrequency ablation. Circulation 1999;100:2507–2513.
Shah D, Haíssaguerre M, Takahashi A, Jaís P, Hocini M, Clémenty J. Differential pacing for distinguishing block from persistent conduction through an ablation line. Circulation 2000;102:1517–1522.
Shah D, Haíssaguerre M, Jaís P, Fischer B, Takahashi A, Hocini M, Clementy J. Simplified electrophysiologically directed catheter ablation of recurrent common atrial flutter. Circulation 1997;96:2505–2508.
Tada H, Oral H, Sticherling C, Chough SP, Baker RL, Wasmer C, Pelosi F, Knight BP, Strickberger A, Morady F. Double potentials along the ablation line as a guide to radiofrequency ablation of typical atrial flutter. J Am Coll Cardiol. 2001; 38:750–755.
Anselme F, Savouré A, Cribier A, Saoudi N. Catheter ablation of typical atrial flutter, a randomized comparison of 2 methods for determining complete bidirectional isthmus block. Circulation 2000;103:1434–1439.
Kirkorian G, Moncada E, Chevalier P, Canu G, Claudel JP, Bellon C, Lyon L, Touboul P. Radiofrequency ablation of atrial flutter: efficacy of an anatomically guided approach. Circulation 1994;90:2804–2814.
Shah D, Haíssaguerre M, Jaís P, Takahashi A, Hocini M, Clementy J. High-density mapping of activation through an incomplete isthmus ablation line. Circulation 1999;99:211–215.
Chen J, de Chillou C, Hoff PI, Rossvoll O, Andronache M, Sadoul N, Magnin-Poull I, Erga S, Aliot E, Ohm OJ. Identification of extremely slow conduction in the cavotricuspid isthmus during common atrial flutter ablation. J Interv Card Electrophysiol 2002;7(1):67–75.
takahashi A, Shah DC, Jais P, Hocini M, Clementy J, Haissaguerre M. Partial cavotricuspid isthmus block before ablation in patients with typical aatrial flutter. J Am Coll Cardiol 1999;33(7):1996–2002.
Arenal A, Almendral J, Alday JM, Villacastin J, Ormaetxe JM, Sande JL, Perez-Castellano N, Gonzalez S, Ortiz M, Delcan JL. Rate-dependent conduction block of the crista terminalis in patients with typical atrial flutter. Influence on evaluation of cavotricuspid isthmus conduction block. Circulation 1999;99:2771–2778.
Tada H, Oral H, Ozaydin M, Chugh A, Sharf C, Hassan S, Greenstein R, Pelosi F, Knight BP, Strickberger SA, Morady F. Randomized comparison of anatomic and electrogram mapping approaches to ablation of typical atrial flutter. J Cardiovasc Electrophysiol 2002;13(7):662–666.
Tai CT, Haque A, Lin YK, Tsao HM, Ding YA, Chang MS, Chen SA. Double potential interval and transisthmus conduction time for prediction of cavotricuspid isthmus block after ablation of typical atrial flutter. J Interv Card Electropysiol 2002;7(11):77–82.
Andronache M, de Chillou C, Miljoen H, Magnin-Poull I, Messier M, Dotto P, Doan T, Houriezz P, Bineau-Jorisse A, Thiel B, Brembillat-Perrot B, Massin JL, Sadoul N, Aliot E. Correlation between electrogram morphology and standard criteria validate bi-directional cavotricuspid block in common atrial flutter ablation. Europace 2003;5(4):335–341.
Klug D, Lacroix D, Marquie C, Mairesse G, Alix D, Dennetiere S, d'Hautefeuille B, Zghal N and Kacet S. Prospective evaluation of a simplified approach for common atrial flutter radio-frequency ablation with only two catheters. Europace 2001;3(3):208–215.
Tada H, Nogami A, Naito S, Horie Y, Suguta M, Nakatsugawa M, Hoshizaki H, Taniguchi K. Quantitative analysis of surface P-Wave morphology in isthmus ablation for type 1 atrial flutter: differentiation between complete isthmus block and slow isthmus conduction. Jpn Circ J. 1999;63(4):244–248.
Shah DC, Takahashi A, Jais P, Hocini M, Peng JT, Clementy J, Haissaguerre M. Tracking dynamic conduction recovery across the cavotricuspid isthmus. J Am Coll Cardiol 2000;35(6):1478–1484.
Weiss C, Willems S, Hoffmann M, Meinert T. Impact of the ECG for the detection of intra-atrial conduction block after flutter ablation. Pacing Clin Electrophysiol 1999;22(10):1457–1465.
Mairesse GH, Lacroix D, Klug D, Le Franc P, Kouakam C, Kacet S. The usefulness of surface ECG 12-lead electrogram to predict intra-atrial conduction block after successful atrial flutter ablation. J Electrocardiol 2003;36(3):227–235.
Tai CT, Tsai CF, Hsieh MH, Lin WS, Lin YK, Lee SH, Yu WC, Ding YA, Chang MS, Chen SA. Effects of cavotricuspid isthmus on atrioventricular node electrophysiology in patients with typical atrial flutter. Circulation 2001;104:1501–1505.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Laurent, G., Bourcier, A., Bertaux, G. et al. A New and Simple Method for Distinguishing Complete from Incomplete Block Through the Cavotricuspid Isthmus. J Interv Card Electrophysiol 14, 175–182 (2005). https://doi.org/10.1007/s10840-006-6085-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-006-6085-5