
Abstract
Purpose
To describe the stages of development and natural course of a full-thickness macular hole (FTMH) in a patient with enhanced S-cone syndrome (ESCS).
Methods
This study reported the serial ophthalmologic examinations and macular spectral-domain optical coherence tomography (SD-OCT) imaging over a period of 6 years in a 29-year-old man with ESCS confirmed by electroretinography (ERG) and NR2E3 molecular genetic analysis.
Results
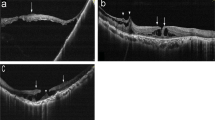
At presentation, patient had night blindness and visual acuity (VA) of 20/300 in the right eye (OD) and 20/100 in the left eye (OS). Examination showed bilateral retinal midperipheral pigmentary deposits and a macular schisis in OD. Electroretinography and NR2E3 genetic analysis confirmed ESCS. A year later, a lamellar MH (LMH) appeared at the fovea in OD. SD-OCT confirmed it as inner retinal layer LMH with outer retinal preservation and displayed, on the temporal side of the LMH, prominent splitting between the inner and outer retinal layers. At 2 years, a focal defect in the ellipsoid zone appeared on SD-OCT, followed by split in the outer retinal layer creating a progressively expanding outer LMH. The latter had rolled edges which then fused with the inner LMH margins creating a single full-thickness FTMH. Over the next 4 years, enlargement of the FTMH with increased adjacent retinal splitting continued. No visible vitreous abnormalities or vitreoretinal traction forces were identified at any stage during follow-up. VA OD remained unchanged.
Conclusion
This case illustrates that the clinical evolution of FTMH in ESCS may be progressive and likely involves degeneration and intraretinal, rather than vitreoretinal, traction. This should be kept in mind when considering surgical intervention in these cases.



Similar content being viewed by others


Availability of data and material
This work was conducted at King Khaled Eye Specialist Hospital (KKESH). The case’s data are available at KKESH.
References
Marmor MF, Jacobson SG, Foerster MH et al (1990) Diagnostic clinical findings of a new syndrome with night blindness, maculopathy, and enhanced S cone sensitivity. Am J Ophthalmol 110(2):124–134
Vaclavik V, Chakarova C, Bhattacharya SS, Robson AG, Holder GE, Bird AC, Webster AR (2008) Bilateral giant macular schisis in a patient with enhanced S-cone syndrome from a family showing pseudo-dominant inheritance. Br J Ophthalmol 92(2):299–300
Yzer S, Barbazetto I, Allikmets R et al (2013) Expanded clinical spectrum of enhanced S-cone syndrome. JAMA Ophthalmol 131(10):1324–1330
Jacobson SG, MarmorMF Kemp CM et al (1990) SWS (blue) cone hypersensitivity in a newly identified retinal degeneration. Invest Ophthalmol Vis Sci 31:827–838
Vincent A, Robson AG, Holder GE (2013) Pathognomonic (diagnostic) ERGs. A review and update. Retina 33(1):5–12
Haider NB, Jacobson SG, Cideciyan AV et al (2000) Mutation of a nuclear receptor gene, NR2E3, causes enhanced S cone syndrome, a disorder of retinal cell fate. Nat Genet 24(2):127–131
Theodossiadis PG, Koutsandrea C, Kollia AC, Theodossiadis GP (2000) Optical coherence tomography in the study of the Goldmann-Favre syndrome. Am J Ophthalmol 129(4):542–544
Khairallah M, Ladjimi A, Ben Yahia S, Zaouali S, Messaoud R, Boulima K (2002) Elevated macular retinoschisis associated with Goldmann-Favre syndrome successfully treated with grid laser photocoagulation. Retina 22(2):234–237
Arevalo JF, Kozak I (2015) Enhanced S-cone syndrome and macular hole. JAMA Ophthalmol 133(6):e15108
Magliyah M, Saifaldein AA, Schatz P (2020) Late presentation of RPE65 retinopathy in three siblings. Doc Ophthalmol. https://doi.org/10.1007/s10633-019-09745-z
Chavala SH, Sari A, Lewis H, Pauer GJ, Simpson E, Hagstrom SA, Traboulsi EI (2005) An Arg311Gln NR2E3 mutation in a family with classic Goldmann-Favre syndrome. Br J Ophthalmol 89(8):1065–1066
Jacobson SG, Román AJ, Román MI, Gass JDM, Parker JA (1991) Relatively enhanced S cone function in the Goldmann-Favre syndrome. Am J Ophthalmol 111:446–453
Sharon D, Sandberg MA, Caruso RC et al (2003) Shared mutations in NR2E3 in enhanced S-cone syndrome, Goldman-Favre syndrome and many cases of clumped pigmentary retinal degeneration. Arch Ophthalmol 121:1316–1323
Wright AF, Reddick AC, Schwartz SB et al (2004) Mutation analysis in NR2E3 and NRL genes in enhanced S cone syndrome. Hum Mut 24:439
Gass JD (1999) Müller cell cone, an overlooked part of the anatomy of the fovea centralis: hypotheses concerning its role in the pathogenesis of macular hole and foveomacular retinoschisis. Arch Ophthalmol 117(6):821–823
Chen F, Figueroa DJ, Marmorstein AD et al (1999) Retina-specific nuclear receptor: a potential regulator of cellular retinaldehyde-binding protein expressed in retinal pigment epithelium and Müller glial cells. Proc Natl Acad Sci USA 96(26):15149–15154
Sohn EH, Chen FK, Rubin GS, Moore AT, Webster AR, MacLaren RE (2010) Macular function assessed by microperimetry in patients with enhanced S-cone syndrome. Ophthalmology 117(6):1199–1206.e1
Landa G, Gentile RC, Garcia PM, Muldoon TO, Rosen RB (2012) External limiting membrane and visual outcome in macular hole repair: spectral domain OCT analysis. Eye (Lond) 26(1):61–69
Funata M, Wendel RT, de la Cruz Z, Green WR (1992) Clinicopathologic study of bilateral macular holes treated with pars plana vitrectomy and gas tamponade. Retina 12(4):289–298
Madreperla SA, Geiger GL, Funata M, de la Cruz Z, Green WR (1994) Clinicopathologic correlation of a macular hole treated by cortical vitreous peeling and gas tamponade. Ophthalmology 101(4):682–686
Nork TM, Ghobrial MW, Peyman GA, Tso MO (1986) Massive retinal gliosis. A reactive proliferation of Müller cells. Arch Ophthalmol 104(9):1383–1389
Rosa RH Jr, Glaser BM, de la Cruz Z, Green WR (1996) Clinicopathologic correlation of an untreated macular hole and a macular hole treated by vitrectomy, transforming growth factor-beta 2, and gas tamponade. Am J Ophthalmol 122(6):853–863
McCulloch DL, Marmor M, Brigell MG et al (2015) ISCEV Standard for full-field clinical electroretinography (2015 update). Doc Ophthalmol 130:1–12
Thompson DA, Fujinami K, Perlman I, Hamilton R, Robson AG (2018) ISCEV extended protocol for the dark-adapted red flash ERG. Doc Ophthalmol 136(3):191–197
Funding
None.
Author information
Authors and Affiliations
Contributions
All authors attest that they meet the current ICMJE criteria for authorship. MM and SN designed and conducted the study. MM, SS, PS, and SN were involved in collection, management, analysis, and interpretation of the data, and contributed to the preparation, review, and final approval of the manuscript. Part of this material was submitted for poster presentation at the World Ophthalmology Congress Meeting in Cape Town on June 26–29, 2020.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest of financial disclosures.
Ethical approval
This retrospective case study involving a human participant was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments. The Human Investigation Committee (IRB) of King Khaled Eye Specialist Hospital (KKESH) approved this study (Ref. 19122024-R). No animal was involved in this study.
Informed consent
Informed consent was obtained from the individual participant included in the study.
Consent for publication
The patient has consented to the submission of the case report for submission to the journal. This report does not contain any personal information that could lead to the identification of the patient.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Magliyah, M.S., AlSulaiman, S.M., Schatz, P. et al. Evolution of macular hole in enhanced S-cone syndrome. Doc Ophthalmol 142, 239–245 (2021). https://doi.org/10.1007/s10633-020-09787-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10633-020-09787-8