
Abstract
While hotspots of alcohol-related incidents have been associated with alcohol outlet density, few studies have considered other environmental factors. We aimed to characterise the environment of hotspots outside of outlet density areas in Amsterdam. Using geographical information systems, we identified hotspots of alcohol-related health incidents outside of outlet density areas based on the registry of alcohol related ambulance attendances. While quantitative data and methods were used to analyse victim profiles (including age, sex and home address) and temporal profiles (time of incident), we combined quantitative and qualitative information to develop environmental profiles of these hotspots. We identified 11 hotspots with 242 incidents outside outlet density areas. Results indicate substantial differences between incidents in these hotspots and incidents in high outlet density areas. Victims in these hotspots are older, more often male and live closer to the incident location compared to victims in high outlet density hotspots. Incidents are less likely to take place during the night and at weekends. In-depth analysis of four hotspots showed different combinations of contributing environmental factors, including (a) public parks bordering deprived neighbourhoods, (b) dance event facilities close to a traffic black spot, and (c) residential services for disadvantaged groups near ‘hang-outs’. The study shows that hotspots of alcohol-related incidents can arise outside outlet density areas at locations where several other environmental factors cluster, particularly in more deprived areas. Such hotspots can be addressed in urban planning and urban design.
Similar content being viewed by others
Introduction
Alcohol-related harm is a public health issue of critical importance. In 2011, 2732 alcohol-related incidents were registered by the ambulance service in Amsterdam, The Netherlands. In that year, Amsterdam counted 780,559 inhabitants. The number of incidents involving people under the age of 25 almost tripled between 2001 and 2011, going from 216 to 609 incidents (Ujcic-Voortman et al. 2013). Because the prevention of alcohol-related harm would have great public health and societal benefits, a large body of research has attempted to reveal determinants of hazardous alcohol use and alcohol-related harm such as injuries and poisoning.
A voluminous ‘alcohol studies’ literature exists across both social and medical sciences. Relevant studies examine diverse issues such as the relationship between drinking and gender, class, ethnicity and differences in drinking practices across countries, between regions and within cities. Important contributions to alcohol-related research were made by geographers (Jayne et al. 2008).
Researchers within the field of public health and health geography have increasingly turned their attention towards the environmental determinants of hazardous alcohol use (see, for example Bernstein et al. 2007; Karriker-Jaffe 2011; Robert 1999; Romley et al. 2007). The focus of most of these studies has been on the social and socio-economic characteristics of the residential environment, or on the functional characteristics of locations where hazardous use of alcohol is common. Ecologic theories, such as routine activity theories and social disorganisation theories, are frequently used to understand the processes and mechanisms linking environmental characteristics to the spatial clustering of alcohol-related problems (Gorman et al. 2013).
With regard to the residential environment, associations between neighbourhood socio-economic status and alcohol use were found, though the direction thereof varied between studies. Some studies have suggested that heavy drinking is more prevalent in deprived areas, possibly because of lower levels of social control over deviant behaviours and drinking being used by residents as a coping mechanism to feel less miserable and stressed (Elliott 2000; Galea et al. 2007; Halonen et al. 2012; Stimpson et al. 2007; Cerda et al. 2010). Social disorganisation theory hypothesizes that in deprived neighbourhoods social networks among residents are disrupted resulting in reduced informal social control and low collective efficacy (Quick et al. 2016). Other studies have observed high levels of alcohol consumption in affluent neighbourhoods where drinking may be part of a privileged lifestyle focused on pleasure and comfort (Pollack et al. 2005). Other studies have not found any significant association (Cornaz et al. 2009; Ecob and Macintyre 2000). For the Netherlands, Kuipers et al. (2013) found a lower prevalence of heavy alcohol consumption in deprived areas. This was partially explained by the presence of a large immigrant population with an Islamic background, which is traditionally associated with little or no alcohol consumption.
Other studies have adopted a micro spatial approach and have turned their attention towards the identification of spatial patterns of alcohol-related problems at lower spatial scales than administratively defined areas such as wards or census tracts (Parker 2004). Many studies in this field draw on spatial modelling approaches and ecologic theories derived from the field of environmental criminology. Spatial modelling approaches are mostly used to identify areas at a micro-spatial scale with a higher level of specific problems (often referred to as ‘hotspots’). To explain the higher incidence of problems in these hotspots, spatial relationships with functional characteristics of the hotspot and their surroundings are being studied (see for example Schuurman et al. 2009; Walker et al. 2014).
Such studies are particularly useful to study associations between the alcohol-related harm and the functional environment. Functional environment refers to land use such as residential area, shopping area, or recreational area, and the functions of specific buildings such as bars, supermarkets, or homeless shelters. One important theme in this literature is the density of alcohol outlets as a key determinant of hotspots of alcohol-related violence (Grubesic and Pridemore 2011; Gruenewald and Remer 2006; Gruenewald et al. 2006; Quick et al. 2016), increased consumption (Van Oers and Garretsen 1993; Popova et al. 2009), alcohol-related incidents such as pedestrian injuries (LaScala et al. 2001; DiMaggio et al. 2016), vehicle crashes (Scribner et al. 1994; Treno et al. 2007), hospital admissions (Tatlow 2000), and other alcohol-related harm (Connor et al. 2011). Clusters of alcohol outlets in night-time leisure zones are known to be related to relatively high numbers of alcohol-related incidents (for a systematic review of studies, see Popova et al. (2009). Entertainment districts create the potential for alcohol-related problems, such as violence, by generating large numbers of people in various states of intoxication and who spill out onto the streets at closing time (Gorman et al. 2013). The routine-activity theory hypothesizes that clusters of alcohol outlets provide an opportunity for the intersection of offenders and targets which in the absence of guardianship may increase the risk of alcohol-related violence (Parker 2004).
The focus on outlet density may ignore the role of other environmental characteristics. Relatively few studies use a more comprehensive approach, i.e. one that considers the contribution of a wider array of environmental factors. In Worcester (United Kingdom) patterns of alcohol-related crime and disorder in the city centre were associated with various characteristics of the functional environment, with higher rates along the key route ways towards residential areas and retail zones, and close to functional sites such as the railway station and the shopping centre (Bromley and Nelson 2002). Similar studies on hotspots of violent injuries identified environmental features such as a high number of bars, recreation facilities, transit nodes, high density housing, public restrooms and homeless shelters (Braga et al. 1999; Cusimano et al. 2010; Walker and Schuurman 2012).
Until now, studies outside the scope of outlet density are relatively scarce as compared to the potentially large number of environmental factors that could play a role. Moreover, most studies have listed the role of isolated factors that are measurable in quantitative studies. Little attention has been given to the social-cultural or historical context of areas, and how these may interact with other environmental factors in generating or preventing alcohol-related incidents. To assess this complexity of factors, commonly used quantitative methods may need to be extended with qualitative approaches.
In this study, we focus on hotspots of alcohol-related incidents outside of areas with high outlet density in Amsterdam. Our aim is to characterise the local environments of these areas. We pay attention to a wide range of potential relevant aspects and use quantitative and qualitative techniques. We had three specific aims. First, we aimed to identify hotspots of alcohol-related ambulance attendances in Amsterdam outside of the well-known outlet density areas. Next, we aimed to assess the victim and temporal characteristics of incidents in these hotspots, and to compare these with characteristics of incidents in hotspots with high outlet density. Particular victim or temporal patterns may guide further search for relevant environmental factors. Finally, for the four highest incident hotspots outside high outlet density areas, we created environmental profiles with the aim to identify combinations of environmental factors that could possibly contribute to the occurrence of alcohol-related incidents.
Materials and methods
Ethics statement
The incidence data were analysed anonymously. As the Dutch Act on Medical Research Involving Human Subjects does not apply to this study, an official approval of this study by the AMC Medical Ethics Review Committee (MERC) was not required (MERC letter W12_275 # 12.17.0314).
Study design
We used an exploratory, observational study design incorporating quantitative and qualitative methods.
Incidence data were acquired from the register of the Regional Ambulance Services Agglomerate Amsterdam (RAVAA). The operator in the emergency control room who receives an incoming phone call determines whether an ambulance will be sent to the incident location. The register records the location and time of all ambulance attendances, characteristics of the persons involved, and the circumstances and nature of each incident. The information for each incident was derived from the incoming phone call. Additional information came from attending paramedics, who gave feedback to the operator on details of the ambulance attendance, and from the emergency department in case of transportation of the victim to a hospital.
An alcohol-related incident was defined as an incident in which the person suffered from the direct or indirect consequences of alcohol consumption, predominately including poisoning, reduced consciousness, and wounds, but also other injuries. To classify injuries as alcohol-related we used the short descriptions of the incoming phone call, the situation encountered by the paramedics, and the feedback from the emergency department. Records were selected when at least one of the three short descriptions contained a keyword related to drinking, drunkenness, alcohol, or specific alcoholic beverages.
The dataset included 11,256 alcohol-related incidents from 2006 to 2011. We excluded incidents with no information on the precise spatial location. In the end, a total of 11,155 incidents were included in the study.
Identification of hotspots
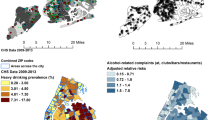
We used Geographic Information Systems (GIS) to construct hotspots of alcohol-related incidents based on the incident’s six-digit postal code. A six-digit postal code area is the smallest geographical area unit available. These units are sized approximately 50 × 50 metres and have on average 42 inhabitants. Figure 1 shows how the alcohol-related ambulance attendances are spread among these areas across the entire city.

Spatial pattern of alcohol-related ambulance attendances
To construct hotspots we applied the approach used in the Regiomonitor Amsterdam. This monitor was developed by the University of Amsterdam and the Municipality of Amsterdam to support policy makers and planners by showing spatial concentrations of social phenomena in the city. The approach aimed to identify areas that clearly deviate from the average situation with regard to events of interest.
According to this procedure, hotspots were created in three steps. The first step was to select postcodes that meet the selection criterion regarding a minimum number of incidents. More specifically, the number of alcohol-related attendances should be two standard deviations above the average. In practice, this means a minimum of 2 incidents (.61 + 2 × .49). We consider two standard deviations a reasonable compromise between two criteria. On the one hand, we wanted the identified hotspots to be large enough to be meaningful. On the other hand, it allowed the identification of a reasonable number of hotspots.
Secondly, each selected postcode area was extended by a buffer of 25 m metres and resulting overlapping postcode areas were combined into larger spatial units. A distance of 25 is considered as a reasonable definition of adjacency in urban areas with a comparable morphology. Finally, the number of incidents was recalculated for each postcode aggregate. The resulting 213 spatial aggregates were considered hotspots of potential interest to our analysis (see Pfeffer et al. 2012; Veldhuizen and Pfeffer 2016).
To remove the effect of outlet density as a main predictor of alcohol-related incidents, we excluded hotspots that contained more than one bar within a 100-metre buffer surrounding the hotspot. A 100 m margin was included to take into account the mobility of persons after visiting bars, which may lead to incidents occurring at some short distance from the bars of exposure. Moreover, we excluded all hotspots that were located within the city centre, because of the specific recreational and touristic functions of the city centre, and the deviant recreational behaviour of its highly transient population. After these exclusions, 75 hotspots remained for analysis.
In order to have sufficient observations, we decided to restrict further analysis to the larger hotspots. The analysis of victim and temporal profiles (see below) was restricted to the 11 hotspots with at least 10 incidents. Further analyses, aimed to assess environmental profiles, was restricted to the four hotspots with the highest number of incidents.
A main issue in the construction of hotspots is whether basic areas should be weighted according to their population size, area or some other feature that is proportional to the expected number of alcohol-related incidents. An argument to correct for population would be that a larger resident population size would generate a higher number of incidents. However, not only the number of residents in an area should be taken into account, but also non-residents, because the size of transient population may greatly vary between areas. Indeed, we found that the corresponding correlation between the number of incidents and size of the residential population to be almost 0 (.019). Alternatively, one might correct for the area size because a larger area would correspond to a higher number of incidents. However, this correlation was almost 0 as well (.017). In the Amsterdam context, many larger postcode areas may be relatively empty areas both in terms of residential and transient population.
Another issue is the robustness of the results to minor changes in the criteria used to identify the hotspots, such as a minimum number of 2 incidents. We checked for sensitivity and found that minor changes, for instance 3 instead of 2 incidents, would not have influenced our main results.
Victim and temporal profiles
For alcohol-related incidents that occurred within the selected hotspots (defined as group 1, N = 242), we compared victim characteristics (age, sex, place of residence) and temporal characteristics (day and time of incident) with that of two other groups of incidents: incidents in hotspots with high outlet density (group 2, N = 2210) and incidents within the city centre (group 3, N = 3205). Incidents outside of any hotspot (N = 5498) were not included in the analysis.
Differences in victim and temporal profiles between the three groups of incidents were assessed by comparing means and using cross table analysis. In addition, we used (logistic) regression analysis to quantify the differences between the three groups in victim and temporal characteristics of the incidents. The incidents are the units of analysis. The dependent variables are the victim characteristics (such as age 18–24 or not) and the temporal characteristics (such as in the weekend or not). The independent variable is the group, where group 1, our group of interest, is the reference category. The results of the models are expressed in terms of odds ratios (OR) and the associated 95% CI.
In many cases, it was not possible to classify incidents accurately according to the nature of the incident. The free-text descriptions of injuries are relatively short and during peak times the ambulance service had little time to report relevant information.
Environmental profiles
To create environmental profiles for the four highest incident hotspots with most incidents, we used both quantitative and qualitative data. To describe the social environment, we used integral social and socio-economic registries at the six-digit postal code level for the year 2009. These registries were maintained by the municipality of Amsterdam. For each hotspot, we aggregated the postal code level data and we calculated the percentage of residents receiving social benefits (unemployment or welfare), the percentage of the population aged 18 through 24, the percentage of non-Western migrants, and the percentage of houses under social housing schemes. The functional environment was described using data from the city’s Department of Planning, where the ‘Map of Functions’ described the function of each object on the map (for example, supermarket, discotheque, or hotel). Information on traffic infrastructure and traffic safety was obtained from the Department of Transport and Infrastructure. Furthermore, we used Google Street View to explore and describe the built environment. The highly detailed imagery available in Google Street View raises the possibility to virtually being in the neighbourhood. We systematically observed the hotspots in terms of residential density, dwelling types, amount of green space, functions and road infrastructure. We examined environmental characteristics which can be considered as potential risk factors with regard to an alcohol-related incident. We selected functions where alcohol can be bought or functions that attract risk populations such as homeless people. Relevant characteristics of the functional, social and built environment were selected based on results of previous studies mentioned in the introduction (for example Bromley and Nelson 2002; Braga et al. 1999; Cusimano et al. 2010; Walker and Schuurman 2012).
Qualitative methods were used to provide additional information on the local context of the highest incident hotspots which cannot be captured by quantitative measures or by using Google Street View. Studies assessing the usefulness of Street View to examine neighbourhood characteristics found that many characteristics, such as general land use, can be assessed reliably using Street View. However, small-scale features (such as garbage, broken bottles of beer) or temporarily variable features, such as the presence of people (such as youth hanging around), benefit from direct observation in the field (Clarke et al. 2010; Rundle et al. 2011). Additionally, we sought to obtain information on the cultural and historical context of each area and on local activities. The information was gathered during field visits and face-to-face interviews with two persons for each hotspot: the district manager (responsible for the communication between inhabitants, municipality, schools and police within a specific area) and the police officer (responsible for safety and crime issues). We thus interviewed eight persons in total. These persons were chosen as they were familiar with the areas in which the four large hotspots were located, as each of them had worked for several years in their respective area. Because of the exploratory nature of our research, the interviews were unstructured and guided by the results of preceding quantitative analyses.
The resulting information consisted of eight sets of interview notes, each one to two pages long. We analysed the data systematically by preparing a matrix for each hotspot that lists the main topics that are relevant to alcohol-related problems (what, where, when, who, why) in the columns. Each matrix consisted of two rows representing the two key informants. The data in the matrix showed to what extent perceptions of the key informants were similar or different, and were used to construct the environmental profiles for each area.
Results
From 2006 to 2011, 11,155 incidents were recorded in areas Amsterdam. The number of incidents ranged from 0 to 190 at the level of the 18,287 six-digit postcode areas. The average number of incidents was .61 and the corresponding standard deviation was .49. On the basis of our selection criteria, 11 hotspots with 242 incidents were identified for further analysis. Figure 2 shows the geographical distribution of these hotspots. By definition, they were located outside of areas with high outlet density and outside the city centre. Most hotspots were located within the “ring road”, which is a circle of highways about 5 kilometre away from the city centre. The hotspots varied not only in number of incidents, but also in size and shape.

Hotspots outside of areas with high outlet density
Table 1 compares the victim and temporal characteristics of the incidents in these hotspots with those of incidents in the other two groups of incidents. To establish the significance of the differences, 7 univariate (logistic) regression analyses were performed. In each analysis, the incidents were the units of analysis and the independent variable was the group (with group 1 as reference category). In each analysis a specific victim characteristic (for instance male or not) or temporal characteristic (for instance during the night or not) was the dependent variable. The % 18–24, for instance, was considerably higher in group 2 (21.2) and 3 (23.0) than in group 1 (11.7). This corresponds with OR’s significantly higher than 1 for group 2 (2.02) and group 3 (2.24). Compared with victims in high-outlet density hotspots and the city centre, victims in our hotspots of interest were on the average older and more often male. Also, these victims were more often residents of the surrounding neighbourhood (defined as the four-digit postal code area). Incidents in our hotspots of interest were less likely to occur during the night or during the weekend.
Table 2 compares victim and temporal characteristics of incidents within the four highest incident hotspots (A–D), taking incidents in high outlet density hotspots as the reference group. Victim and temporal profiles differ between the four hotspots. Striking patterns include: a low percentage of incidents during the night in A; a high percentage of incidents during the night and during the weekend in B (comparable with the reference group); a high percentage of victims aged 18 through 24 and male victims in C (again, comparable with the reference group), and a high percentage of victims aged 50 through 65, male victims, and of victims who reside in the surrounding neighbourhood in case of D. Although all incidents belong to group 1 substantial differences can be observed in the victim and temporal characteristics between the four hotspots.
Figure 3 shows the built environment of the four large hotspots. The hotspots strongly differ in terms of residential density, dwelling types, amount of green space, and infrastructure. For example, hotspot A is a densely populated residential area bordering the ring highway. Hotspot B contains a recreational park and an important traffic junction. Hotspot C is a heterogeneous, relatively low populated area containing a diverse mix of functions such as family dwellings, apartments, schools, offices and a train station. Hotspot D is characterised by high blocks of flats surrounded by much public green space.

Source: Google Earth
The built environment of the four large hotspots.
Table 3 lists, for each of the four hotspots, the characteristics of the social, functional and built environment that we regarded as potential risk factors for alcohol-related incidents. All hotspots had populations with relatively low socio-economic status. A and C have facilities that may attract potential risk groups, such as a homeless shelter, a low-budget hotel, and student housing. In B and D alcohol is sold in local retail outlets such as supermarkets. Most hotspots have public locations that are attractive for drinking alcohol, such as benches in public green spaces.
By combining this information with qualitative information that we obtained from interviews, we could construct environmental profiles for each of the four hotspots.
Hotspot A combines various environmental characteristics that all may be important. First of all, this area hosts a homeless shelter (HVO) whose residents often are psychiatric patients. Secondly, the surrounding streets are characterised by a high concentration of social housing. According to police officers, residents are less likely to call the authorities in the case of disturbances or nuisance. Along with the presence of benches surrounded by public green space, this contributes to an environment where alcohol consumers can spend time in relative anonymity. Thirdly, a shopping centre only a few hundred metres away creates opportunities for begging, getting alcohol, and socialising. The shopping centre is a run-down area and is generally avoided by older people and families with children. HVO users are perceived as having ‘taken over’ the square in the middle of the shopping centre. As long as they do not cause too much trouble, they are permitted to stay, or overlooked by law enforcement officers.
In hotspot B, two environmental constellations may explain the high number of alcohol-related incidents in this area. First, just outside of this hotspot, big dance events and concerts are organized at the Westergasfabriek Culture Park. Visitors of the events are channeled on a route way to the city centre which crosses the hotspot. Many road traffic accidents occur at a junction on this route way inside the hotspot (a so-called traffic black spot, a concentration of road traffic accidents). Secondly, the area itself is characterised by high unemployment rates and a high prevalence of socio-psychological problems. There is a regular group of alcoholics, generally older men, who drink in the Westerpark, an attractive public park with benches. Aggressive situations have arisen there frequently.
Hotspot C has a high concentration of student housing. Notorious are student parties during which large quantities of alcohol are often consumed. In addition, this hotspot includes one of the key train stations in Amsterdam, which also serves as Amsterdam’s principal pick-up location for international low-budget hire cars. The large numbers of young people waiting there in a holiday mood often generates a favourable context for alcohol and drugs consumption.
Hotspot D is located in a district with frequent problems related to drugs, crime, violence, early school leaving, and unemployment. An elaborate programme of physical and socio-economic renewal implemented between 1992 and 2009 improved the situation considerably. However, drug-related problems and other problems still occur. People with social problems are concentrated in two big anonymous blocks of flats in this hotspot. Moreover, this area attracts many visitors, including those from risk groups, because of the presence of shopping centre, metro station, youth centre, one local bar, and a centre for addicts. Aside from the bar, alcohol is also available in the supermarket, a late-night shop, and a number of ‘tokos’ (Asian food shops that also sell plastic bags of ‘bitters’ (drinks containing 42% alcohol). Additionally, the green space (including comfortable benches) that is abundant in this area, creates an attractive context for drinking.
A particular phenomenon in this area of Amsterdam are flat parties. Local residents, most of whom are from Africa, Suriname, or the Caribbean, organize parties for the ‘extended family’, including friends and neighbours. Much alcohol is consumed during some of these parties.
The four hotspots have different environmental characteristics which correspond to some extent with the different victim and temporal characteristics found in Table 2. For example, in hotspot A, the presence of the HVO corresponds to the small number of incidents occurring during the night and during the weekend and the high number of incidents among people from the same neigbhourhood. In hotspot B, the dance events which take place in that area corresponds with a lot of incidents during the night and the weekend and victims not living in the neigbhourhood. In hotspot D, the attractiveness of the area for visitors corresponds with the high percentage of victims coming from surrounding neighbourhoods. For hotspot C no direct link could be made.
Further analyses of the short free-text descriptions in the incidence registry showed that incidents related to mental problems and alcoholism occurred relatively often in A, traffic incidents in B, hazardous alcohol use and drugs abuse in C and mental problems and violence in D. These type of incidents correspond with the environmental profiles of the different hotspots (as depicted above). For example, in B, the higher number of traffic-related incidents corresponds with the potential role of the traffic black spotSimilarly, in D, the higher number of violence-related incidents corresponds with the unsafe character of this area.
Discussion
This study has identified and described hotspots of alcohol-related ambulance attendances outside of the entertainment districts of Amsterdam. Compared with hotspots with high outlet density, victims are older, are more often male, and live closer to the location of the incident. Incidents in most hotspots are less likely to happen during the night or during the weekend. In-depth study of four hotspots revealed widely different ways in which specific local environments could possibly contribute to the occurrence of incidents in a neighbourhood.
Evaluation of data and methodology
Because the ambulance dataset provides information about the six-digit postcode of the location of serious alcohol-related incidents we were able to accurately determine relevant hotspots, while the availability of micro-scale environmental data for the city of Amsterdam allowed us to characterise the hotspots that we identified.
A limitation of these data is that inaccurate registration could have led to underestimation of alcohol-related injuries. However, this underestimation could not have affected our results unless the degree of underestimation would systematically differ between the groups of incidents or between hotspots.
There are a variety of methods for determining hotspots. In general, the nature of the data and the purpose of study determine which method is most appropriate. We used the mapping approach described and employed by Pfeffer et al. (2012), because it produces hotspots with the geographical detail necessary for identifying small clusters of incidents and for describing their immediate surroundings. In this approach, accurate boundaries could be drawn based on micro areas comprising only a few addresses, thus neatly representing the actual distribution of observations. Hotspots represented by density surfaces based on grid cells—frequently used in crime hotspot analysis (Chainey and Ratcliffe 2005)—were not considered, because they assume a continuous distribution of observations over the study area. Such an assumption would greatly affect our ability to detect small-scale hotspots.
The number of alcohol-related incidents in hotspots outside of entertainment districts was relatively small, and our findings should be interpreted accordingly. However, on the scale of a few blocks, ten incidents involving ambulance attendances in just a few years is a phenomenon of significance to the local residents. Moreover, hotspots outside of entertainment districts may reflect the impact of environmental determinants that could create similar clusters of problems, though too diffuse to be noticed, in other parts of the city.
By preparing environmental profiles of hotspots, we aimed to identify environmental characteristics, or combinations of these, that may induce a concentration of alcohol-related incidents. We recognise that we should be very careful to infer causality, because our analysis is cross-sectional and lacks a systematic comparison with characteristics of areas outside of hotspots. In our study, some support for causal inference may come from two sources. First, to our knowledge of the geography of Amsterdam, many of the identified constellations of environmental factors are rare, and would very probably not be found in a random selection of control areas. Second, the victim and temporal profiles of the alcohol incidents often corresponded to the type of environmental factors that we identified in the qualitative analysis. Nonetheless, further mixed-methods are needed, preferably in other cities as well, to test for the plausibility and generalisability of relationships suggested by our analysis.
Interpretation and comparison with previous studies
Our study has shown that hotspots of alcohol-related incidents also occur outside of outlet dense areas. To date, no other study has explored the environmental characteristics of such hotspots by combining quantitative and qualitative methods.
We found that some hotspots emerged around social services such as a homeless shelter and a centre for addicts. However, many such services exist in Amsterdam without a corresponding hotspot in alcohol-related incidents, suggesting that the presence of such a service was in itself not sufficient to give rise to a hotspot. We found that the occurrence of hotspots depended upon the wider functional, physical, and social environment. More specifically, hotspots of alcohol-related incidents arose when combined with a favourable drinking context, including attractive locations where it is possible to sit and drink in relative anonymity.
A previous study (Schuurman et al. 2009) found hotspots of pedestrian injuries to occur where unsafe and complex traffic situations exist close to retail establishments that serve alcohol. We found a comparable pattern in one of our hotspots, where visitors of dance events have to cross a traffic black spot on their way home. These results imply that roadway design and traffic safety measures are particularly important at locations frequently visited by people under the influence of alcohol.
The results of some of our hotspots can be interpreted in terms of social disorganisation theory and more specifically the collective efficacy thesis as emphasised in research on neighbourhood crime (Shaw and McKay 1942; Sampson and Groves 1989). Collective efficacy refers to the ability of members of a community to control the behaviour of individuals or groups in the community (Sampson et al. 1997). We found that hotspots of alcohol-related incidents could occur in deprived neighbourhoods where social housing concurs with little social control and a high tolerance to deviant behaviour. In line with the collective efficacy perspective, social housing may hinder neighbourhood collective efficacy processes because of reduced social cohesion and fewer vested interests among community members. Previous empirical studies found that more deprived areas show a higher level of acceptance of deviant behaviour (Friedrichs and Blasius 2003; Sampson and Raudenbush 1999). Sampson and Raudenbush (1999) stressed the important role of home ownership. Financial investments provide homeowners with a vested interest in supporting the commonweal of neighbourhood life and in promoting collective efforts to maintain social control. In contrast, residents in more deprived areas dominated by social housing tend to be more indifferent to what goes on in their neighbourhoods and may be less likely to call the authorities in the case of disturbances like drinking in public.
Conclusions
This study has shown that hotspots of alcohol-related incidents may emerge outside of areas with high outlet density. Our results indicate that the local environment could give rise to hotspots of alcohol incidents in a great variety of ways which could not have been captured by statistical analyses of quantitative data. This underlines that place-specific context-sensitive research that include qualitative methods is needed to understand how local environments may induce or prevent the occurrence of alcohol-related problems.
References
Bernstein, K. T., Galeo, S., Ahern, J., Tracy, M., & Vlahov, D. (2007). The built environment and alcohol consumption in urban neighbourhoods. Drug and Alcohol Dependence, 91(2–3), 244–252.
Braga, A., Weisburd, E., Waring, L., Mazerolle, L., Spelman, W., & Gajewski, F. (1999). Problem-oriented policing in violent crime place: a randomized controlled experiment. Criminology, 37(3), 541–580.
Bromley, D. F., & Nelson, A. L. (2002). Alcohol-related crime and disorder across urban space and time: Evidence from a British city. Geoforum, 33(2), 239–254.
Cerda, M., Diez-Roux, A. V., Tchetgen Tchetgen, E., Godon-Larsen, P., & Kiefe, C. (2010). The relationship between neighborhood poverty and alcohol use: Estimation by marginal structural models. Epidemiology, 21(4), 482–489.
Chainey, S., & Ratcliffe, J. (2005). GIS and crime mapping. London: Wiley.
Clarke, P., Ailshire, J., Melendez, R., Bader, M., & Morenoff, J. (2010). Using google earth to conduct a neighborhood audit: Reliability of a virtual audit instrument. Health and Place, 16(6), 1224–1229. doi:10.1016/j.healthplace.2010.08.007.
Connor, J. L., Kypri, K., Bell, M. L., & Cousins, K. (2011). Alcohol outlet density, levels of drinking and alcohol-related harm in New Zealand: A national study. Journal of Epidemiology and Community Health, 65(10), 841–846.
Cornaz, S., Taffe, P., & Santos-Eggimann, B. (2009). Life-course socioeconomic environment and health risk behaviours. A multilevel small-area analysis of young-old persons in an urban neighbourhood in Lausanne, Switzerland. Health and Place, 15(1), 273–283.
Cusimano, M., Marshall, S., Rinner, C., Jiang, D., & Chipman, M. (2010). Patterns of urban violent injury: A spatio-temporal analysis. PLoS ONE, 5(1), 1–9.
DiMaggio, C., Mooney, S., Frangos, S., & Wall, S. (2016). Spatial analysis of the association of alcohol outlets and alcohol-related pedestrian/bicyclist injuries in New York City. Injury Epidemiology, 3(1), 11. doi:10.1186/s40621-016-0076-5.
Ecob, R., & Macintyre, S. (2000). Small area variations in health related behaviours; Do these depend on the behaviour itself, its measurement, or on personal characteristics? Health and Place, 6(4), 261–274.
Elliott, M. (2000). The stress process in neighbourhood context. Health and Place, 6(4), 287–299.
Friedrichs, J., & Blasius, J. (2003). Social norms in distressed neighbourhoods: Testing the Wilson hypothesis. Housing Studies, 18(6), 807–826.
Galea, S., Ahern, J., Tracy, M., & Vlahov, D. (2007). Neighborhood income and income distribution and the use of cigarettes, alcohol, and marijuana. American Journal of Preventive Medicine, 32(6), 195–202.
Gorman, D. M., Gruenewald, P. J., & Waller, L. A. (2013). Linking places to problems: Geospatial theories of neighbourhoods, alcohol and crime. GeoJournal, 78(3), 417–428.
Grubesic, T. H., & Pridemore, W. A. (2011). Alcohol outlets and clusters of violence. International Journal of Health Geographics. doi:10.1186/1476-072X-10-30.
Gruenewald, P. J., Freisthler, L., Remer, L., Lascala, E. A., & Treno, A. (2006). Ecological models of alcohol outlets and violent assaults: Crime potentials and geospatial analysis. Addiction, 101(5), 666–677.
Gruenewald, P. J., & Remer, L. (2006). Changes in outlet densities affect violence rates. Alcoholism: Clinical and Experimental Research, 30(7), 1184–1193.
Halonen, J. I., Kivimäki, M., Pentti, J., et al. (2012). Quantifying neighbourhood socioeconomic effects in clustering of behaviour-related risk factors: A multilevel analysis. PLoS ONE, 7(3), e32937. doi:10.1371/journal.pone.0032937.
Jayne, M., Valentine, G., & Holloway, S. L. (2008). Geographies of alcohol, drinking and drunkenness: A review of progress. Progress in Human Geography, 32(2), 243–259.
Karriker-Jaffe, K. J. (2011). Areas of disadvantage: A systematic review of effects of area-level socioeconomic status on substance use outcomes. Drug and Alcohol Review, 30(1), 84–95.
Kuipers, M. A. G., Jongeneel-Grimen, B., Droomers, M., Wingen, M., Stronks, K., & Kunst, A. E. (2013). Why residents of Dutch deprived neighbourhoods are less likely to be heavy drinkers: The role of individual and contextual characteristics. Journal of Epidemiology and Community Health. doi:10.1136/jech-2012-201242.
LaScala, E. A., Gruenewald, P. J., & Johnson, F. (2001). Neighborhood characteristics of alcohol-related pedestrian injury collisions: A geostatistical analysis. Prevention Science, 2(2), 123–134.
Parker, R. N. (2004). Alcohol and violence: Connections, evidence and possibilities for prevention. Journal of Psychoactive Drugs, 36(2), 157–163.
Pfeffer, K., Deurloo, M. C., & Veldhuizen, E. M. (2012). Visualising postcode data for urban analysis and planning: the Amsterdam City Monitor. Area, 44(3), 326–335.
Pollack, C. E., Cubbin, C., Ahn, D., & Winkleby, M. (2005). Neighbourhood deprivation and alcohol consumption: Does the availability of alcohol play a role? International Journal of Epidemiology, 34(4), 772–780.
Popova, S., Giesbrecht, N., Bekmuradov, D., & Patra, J. (2009). Hours and days of sale and density of alcohol outlets: Impacts on alcohol consumption and damage: A systematic review. Alcohol and Alcoholism, 44(5), 500–516.
Quick, M., Law, J., & Luan, H. (2016). The influence of on-premise and off-premise alcohol outlets on reported violent crime in the region of Waterloo, Ontario: Applying Bayesian spatial modeling to inform land use planning and policy. Applied Spatial Analysis. doi:10.1007/s12061-016-9191-5.
Robert, S. (1999). Socioeconomic position and health: The independent contribution of community socioeconomic context. Annual Review of Sociology, 25(1), 489–516.
Romley, J. A., Cohen, D., Ringel, J., & Sturm, R. (2007). Alcohol and environmental justice: The density of liquor stores and bars in urban neighbourhoods in the United States. Journal of Studies on Alcohol and Drugs, 68(1), 48–55.
Rundle, A. G., Bader, M. D. M., Richards, C. A., Neckerman, K. M., & Teitler, J. O. (2011). Using Google Street View to audit neighborhood environments. American Journal of Preventive Medicine, 40(1), 94–100. doi:10.1016/j.amepre.2010.09.034.
Sampson, R. J., & Groves, W. B. (1989). Community structure and crime: testing social disorganization-theory. American Journal of Sociology, 94(4), 774–802.
Sampson, R. J., & Raudenbush, S. W. (1999). Systematic social observation of public spaces: A new look at disorder in urban neighborhoods. American Journal of Sociology, 105(3), 603–651.
Sampson, R. J., Raudenbush, S. W., & Earls, F. (1997). Neighbourhoods and violent crime: A multilevel study of collective efficacy. Science, 277(5328), 918–924.
Schuurman, N., Cinnamon, J., Crooks, V. A., & Hameed, S. M. (2009). Pedestrian injury and the built environment: An environmental scan of hotspots. BMC Public Health. doi:10.1186/1471-2458-9-233.
Scribner, R. A., Mackinnon, D. P., & Dwyer, J. H. (1994). Alcohol outlet density and motor vehicle crashes in Los Angeles County cities. Journal of Studies on Alcohol, 55(4), 447–453.
Shaw, C. R., & McKay, H. D. (1942). Juvenile delinquency in urban areas. Chicago: University of Chicago Press.
Stimpson, J. P., Ju, H., Raij, M. A., & Eschbach, K. (2007). Neighborhood deprivation and health risk behaviors in NHANES III. American Journal of Health Behavior, 31(2), 215–222.
Tatlow, J. R. (2000). The relationship between the geographic density of alcohol outlets and alcohol-related hospital admissions in San Diego County. Journal of Community Health, 25(1), 79–88.
Treno, A. J., Johnson, F. W., Remer, L. G., & Gruenewald, P. J. (2007). The impact of outlet densities on alcohol-related crashes: A spatial panel approach. Accident Analysis and Prevention, 39(5), 895–901.
Ujcic-Voortman, J. K., Schilthuis, W., Osté, J. P., & Buster, M. C. A. (2013). Alcoholmonitor 2012. Amsterdam: GGD.
Van Oers, J. A. M., & Garretsen, H. F. (1993). The geographic relationship between alcohol use, bars, liquor shops and traffic injuries in Rotterdam. Journal of Studies on Alcohol, 54(6), 739–744.
Veldhuizen, E., Pfeffer, K. (2016). Crossing boundaries: Mapping urban dynamics of urban phenomena at micro scale to support urban management in the Amsterdam urban region. Belgeo. http://belgeo.revues.org/17740.
Walker, B. B., Hameed, S. M., & Schuurman, N. (2014). A GIS-based spatial-temporal analysis of violent trauma hotspots in Vancouver, Canada: Identification, contextualisation and intervention. British Medical Journal Open, 4(2), e003642.
Walker, B., & Schuurman, S. (2012). Environmental correlates with violent injury. Geomatica, 66(4), 269–278.
Acknowledgements
The authors gratefully acknowledge the Regional Ambulance Services Agglomerate Amsterdam (RAVAA) and the Department of Research and Statistics of the Municipality of Amsterdam for providing the data and our key informants for providing valuable information.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interests.
Ethical approval
The incidence data were analysed anonymously. As the Dutch Act on Medical Research Involving Human Subjects does not apply to this study, an official approval of this study by the AMC (Academic Medical Center) Medical Ethics Review Committee (MERC) was not required (MERC letter W12_275 # 12.17.0314).
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Veldhuizen, E.M., Osté, J. & Kunst, A.E. Environmental characteristics of hotspots of alcohol-related health incidents outside of the entertainment districts of Amsterdam. GeoJournal 83, 1053–1066 (2018). https://doi.org/10.1007/s10708-017-9818-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10708-017-9818-3