
Abstract
Background
Inpatient charges for patients with cirrhosis are substantial. We aimed to examine trends in inpatient charges among patients with cirrhosis to determine the drivers of healthcare expenditures. We hypothesized that alcoholic cirrhosis (AC) was a significant contributor to overall expense.
Methods
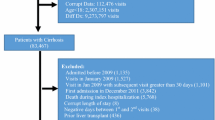
We performed a retrospective analysis of the Health Care Utilization Project Nationwide Inpatient Sample Database 2002–2014 (annual cross-sectional data) and New York and Florida State Inpatient Databases 2010–2012 (longitudinal data). Adult patients with cirrhosis of the liver were categorized as AC versus all other etiologies of cirrhosis combined. Patient characteristics were analyzed using ordinary least squares regression modeling. A random effects model was used to evaluate 30-day readmissions.
Results
In total, 1,240,152 patients with cirrhosis were admitted between 2002 and 2014. Of these, 567,510 (45.8%) had a diagnosis of AC. Total charges for AC increased by 95.7% over the time period, accounting for 59.9% of all inpatient cirrhosis-related charges in 2014. Total aggregate charges for AC admissions were $28 billion and increased from $1.4B in 2002 to $2.8B by 2014. In the NIS and SID, patients with AC were younger, white and male. Readmission rates at 30, 60, and 90 days were all higher among AC patients.
Conclusions
Inpatient charges for cirrhosis care are high and increasing. Alcohol-related liver disease accounts for more than half of these charges and is driven by sheer volume of admissions and readmissions of the same patients. Effective alcohol addictions therapy may be the most cost-effective way to substantially reduce inpatient cirrhosis care expenditures.

Similar content being viewed by others


Abbreviations
- AC:
-
Alcoholic cirrhosis
- HCV:
-
Hepatitis C
- NAFLD:
-
Nonalcoholic fatty liver disease
- NIS:
-
Nationwide Inpatient Sample
- HCUP:
-
Healthcare Cost and Utilization Project
- AHRQ:
-
Agency for Healthcare Research and Quality
- SID:
-
State Inpatient Database
- ICD-9-CM:
-
International Classification of Diseases, 9th Revision, Clinical Modification
- NC:
-
Nonalcohol-related cirrhosis
References
Bodenheimer T. High and rising health care costs. Part 1: seeking an explanation. Ann Intern Med. 2005;142:847–854.
Schmidt ML, Barritt AS, Orman ES, et al. Decreasing mortality among patients hospitalized with cirrhosis in the United States from 2002 through 2010. Gastroenterology. 2015;148:967-977 e2.
Peery AF, Crockett SD, Barritt AS, et al. Burden of gastrointestinal, liver, and pancreatic diseases in the United States. Gastroenterology. 2015;149:1731-1741.e3.
Peery AF, Crockett SD, Murphy CC, et al. Burden and cost of gastrointestinal, liver, and pancreatic diseases in the United States: update 2018. Gastroenterology. 2019;156:254-272.e11.
Ndugga N, Lightbourne TG, Javaherian K, et al. Disparities between research attention and burden in liver diseases: implications on uneven advances in pharmacological therapies in Europe and the USA. BMJ Open. 2017;7:e013620.
Williams R, Alexander G, Armstrong I, et al. Disease burden and costs from excess alcohol consumption, obesity, and viral hepatitis: fourth report of the Lancet Standing Commission on Liver Disease in the UK. Lancet. 2018;391:1097–1107.
O’Shea RS, Dasarathy S, McCullough AJ. Alcoholic liver disease. Hepatology. 2010;51:307–328.
Griswold MG, Fullman N, Hawley C, et al. Alcohol use and burden for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2018;392:1015–1035.
HCUP Nationwide Inpatient Survey (NIS). 2002–2010. www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed 2 May 2017.
Kramer JR, Davila JA, Miller ED, et al. The validity of viral hepatitis and chronic liver disease diagnoses in Veterans Affairs administrative databases. Aliment Pharmacol Ther. 2008;27:274–282.
Liu TL, Trogdon J, Weinberger M, et al. Diabetes is associated with clinical decompensation events in patients with cirrhosis. Dig Dis Sci. 2016;61:3335–3345.
Orman ES, Hayashi PH, Bataller R, et al. Paracentesis is associated with reduced mortality in patients hospitalized with cirrhosis and ascites. Clin Gastroenterol Hepatol. 2014;12:496-503 e1.
Zou G. A modified poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159:702–706.
Zou GY, Donner A. Extension of the modified Poisson regression model to prospective studies with correlated binary data. Stat Methods Med Res. 2013;22:661–670.
Molenberghs G, Verbeke G, Demetrio CG. An extended random-effects approach to modeling repeated, overdispersed count data. Lifetime Data Anal. 2007;13:513–531.
Orman ES, Hayashi PH, Bataller R, et al. Paracentesis is Associated with Reduced Mortality in Patients Hospitalized with Cirrhosis and Ascites. Clin Gastroenterol Hepatol. 2013;12:496–503.
Le S, Spelman T, Chong CP, et al. Could adherence to quality of care indicators for hospitalized patients with cirrhosis-related ascites improve clinical outcomes? Am J Gastroenterol. 2016;111:87–92.
Oppedal K, Moller AM, Pedersen B, et al. Preoperative alcohol cessation prior to elective surgery. Cochrane Database Syst Rev. 2012. https://doi.org/10.1002/14651858.CD008343.pub2.
Case A, Deaton A. Rising morbidity and mortality in midlife among white non-Hispanic Americans in the 21st century. Proc Natl Acad Sci USA. 2015;112:15078–15083.
Denniston MM, Jiles RB, Drobeniuc J, et al. Chronic hepatitis C virus infection in the United States, National Health and Nutrition Examination Survey 2003 to 2010. Ann Intern Med. 2014;160:293–300.
Armstrong GL, Wasley A, Simard EP, et al. The prevalence of hepatitis C virus infection in the United States, 1999 through 2002. Ann Intern Med. 2006;144:705–714.
Alter MJ, Kruszon-Moran D, Nainan OV, et al. The prevalence of hepatitis C virus infection in the United States, 1988 through 1994. N Engl J Med. 1999;341:556–562.
Morse A, Barritt AS, Jhaveri R. Individual state Hepatitis C data supports expanding screening beyond baby boomers to all adults. Gastroenterology. 2018;154:1850–1851.e2.
Barritt AS, Lee B, Runge T, et al. Increasing prevalence of hepatitis c among hospitalized children is associated with an increase in substance abuse. J Pediatr. 2018;192:159–164.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant conflicts to disclose.
Appendix 1: Additional Cirrhosis-Related ICD-9 Codes Used
Appendix 1: Additional Cirrhosis-Related ICD-9 Codes Used
-
1.
Alcoholic cirrhosis: 5712
-
2.
Nonalcoholic cirrhosis: 5715
-
3.
Biliary cirrhosis: 5716
-
4.
Variceal hemorrhage: 4560, 53082, 53140, 53240, 5789, 5780
-
5.
Encephalopathy: 5722
-
6.
Ascites: 7895, 78951, 78959
-
7.
Portal hypertension: 5723
-
8.
Sepsis: 99591
-
9.
Hepatorenal syndrome: 5724
-
10.
Hepatocellular carcinoma (HCC): 1550
-
11.
Hepatitis B (HBV): 07020-3, 07030-3, 07042
-
12.
Hepatitis C (HCV): 07041, 07044, 07054
-
13.
Acute Kidney Injury (AKI): 5845-9
-
14.
Liver transplant: 505, 5051, 5059, V427 (or procedure codes 5051, 5059, 505, 0091, 0092, 0093)
-
15.
Alcoholic hepatitis: 5711
-
16.
Acute pancreatitis: 5770
-
17.
Chronic pancreatitis: 5771
-
18.
Primary Sclerosing cholangitis (PSC): 5761
-
19.
Primary Biliary Cirrhosis/Cholangitis (PBC): 5716
-
20.
Spontaneous Bacterial Peritonitis (SBP): 56723, 567, 5672, 5678, 5679
-
21.
Transfusion: 9904, 9905, 9907
-
22.
Esophagogastroduodenoscopy (EGD): 4513, 4233, 4516, 4443
-
23.
Paracentesis: 5491
-
24.
Thoracentesis: 3491
-
25.
Trans-jugular intrahepatic portosystemic shunt (TIPS): 391
-
26.
Hemodialysis: 3995
-
27.
Mechanical ventilation > 96 h: 9672
-
28.
Alcohol detoxification: 9462
Rights and permissions
About this article

Cite this article
Barritt, A.S., Jiang, Y., Schmidt, M. et al. Charges for Alcoholic Cirrhosis Exceed All Other Etiologies of Cirrhosis Combined: A National and State Inpatient Survey Analysis. Dig Dis Sci 64, 1460–1469 (2019). https://doi.org/10.1007/s10620-019-5471-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-019-5471-7