
Abstract
The earliest case of Covid-19 was documented in Wuhan city of China and since then the virus has been spreading throughout the globe. The aim of this study is to evaluate the clusters of Covid-19 among the provinces in Turkey and to examine whether the clustering pattern has changed after the country’s lockdown strategy. The spatial dependence of Covid-19 in 81 provinces of Turkey was examined by spatial analysis between February 8 and June 28, 2021. Global and Local Moran's I and Gi* were employed to measure the global and local spatial autocorrelation degrees. The geographical distribution of Covid-19 in the provinces of Turkey showed a strong spatial autocorrelation while the spatial structure of the clusters varied by weeks. The findings of the study show that the complete lockdown carried out in Turkey has been quite effective in mitigating Covid-19. The importance of spatial relations in preventing the spread of the disease in Turkey has also been demonstrated in this context.
Similar content being viewed by others
Introduction
The novel coronavirus disease first appeared in Wuhan, China. As a result of the examination of a group of patients, the virus was diagnosed on January 13, 2020. While the fight against the first pandemic of the century continues, public health and national economies continue to suffer serious damage (Arauzo-Carod, 2021). Different measures have been implemented by most countries to fight against the coronavirus. People have been locked down in cities, production has stopped, schools have been closed, and restrictions have been imposed on people's movements. While the pandemic has been threatening people’s health and causing loss of lives, an economic downturn began to emerge on the other hand. In fact, as highlighted by the United Nations, the Covid-19 pandemic means much more than a medical crisis; it is an economic, a social and a human crisis (UN, 2020). During this pandemic, the main concern for each nation is to keep their populations healthy. However, the disease also had an impact on national economies. Hence, during this unusual and challenging time of Covid-19, every country has to deal with two major issues: Healthcare and economics (Sharma et al., 2021). Undetected spread of the virus shocked governments, scientists and international organizations. In addition to its impact on public health, it caused major economic distress. Therefore, these changes will cause a long-run international economic downturn. As we mention in this paper, health systems of most countries haven’t been able to contain the evolution and the persistence of the virus (Kalla et al., 2021).
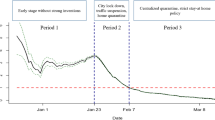
The whole world is fighting this pandemic, which shows the highest number of daily cases around the globe and losses of the last century, while the numbers affected by the pandemic differ by countries. For example, as a country with high population density, Turkey has experienced high percentages of incidence and fatality. Additionally, new cases and deaths related to Covid-19 increase Daily. The first news of death from Turkey came on March 17, 2020 (T.C.S.B, 2021). More than forty-nine thousand citizens of the Republic of Turkey died since the day Turkey met with the first Covid-19 case. In the face of the daily increase in registered cases in Turkey, the government and the public authorities took a wide range of measures that included the entire country at the end of April, and a complete lockdown was implemented in Turkey from April 29, 2021 until May 17, 2021. In this research, we aim to investigate the spatial distribution of the virus and the effect of complete lockdown measures on the spatial structure of the clusters.
Review of the literature
After the break of coronavirus, studies have used statistical methods to determine the nexus between cases, the factors of transmission and the determination of clusters (Appiah-Otoo & Kursah, 2021). As the characteristics of Covid-19 are original and wild, it spread very quickly. Therefore, The World Health Organizaton has consistently used spatial data analysis to control infectious diseases (Esri, 2020; Nasiri et al., 2021). Within the scope of the research of measures that can be taken to prevent the pandemic, many researchers in different countries have revealed the effects of spatial factors on the fast spread of coronavirus (Adegboye et al., 2021; Casado-Aranda et al., 2021; Castro et al., 2021; Gupta et al., 2021; Li et al., 2021; Liu et al., 2021; Maiti et al., 2021; Mansour et al., 2021; Nasiri et al., 2021; Rubino et al., 2020; Sarkar et al., 2021; Shariati et al., 2020; Tang et al., 2020; Tao et al., 2020; Vaz, 2021; Xiong et al., 2020). Ramírez-Aldana et al. (2020) determined that the number of Covid-19 cases in Iranian provinces is spatially related. Similarly Arauzo-Carod (2021) showed that in Catalonia (Spain), positive case numbers were associated with nearby settlements, through spatial autocorrelation. Eryando et al. (2020) stated that Covid-19 was not observed randomly in Indonesia, but that the neighboring provinces that were connected and five other cities with the highest number of cases were adjacent to each other. Ghosh and Cartone (2020) determined the spatial impact of the virus that emerged in different regions of Italy. Again, researchers similarly highlighted the importance of spatial relation in the spread and prevention of the epidemic in Oman (Al-Kindi et al., 2020), Kuwait (Alkhamis et al., 2020), South Korea (Kim & Castro, 2020), Iran (Pourghasemi et al., 2020), China (Kang et al., 2020), Lebanon (El Deeb, 2021), and Rio de Janeiro (Ferreira et al., 2020). In these studies, which take place in literature, the importance of spatial heterogeneity has been underlined and it has been determined that local characteristics affect the spread of coronavirus. The efficiency of health policies has been associated with coordination at both local and national levels. Geographical information about the pandemic helps to ensure coordination at national and local levels. It has been stated that maintaining health standards, preventing social tension and achieving fewer work interruptions can be accomplished this way (Ghosh & Cartone, 2020).
In the light of this information, the goal of this research is to survey the clusters of the pandemic among the provinces of Turkey and to examine whether the clustering structure has changed after the country’s lockdown strategy. The course of the change in Covid-19 cases in Turkey during the period of study by provinces can also be examined in the timeline. Selected accordingly, the period of study offers the scope to examine the spatial distribution of Covid-19 in Turkey's provinces in a comparative way including the complete lockdown period and the previous period.
Methodology
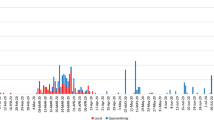
Data showing the number of coronavirus cases by province, corresponding to a weekly population of 100,000 began to be published as of February 15, 2021 in Turkey. The study uses the number of cases by province corresponding to a population of 100,000 for 20 weeks (8 February–28 June). The summary of the characteristics of the research variables are presented in Table 1. The number of coronavirus cases, which increased within weeks during the period of this study, reached its peak in the 11th week and then started to decline.
If the empirical study is developed on spatial data, or if the relations studied are “spatial” in nature, it becomes essential to use spatial analysis that can “appropriately” incorporate location and spatial arrangement into the study (Anselin, 1999). In this context, spatial autocorrelation was employed to examine whether Covid-19 has noteworthy global or local spatial autocorrelation features (Xiong et al., 2020). Global or local measures of spatial autocorrelation have been used to investigate the spatial patterns and define hot spots and cold spots of the epidemic in many researches (Alves et al., 2021; Castro et al., 2021; Das et al., 2021; Ghosh & Cartone, 2020; Islam et al., 2021; Kuznetsov & Sadovskaya, 2021; Maithani et al., 2020; Maroko et al., 2020). Spatial statistical methods have also been employed in previous years to comprehend spatial patterns of epidemic risks (Bailey, 2001; Bailey et al., 2011; Cao et al., 2010; Cromley, 2003; Ge et al., 2016; Hu et al., 2013; Tsai et al., 2009; Wang et al., 2008; Wen et al., 2006).
Spatial autocorrelation, a concept that is of use in defining the field of spatial analysis, is at the center of studies using spatial statistics (Getis, 2008; Ord & Getis, 2001). Spatial autocorrelation measurements and tests are divided into local and global scales depending on the scale and scope of the analysis (Anselin, 1995).
The Moran’s I statistic was employed to determine the global spatial autocorrelation characteristics of Covid-19 (Anselin, 1988; Moran, 1948, 1950):
Similar to the correlation coefficient, Moran's I score varies in the range of [− 1 + 1]. (Anselin, 1996; Griffith, 2003).
Local spatial autocorrelation was used to determine local spatial autocorrelation features of the coronavirus.
The Local Moran’s I statistic is calculated as follows (Anselin, 1995):
Similar to Moran's I, the G test is another sign of local spatial autocorrelation. In this test proposed by Getis and Ord (1992) and then further detailed in Ord and Getis (1995), values near − 1 indicate clustering of similar values. Values near 1 indicate divergence (i.e., random models), which means that this test is inversely linked with Moran's I test. G is calculated as follows (Getis & Aldstadt, 2004; Getis & Ord, 2010):
With the G test, four values are obtained. First, the p-value is examined. If the obtained p-value is found to be statistically small and significant, it indicates that the observation values are clustered spatially, otherwise, the observation values are randomly distributed. If the p-value suggests a cluster, look at the z-score. If the z-score is positive, it indicates that high values of the observation values tend to cluster in the analyzed area. Otherwise, if the z-score is found to be negative, it indicates that low observation values tend to cluster (Getis & Ord, 2010).
The Getis-Ord Gi ∗ is another primarily used test to measure local spatial autocorrelation. The Gi ∗ statistic has been calculated to define hot spots and cold spots of coronavirus. Gi ∗ is calculated as follows:
Here;
Gi ∗ , similar to the G test, yields two measures, the z-score and the p-value. The resulting z-score reports where locations with high or low observations show a tendency to cluster in space. Unlike Local Moran’s and Local Geary statistics, the Getis-Ord method does not consider spatial outliers (Anselin, 1995, 2019; Getis & Ord, 1992, 1996; Ord & Getis, 1995).
Results and discussion
In the study, Moran’s I coefficients were calculated first in order to analyze the relationship between Covid-19 cases in any province and Covid-19 cases in neighboring provinces. Spatial autocorrelation indicates whether Covid-19 numbers are associated with close locations. Accordingly, it is observed that the spatial autocorrelation of Covid-19 cases is positive across the country. Moran’s I values for Covid-19 were recorded in the range of 0.257387–0.674243, confirming the presence of spatial structure. While Moran’s I statistics tended to increase in the period under consideration, it reached its highest value in the 12th week. As of the 13th week (during the complete lockdown period), it started to trend downwards, but the spatial correlation was still in clustering characteristic. At the 17th week, Moran’s I values started to rise again (Table 1).
Figure 1 shows the results of cluster analysis of provinces in Turkey, which is created to examine whether the observation values show regionally significant spatial clustering or scattering. According to LISA, LL clusters are observed in eastern and southeastern provinces in all periods. In these regions, the patterns of LL clusters tend to have a continuous distribution. While the main clusters of HH were frequently seen in the northern regions in the first 4 weeks, they started to appear in the west from the 5th week and intensified over time. While the clustering trend was similar in the 7th, 8th and 9th weeks, the northern clustering disappeared at the 10th week. As of the complete lockdown (13th week), the pattern of the distribution started to differ. The number of significant clusters observed in the 16th week decreased considerably and started to rise again from the 17th week. While the clusters of cases seen by weeks tend to rise and rapidly spread over other regions, they tend to decrease during the complete lockdown period. Within this framework, it is possible to see that the effect of the measures taken during this period is positive.


Source: Author
Regional level spatial clustering of Covid-19 for 20 weeks and entire period in Turkey.
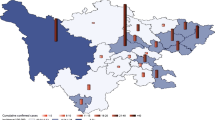
The Gi* statistic has been calculated to identify the clusters of Covid-19 (hot and cold spots). The Gi* utilizes the data of each province infected by Covid-19 and analyzes the local situation, comparing it with the global situation in the neighboring provinces (Bhunia et al., 2021). Figure 2 shows the prevalence of Covid-19 coded by Gi* statistics based on selected weekly data from March 8 to June 28, 2021. Accordingly, it is possible to detect the hot and cold spot regions of Covid-19. In this context, clusters of cold spots and hot spots were detected over the weeks in Turkey with a confidence level of 95%.


Source: Author
Clustering of Covid-19 for 20 weeks and entire period in Turkey.
According to the results of the hot spot analysis, 8 cities turn up hot spots in the first week. While the distribution of hot spots in this region was similar for 4 weeks, Çanakkale province, located in the Marmara region, was included in the hot spots in the 5th week. It spread to Tekirdağ and Kırklareli in the 6th week, and was observed in Edirne, Yalova, Istanbul, Bursa and Kocaeli in the 7th week. Hot spots rapidly covered most of the cities, and these provinces have become important hot spots. From the 11th week, it has spread to neighboring provinces. In the 16th week, the number of hot spots decreased, and it started to rise again from the 17th week.
Again, in this context, the positive effect of complete lockdown is seen. Researchers in different countries have revealed the effects of lockdowns in reducing the spread of Covid-19 (Acter et al., 2020; Alcântara et al., 2020; Bourdin et al., 2021; Cheng et al., 2020; Kraemer et al., 2020; Saha et al., 2021). Therefore, the importance of spatial measures in preventing the spread of the pandemic emerges. Thanks to these measures, both the cost of lockdown will decrease, and the spread of Covid-19 can also be prevented more quickly. Thus, the public reaction against lockdowns will also ease, relieving public administrators as well.
Conclusion and policy recommendations
In Turkey, the first case of coronavirus was diagnosed on March 11, 2020, and during the past year, the number of cases has exceeded five million, while the number of deaths has exceeded forty-nine thousand. On the other hand, different numbers of cases at the provincial level brought up the examination of the geographical distribution of Covid-19. In this context, the necessity of using spatial statistics has emerged. Thus, the efficiency of local decisions will increase and it will be possible to fight against the pandemic more strongly. In this direction, with the help of spatial statistics, this study aims to examine the spatial distribution of the virus and to investigate the effect of complete lockdown measures on the spatial model of the clusters. As a result of the analyses made in this framework, a positive spatial autocorrelation has been determined in Turkey. The relationship between provinces was measured and the spatial clustering of Covid-19 was determined. These findings revealed the significant effects of the infection spreading among provinces. This reveals the importance of geographical location in the fight against the pandemic. Identifying hot spot Covid-19 areas may be beneficial in supervising regional Covid-19 prevention programs (Bhunia et al., 2021). In the light of the results obtained, it is important for policy makers to take measures to prevent the spread of the pandemic for provinces with hot spots because these cities are the riskiest in terms of the virus spreading, while these provinces also have more spatial interactions with their neighbors. Therefore, measures should be highlighted and control should be strengthened in cities with hot spots and their neighbors (Zeren & Yilanci, 2020).
However, with the complete lockdown period, it was determined that the spatial clusters of Covid-19 decreased and the spatial relations between the provinces weakened. The spatial relations observed at the local level will enable decision makers to produce more successful solutions in reply to the pandemic. The spread of the pandemic can be prevented by taking measures for the provinces where the said relations are observed. Therefore, measures taken specifically in provinces with high risk will both prevent the spread of the virus and will have a lower economic cost compared to a nationwide lockdown.
This research, which tries to reveal the spatial relationships of Covid-19, has some limitations. One of the limitations in question is that the data set does not include the number of cases and deaths. For this reason, the spatiotemporal spread pattern of Covid-19 could not be examined by using the number of deaths. Also, since the data began to be published as of February 2021, the spatiotemporal characteristics of the epidemic could not be examined for the whole process. In addition, since the data obtained are related to the provinces, analyzes at lower levels could not be performed. In future studies, when the data is available, more detailed results can be obtained by using the number of deaths, analyzing at the district level or by separating rural and urban areas. It is thought that these analyzes will be beneficial in preventing the spread of the epidemic.
References
Acter, T., Uddin, N., Das, J., Akhter, A., Choudhury, T. R., & Kim, S. (2020). Evolution of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) as coronavirus disease 2019 (COVID-19) pandemic: A global health emergency. Science of the Total Environment, 730, 138996. https://doi.org/10.1016/j.scitotenv.2020.138996
Adegboye, O. A., Adekunle, A. I., Pak, A., Gayawan, E., Leung, D. H., Rojas, D. P., Elfaki, F., McBryde, E. S., & Eisen, D. P. (2021). Change in outbreak epicentre and its impact on the importation risks of COVID-19 progression: A modelling study. Travel Medicine and Infectious Disease, 40(January), 101988. https://doi.org/10.1016/j.tmaid.2021.101988
Al-Kindi, K. M., Alkharusi, A., Alshukaili, D., Al Nasiri, N., Al-Awadhi, T., Charabi, Y., & El Kenawy, A. M. (2020). Spatiotemporal assessment of Covid-19 spread over Oman using GIS techniques. Earth Systems and Environment, 4(4), 797–811. https://doi.org/10.1007/s41748-020-00194-2
Alcântara, E., Mantovani, J., Rotta, L., Park, E., Rodrigues, T., Carvalho, F. C., & Filho, C. R. S. (2020). Investigating spatiotemporal patterns of the covid-19 in São Paulo state, Brazil. Geospatial Health, 15(2), 201–209. https://doi.org/10.4081/gh.2020.925
Alkhamis, M. A., Al Youha, S., Khajah, M. M., Ben Haider, N., Alhardan, S., Nabeel, A., Al Mazeedi, S., & Al-Sabah, S. K. (2020). Spatiotemporal dynamics of the COVID-19 pandemic in the State of Kuwait. International Journal of Infectious Diseases, 98, 153–160. https://doi.org/10.1016/j.ijid.2020.06.078
Alves, J. D., Abade, A. S., Peres, W. P., Borges, J. E., Santos, S. M., & Scholze, A. R. (2021). Impact of COVID-19 on the indigenous population of Brazil: A geo-epidemiological study. Epidemiology and Infection, 149(e185), 1–11. https://doi.org/10.1017/S0950268821001849
Anselin, L. (1988). Spatial econometrics: Methods and models. Kluwer Academic Publishers.
Anselin, L. (1995). Local ındicators of spatial association—LISA. In Geographical analysis (vol. 27, Issue 2). https://doi.org/10.1111/j.1538-4632.1995.tb00338.x
Anselin, L. (1996). The Moran scatter plot as an ESDA tool to assess local instability in spatial association. In H. J. Fischer & M. M. Scholten (Eds.), Spatial analytical perspectives on GIS: GISDATA (4th ed., pp. 111–125). New York: CRC Press.
Anselin, L. (1999). The future of spatial analysis in the social sciences. Annals of GIS, 5(2), 67–76. https://doi.org/10.1080/10824009909480516
Anselin, L. (2019). A local indicator of multivariate spatial association: Extending Geary’s c. Geographical Analysis, 51(2), 133–150. https://doi.org/10.1111/gean.12164
Appiah-Otoo, I., & Kursah, M. B. (2021). Modelling spatial variations of novel coronavirus disease (COVID-19): Evidence from a global perspective. GeoJournal. https://doi.org/10.1007/s10708-021-10427-0
Arauzo-Carod, J. M. (2021). A first insight about spatial dimension of COVID-19: Analysis at municipality level. Journal of Public Health (oxford, England), 43(1), 98–106. https://doi.org/10.1093/pubmed/fdaa140
Bailey, P. E., Keyes, E. B., Parker, C., Abdullah, M., Kebede, H., & Freedman, L. (2011). Using a GIS to model interventions to strengthen the emergency referral system for maternal and newborn health in Ethiopia. International Journal of Gynecology and Obstetrics, 115(3), 300–309. https://doi.org/10.1016/j.ijgo.2011.09.004
Bailey, T. C. (2001). Spatial statistical methods in health. Cadernos De Saúde Pública, 17(5), 1083–1098. https://doi.org/10.1590/S0102-311X2001000500011
Bhunia, G. S., Roy, S., & Shit, P. K. (2021). Spatio-temporal analysis of COVID-19 in India: a geostatistical approach. Spatial Information Research, 29(5), 661–672. https://doi.org/10.1007/s41324-020-00376-0
Bourdin, S., Jeanne, L., Nadou, F., & Noiret, G. (2021). Does lockdown work? A spatial analysis of the spread and concentration of Covid-19 in Italy. Regional Studies, 55(7), 1182–1193. https://doi.org/10.1080/00343404.2021.1887471
Cao, Z. D., Zeng, D. J., Zheng, X. L., Wang, Q. Y., Wang, F. Y., Wang, J. F., & Wang, X. L. (2010). Spatio-temporal evolution of Beijing 2003 SARS epidemic. Science China Earth Sciences, 53(7), 1017–1028. https://doi.org/10.1007/s11430-010-0043-x
Casado-Aranda, L.-A., Sánchez-Fernández, J., & Bastidas-Manzano, A.-B. (2021). Tourism research after the COVID-19 outbreak: Insights for more sustainable, local and smart cities. Sustainable Cities and Society, 73, 103126. https://doi.org/10.1016/j.scs.2021.103126
Castro, R. R., Santos, R. S. C., Sousa, G. J. B., Pinheiro, Y. T., Martins, I. M., Pereira, M. L. D., & Silva, R. A. R. (2021). Spatial dynamics of the COVID-19 pandemic in Brazil. Epidemiology and Infection, 149(e60), 1–9. https://doi.org/10.1017/S0950268821000479
Cheng, C., Zhang, T., Song, C., Shen, S., Jiang, Y., & Zhang, X. (2020). The coupled impact of emergency responses and population flows on the COVID-19 pandemic in China. GeoHealth, 4(12), e2020GH000332. https://doi.org/10.1029/2020GH000332
Cromley, E. K. (2003). GIS and disease. Annual Review of Public Health, 24, 7–24. https://doi.org/10.1146/annurev.publhealth.24.012902.141019
Das, A., Ghosh, S., Das, K., Basu, T., Dutta, I., & Das, M. (2021). Living environment matters: Unravelling the spatial clustering of COVID-19 hotspots in Kolkata megacity, India. Sustainable Cities and Society, 65, 102577. https://doi.org/10.1016/j.scs.2020.102577
El Deeb, O. (2021). Spatial autocorrelation and the dynamics of the mean center of Covid-19 infections in Lebanon. Frontiers in Applied Mathematics and Statistics, 6, 1–15. https://doi.org/10.3389/fams.2020.620064
Eryando, T., Sipahutar, T., & Rahardiantoro, S. (2020). The risk distribution of Covid-19 in Indonesia: A spatial analysis. Asia-Pacific Journal of Public Health, 32(8), 450–452. https://doi.org/10.1177/1010539520962940
Esri. (2020). Mapping epidemics: From SARS, Zika, and Ebola to the pandemic of COVID-19. https://www.esri.com/about/newsroom/blog/maps-that-mitigate-epidemics/
Ferreira, D., Ferreira, P., Oliveira, P., Ribeiro, J., Goncalves, E., & Papa, A. (2020). Temporal and spatial characteristics of the spread of COVID-19 in Rio de Janeiro state and city. MedRxiv. https://doi.org/10.1101/2020.05.13.20101113
Ge, L., Zhao, Y., Zhou, K., Mu, X., Yu, H., Wang, Y., Wang, N., Fan, H., Guo, L., & Huo, X. (2016). Spatio-temporal pattern and influencing factors of Hemorrhagic Fever with Renal Syndrome (HFRS) in Hubei province (China) between 2005 and 2014. PLoS ONE, 11(12), e0167836. https://doi.org/10.1371/journal.pone.0167836
Getis, A., & Ord, J. K. (1996). Local spatial statistics: an overview. In P. Longley & M. Batty (Eds.), Spatial analysis modelling in a GIS environment (pp. 269–285). Wiley.
Getis, A. (2008). A history of the concept of spatial autocorrelation: A geographer’s perspective. Geographical Analysis, 40(3), 297–309. https://doi.org/10.1111/j.1538-4632.2008.00727.x
Getis, A., & Aldstadt, J. (2004). Constructing the spatial weights matrix using a local statistic. Geographical Analysis, 36(2), 90–104. https://doi.org/10.1111/j.1538-4632.2004.tb01127.x
Getis, A., & Ord, J. K. (1992). The analysis of spatial association by use of distance statistics. Geographical Analysis, 24(3), 189–206. https://doi.org/10.1111/j.1538-4632.1992.tb00261.x
Getis, A., & Ord, J. K. (2010). The analysis of spatial association by use of distance statistics. In L. Anselin & S. J. Rey (Eds.), Springer. Springer.
Ghosh, P., & Cartone, A. (2020). A Spatio-temporal analysis of COVID-19 outbreak in Italy. Regional Science Policy and Practice, 12(6), 1047–1062. https://doi.org/10.1111/rsp3.12376
Griffith, D. (2003). Spatial autocorrelation and spatial filtering: Gaining understanding through theory and scientific visualization. Springer Science & Business Media.
Gupta, D., Biswas, D., & Kabiraj, P. (2021). COVID-19 outbreak and Urban dynamics: Regional variations in India. GeoJournal. https://doi.org/10.1007/s10708-021-10394-6
Hu, B., Gong, J., Zhou, J., Sun, J., Yang, L., Xia, Y., & Ibrahim, A. N. (2013). Spatial-temporal characteristics of epidemic spread in-out flow—Using SARS epidemic in Beijing as a case study. Science China Earth Sciences, 56(8), 1380–1397. https://doi.org/10.1007/s11430-012-4479-z
Islam, M. S., Tusher, T. R., Roy, S., & Rahman, M. (2021). Impacts of nationwide lockdown due to COVID-19 outbreak on air quality in Bangladesh: A spatiotemporal analysis. Air Quality, Atmosphere and Health, 14(3), 351–363. https://doi.org/10.1007/s11869-020-00940-5
Kalla, M. I., Lahmar, B., Geullouh, S., & Kalla, M. (2021). Health geo-governance to assess the vulnerability of Batna, Algeria to COVID-19: The role of GIS in the fight against a pandemic. GeoJournal. https://doi.org/10.1007/s10708-021-10449-8
Kang, D., Choi, H., Kim, J. H., & Choi, J. (2020). Spatial epidemic dynamics of the COVID-19 outbreak in China. International Journal of Infectious Diseases, 94, 96–102. https://doi.org/10.1016/j.ijid.2020.03.076
Kim, S., & Castro, M. C. (2020). Spatiotemporal pattern of COVID-19 and government response in South Korea (as of May 31, 2020). International Journal of Infectious Diseases, 98, 328–333. https://doi.org/10.1016/j.ijid.2020.07.004
Kraemer, M. U. G., Yang, C.-H., Gutierrez, B., Wu, C.-H., Klein, B., Pigott, D. M., du Plessis, L., Faria, N. R., Li, R., Hanage, W. P., Brownstein, J. S., Layan, M., Vespignani, A., Tian, H., Dye, C., Pybus, O. G., & Scarpino, S. V. (2020). The effect of human mobility and control measures on the COVID-19 epidemic in China. Science, 368(6490), 493–497. https://doi.org/10.1126/science.abb4218
Kuznetsov, A., & Sadovskaya, V. (2021). Spatial variation and hotspot detection of COVID-19 cases in Kazakhstan, 2020. Spatial and Spatio-Temporal Epidemiology, 39, 100430. https://doi.org/10.1016/j.sste.2021.100430
Li, B., Peng, Y., He, H., Wang, M., & Feng, T. (2021). Built environment and early infection of COVID-19 in urban districts: A case study of Huangzhou. Sustainable Cities and Society, 66, 102685. https://doi.org/10.1016/j.scs.2020.102685
Liu, Y., Pei, T., Song, C., Chen, J., Chen, X., Huang, Q., Wang, X., Shu, H., Wang, X., Guo, S., & Zhou, C. (2021). How did human dwelling and working intensity change over different stages of COVID-19 in Beijing? Sustainable Cities and Society, 74, 103206. https://doi.org/10.1016/j.scs.2021.103206
Maithani, S., Nautiyal, G., & Sharma, A. (2020). Investigating the effect of lockdown during COVID-19 on land surface temperature: study of Dehradun City, India. Journal of the Indian Society of Remote Sensing, 48(9), 1297–1311. https://doi.org/10.1007/s12524-020-01157-w
Maiti, A., Zhang, Q., Sannigrahi, S., Pramanik, S., Chakraborti, S., Cerda, A., & Pilla, F. (2021). Exploring spatiotemporal effects of the driving factors on COVID-19 incidences in the contiguous United States. Sustainable Cities and Society, 68, 102784. https://doi.org/10.1016/j.scs.2021.102784
Mansour, S., Al Kindi, A., Al-Said, A., Al-Said, A., & Atkinson, P. (2021). Sociodemographic determinants of COVID-19 incidence rates in Oman: Geospatial modelling using multiscale geographically weighted regression (MGWR). Sustainable Cities and Society, 65, 102627. https://doi.org/10.1016/j.scs.2020.102627
Maroko, A. R., Nash, D., & Pavilonis, B. T. (2020). COVID-19 and inequity: A comparative spatial analysis of New York City and Chicago hot spots. Journal of Urban Health, 97(4), 461–470. https://doi.org/10.1007/s11524-020-00468-0
Moran, P. A. P. (1948). The interpretation of statistical maps. Journal of the Royal Statistical Society: Series B (methodological), 10(2), 243–251. https://doi.org/10.1111/j.2517-6161.1948.tb00012.x
Moran, P. A. P. (1950). Notes on continuous stochastic phenomena. Biometrika, 37(1/2), 17–23. https://doi.org/10.2307/2332142
Nasiri, R., Akbarpour, S., Zali, A., Khodakarami, N., Boochani, M., Noory, A., & Soori, H. (2021). Spatio-temporal analysis of COVID-19 incidence rate using GIS: a case study—Tehran metropolitan, Iran. GeoJournal. https://doi.org/10.1007/s10708-021-10438-x
Ord, J. K., & Getis, A. (1995). Local Spatial Autocorrelation Statistics: Distributional Issues and an Application. Geographical Analysis, 27(4), 286–306. https://doi.org/10.1111/j.1538-4632.1995.tb00912.x
Ord, J. K., & Getis, A. (2001). Testing for local spatial autocorrelation in the presence of global autocorrelation. Journal of Regional Science, 41(3), 411–432. https://doi.org/10.1111/0022-4146.00224
Pourghasemi, H. R., Pouyan, S., Heidari, B., Farajzadeh, Z., Fallah Shamsi, S. R., Babaei, S., Khosravi, R., Etemadi, M., Ghanbarian, G., Farhadi, A., Safaeian, R., Heidari, Z., Tarazkar, M. H., Tiefenbacher, J. P., Azmi, A., & Sadeghian, F. (2020). Spatial modeling, risk mapping, change detection, and outbreak trend analysis of coronavirus (COVID-19) in Iran (days between February 19 and June 14, 2020). International Journal of Infectious Diseases, 98, 90–108. https://doi.org/10.1016/j.ijid.2020.06.058
Ramírez-Aldana, R., Gomez-Verjan, J. C., Bello-Chavolla, O. Y., & Peterson, T. (2020). Spatial analysis of COVID-19 spread in Iran: Insights into geographical and structural transmission determinants at a province level. PLoS Neglected Tropical Diseases, 14(11), e0008875. https://doi.org/10.1371/journal.pntd.0008875
Rubino, I., Coscia, C., & Curto, R. (2020). Identifying spatial relationships between built heritage resources and short-term rentals before the Covid-19 pandemic: Exploratory perspectives on sustainability issues. Sustainability, 12(11), 4533. https://doi.org/10.3390/su12114533
Saha, J., Mondal, S., & Chouhan, P. (2021). Spatial-temporal variations in community mobility during lockdown, unlock, and the second wave of COVID-19 in India: A data-based analysis using Google’s community mobility reports. Spatial and Spatio-Temporal Epidemiology, 39, 100442. https://doi.org/10.1016/j.sste.2021.100442
Sarkar, S. K., Ekram, K. M. M., & Das, P. C. (2021). Spatial modeling of COVID-19 transmission in Bangladesh. Spatial Information Research. https://doi.org/10.1007/s41324-021-00387-5
Shariati, M., Mesgari, T., Kasraee, M., & Jahangiri-rad, M. (2020). Spatiotemporal analysis and hotspots detection of COVID-19 using geographic information system (March and April, 2020). Journal of Environmental Health Science and Engineering, 18(2), 1499–1507. https://doi.org/10.1007/s40201-020-00565-x
Sharma, N., Yadav, S., Mangla, M., Mohanty, A., Satpathy, S., Mohanty, S. N., & Choudhury, T. (2021). Geospatial multivariate analysis of COVID-19: A global perspective. GeoJournal. https://doi.org/10.1007/s10708-021-10520-4
T.C.S.B. (2021). T.C. Sağlık Bakanlığı.
Tang, W., Liao, H., Marley, G., Wang, Z., Cheng, W., Wu, D., & Yu, R. (2020). The changing patterns of coronavirus disease 2019 (COVID-19) in China: A tempogeographic analysis of the severe acute respiratory syndrome coronavirus 2 epidemic. Clinical Infectious Diseases, 71(15), 818–824. https://doi.org/10.1093/cid/ciaa423
Tao, R., Downs, J., Beckie, T. M., Chen, Y., & McNelley, W. (2020). Examining spatial accessibility to COVID-19 testing sites in Florida. Annals of GIS, 26(4), 319–327. https://doi.org/10.1080/19475683.2020.1833365
Tsai, P.-J., Lin, M.-L., Chu, C.-M., & Perng, C.-H. (2009). Spatial autocorrelation analysis of health care hotspots in Taiwan in 2006. BMC Public Health, 9(1), 464. https://doi.org/10.1186/1471-2458-9-464
UN. (2020). United Nations. https://www.un.org/en/
Vaz, E. (2021). Covid-19 in Toronto: A spatial exploratory analysis. Sustainability (switzerland), 13(2), 498. https://doi.org/10.3390/su13020498
Wang, J. F., Christakos, G., Han, W. G., & Meng, B. (2008). Data-driven exploration of “spatial pattern-time process-driving forces” associations of SARS epidemic in Beijing, China. Journal of Public Health, 30(3), 234–244. https://doi.org/10.1093/pubmed/fdn023
Wen, T.-H., Lin, N. H., Lin, C.-H., King, C.-C., & Su, M.-D. (2006). Spatial mapping of temporal risk characteristics to improve environmental health risk identification: A case study of a dengue epidemic in Taiwan. Science of the Total Environment, 367(2–3), 631–640. https://doi.org/10.1016/j.scitotenv.2006.02.009
Xiong, Y., Wang, Y., Chen, F., & Zhu, M. (2020). Spatial statistics and influencing factors of the COVID-19 epidemic at both prefecture and county levels in Hubei Province, China. International Journal of Environmental Research and Public Health, 17(11), 3903. https://doi.org/10.3390/ijerph17113903
Zeren, F., & Yilanci, V. (2020). Analysing spatial patterns of the Covid-19 outbreak in Turkey. Bingöl Üniversitesi İktisadi Ve İdari Bilimler Fakültesi Dergisi, 4(2), 27–40.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Aral, N., Bakır, H. Spatiotemporal pattern of Covid-19 outbreak in Turkey. GeoJournal 88, 1305–1316 (2023). https://doi.org/10.1007/s10708-022-10666-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10708-022-10666-9