
Abstract
Background
The endoscopic appearance in patients with “pouchitis” after ileal pouch-anal anastomosis (IPAA) for ulcerative colitis (UC) can be quite heterogenous. Patients with an endoscopic phenotype resembling Crohn’s disease (CD) are at high risk of pouch loss.
Aims
We aimed to assess how the histopathology of colectomy specimens predicts endoscopic pouch phenotypes in UC.
Methods
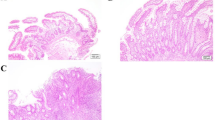
We retrospectively assessed pouchoscopies from patients with UC who underwent IPAA and classified pouch findings into 7 main phenotypes: (1) normal, (2) afferent limb involvement, (3) inlet involvement, (4) diffuse, (5) focal inflammation of the pouch body, (6) cuffitis, and (7) pouch with fistulas noted ≥ 6 months from ileostomy takedown. We assessed the clinical and pathological data including deep, focal inflammation, granulomas, and terminal ileal involvement in the colectomy specimens. Logistic regression analysis was performed to identify contributing factors to each phenotype.
Results
This study included 1,203 pouchoscopies from 382 patients with UC. On multivariable analysis, deep inflammation was significantly associated with pouch fistulas (Odds ratio 3.27; 95% confidence interval 1.65–6.47; P = 0.0007). Of the 75 patients with deep inflammation, only two patients (2.7%) were diagnosed with CD based on pathology review. Terminal ileal involvement significantly increased the risk of afferent limb involvement (Odds ratio 2.96; 95% confidence interval 1.04–8.47; P = 0.04). There were no significant associations between other microscopic features and phenotypes.
Conclusions
We identify histologic features of colectomy specimens in UC that predict subsequent pouch phenotypes. Particularly, deep inflammation in the resected colon was significantly associated with pouch fistulas, a pouch phenotype with poor prognosis.
Similar content being viewed by others

References
Akiyama S, Rai V, Rubin DT. Pouchitis in inflammatory bowel disease: a review of diagnosis, prognosis, and treatment. Intest Res. 2021;19:1-11.
Akiyama S, Ollech JE, Rai V, et al. Endoscopic phenotype of the J pouch in patients with inflammatory bowel disease: A new classification for pouch outcomes. Clin Gastroenterol Hepatol. 2022;20:293-302.
Pellino G, Vinci D, Signoriello G, et al. Long-term bowel function and fate of the ileal pouch after restorative proctocolectomy in patients with Crohn's disease: a systematic review with meta-analysis and metaregression. J Crohns Colitis. 2020;14:418-427.
Odze R. Diagnostic problems and advances in inflammatory bowel disease. Mod Pathol. 2003;16:347-358.
Yantiss RK, Farraye FA, O'Brien MJ, et al. Prognostic significance of superficial fissuring ulceration in patients with severe "indeterminate" colitis. Am J Surg Pathol. 2006;30:165-170.
Barnes EL, Kochar B, Jessup HR, et al. The incidence and definition of Crohn's disease of the pouch: a systematic review and meta-analysis. Inflamm Bowel Dis. 2019;25:1474-1480.
Nasseri Y, Melmed G, Wang HL, et al. Rigorous histopathological assessment of the colectomy specimen in patients with inflammatory bowel disease unclassified does not predict outcome after ileal pouch-anal anastomosis. Am J Gastroenterol. 2010;105:155-161.
Sandborn WJ, Tremaine WJ, Batts KP, et al. Pouchitis after ileal pouch-anal anastomosis: a pouchitis disease activity index. Mayo Clin Proc. 1994;69:409-415.
Shen B, Achkar JP, Connor JT, et al. Modified pouchitis disease activity index: a simplified approach to the diagnosis of pouchitis. Dis Colon Rectum. 2003;46:748-753.
Shen B, Remzi FH, Lavery IC, et al. A proposed classification of ileal pouch disorders and associated complications after restorative proctocolectomy. Clin Gastroenterol Hepatol. 2008;6:145–158; quiz 124.
Satsangi J, Silverberg MS, Vermeire S, et al. The montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut. 2006;55:749-753.
Cohen RD. Inflammatory Bowel Disease Diagnosis and Therapeutics. Third ed: Springer; 2016. p. 121–136.
Rubio CA, Asmundsson J, Silva P, et al. Lymphoid aggregates in Crohn's colitis and mucosal immunity. Virchows Arch. 2013;463:637-642.
Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377-381.
Kanda Y. Investigation of the freely available easy-to-use software 'EZR' for medical statistics. Bone Marrow Transplant. 2013;48:452-458.
Fazio VW, Tekkis PP, Remzi F, et al. Quantification of risk for pouch failure after ileal pouch anal anastomosis surgery. Ann Surg. 2003;238:605–614; discussion 614–607.
Kjaer MD, Kjeldsen J, Qvist N. Poor outcomes of complicated pouch-related fistulas after ileal pouch-anal anastomosis surgery. Scand J Surg. 2016;105:163-167.
Hahnloser D, Pemberton JH, Wolff BG, et al. Results at up to 20 years after ileal pouch-anal anastomosis for chronic ulcerative colitis. Br J Surg. 2007;94:333-340.
Tekkis PP, Fazio VW, Remzi F, et al. Risk factors associated with ileal pouch-related fistula following restorative proctocolectomy. Br J Surg. 2005;92:1270-1276.
Gaertner WB, Witt J, Madoff RD, et al. Ileal pouch fistulas after restorative proctocolectomy: management and outcomes. Tech Coloproctol. 2014;18:1061-1066.
Hermand H, Lefevre JH, Shields C, et al. Postoperative diagnostic revision for Crohn disease after subtotal colectomy for inflammatory bowel disease. Int J Colorectal Dis. 2021;36:709-715.
Nisar PJ, Kiran RP, Shen B, et al. Factors associated with ileoanal pouch failure in patients developing early or late pouch-related fistula. Dis Colon Rectum. 2011;54:446-453.
Li Y, Wu B, Shen B, et al. Diagnosis and differential diagnosis of Crohn's disease of the ileal pouch. Curr Gastroenterol Rep. 2012;14:406-413.
Loftus EV, Jr., Harewood GC, Loftus CG, et al. PSC-IBD: a unique form of inflammatory bowel disease associated with primary sclerosing cholangitis. Gut. 2005;54:91-96.
Mc CF, Bargen JA, et al. Involvement of the ileum in chronic ulcerative colitis. N Engl J Med. 1949;240:119-127.
Shen B, Bennett A·E, Navaneethan U, et al. Primary sclerosing cholangitis is associated with endoscopic and histologic inflammation of the distal afferent limb in patients with ileal pouch-anal anastomosis. Inflamm Bowel Dis. 2011;17:1890-1900.
Quinn KP, Urquhart SA, Janssens LP, et al. Primary sclerosing cholangitis-associated pouchitis: a distinct clinical phenotype. Clin Gastroenterol Hepatol. 2021.
Bell AJ, Price AB, Forbes A, et al. Pre-pouch ileitis: a disease of the ileum in ulcerative colitis after restorative proctocolectomy. Colorectal Dis. 2006;8:402-410.
Mousa OY, Juran BD, McCauley BM, et al. Bile acid profiles in primary sclerosing cholangitis and their ability to predict hepatic decompensation. Hepatology. 2021;74:281-295.
Rubin DT, Huo D, Kinnucan JA, et al. Inflammation is an independent risk factor for colonic neoplasia in patients with ulcerative colitis: a case-control study. Clin Gastroenterol Hepatol. 2013;11:1601-1608 e1601-1604.
Acknowledgments
The authors thank funding in part provided by NIDDK P30 DK42086, NIDDK RC2 DK122394, and the GI Research Foundation of Chicago
Funding
Funding in part provided by NIDDK P30 DK42086, NIDDK RC2 DK122394, and the GI Research Foundation of Chicago.
Author information
Authors and Affiliations
Contributions
SA, EBC, DTR took part in study concept and design; SA, JEO, CT, VR, YY, LRG, JR, ADO, CRW, JH, RDC, KSO, RDH, KU, BDS, NHH, MAR, SRD, AS, JP, DTR involved in acquisition of data; SA, CRW, JH, DTR took part in analysis and interpretation of data; SA, CT, VR, DTR involved in drafting of manuscript; SA, JEO, CT, VR, YY, LRG, JR, ADO, CRW, RDC, KSO, RDH, KU, BDS,NHH, MAR, SRD, AS, JP, EBC, JH, DTR took part in critical revision of manuscript. All authors have approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
SA, JEO, VR, LRG, YY, CT, JR, ADO, CRW, KSO, RDH, KU, BDS, NHH, AS, and JH have no relevant disclosures. RDC is on the speaker’s bureau from AbbVie and Takeda. He is a consultant/advisor for AbbVie Laboratories, BM/celgene, Eli Lilly, Gilead Sciences, Janssen, Pfizer, Takeda, UCB Pharma. He has received clinical trial support/grants from Abbvie, BMS/Celgene, Boehringer Ingelheim, Crohn’s and Colitis Foundation of America, Genentech, Gilead Sciences, Hollister, Medimmune, Mesoblast Ltd., Osiris Therpeutics, Pfizer, Receptos, RedHill Biopharma, Sanofi-Aventis, Schwarz Pharma, Seres Therapeutics, Takeda Pharma, UCB Pharma. His wife is on the board of directors of Aerpio Theraoeutics, Novus Therapeutics, Vital Therapeutics, Inc, and NantKwest. MAR has served as a consultant for Pfizer. SRD has served as a consultant for Pfizer and is on the speaker’s bureau for AbbVie. JP has received grant support from AbbVie and Takeda. He has served as a consultant for Veraste,. CVS Caremark and is on the advisory board for Takeda, Janssen and Pfizer. EBC is the founder and chief medical officer of AVnovum Therapeutics DTR has received grant support from Takeda; and has served as a consultant for Abbvie, Abgenomics, Allergan Inc., Arena Pharmaceuticals, Bellatrix Pharmaceuticals, Boehringer Ingelheim Ltd., Bristol-Myers Squibb, Celgene Corp/Syneos, Check-cap, Dizal Pharmaceuticals, GalenPharma/Atlantica, Genentech/Roche, Gilead Sciences, Ichnos Sciences S.A., InDex Pharmaceuticals, Iterative Scopes, Janssen Pharmaceuticals, Lilly, Materia Prima, Narrow River Mgmt, Pfizer, Prometheus Laboratories,Reistone, Takeda, and Techlab Inc. He is also co-founder of Cornerstones Health, Inc. and GoDuRn, LLC; on the Board of Trustees of the American College of Gastroenterology.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Akiyama, S., Ollech, J.E., Traboulsi, C. et al. Histopathology of Colectomy Specimens Predicts Endoscopic Pouch Phenotype in Patients with Ulcerative Colitis. Dig Dis Sci 67, 4020–4031 (2022). https://doi.org/10.1007/s10620-022-07405-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-022-07405-y