
Abstract
Introduction
Patients hospitalized for cirrhosis are at high risk for readmission and death for the first 30 days following discharge. However, there is no information on how these risks dynamically change over a full year after discharge. Our aim was to determine the absolute risks of first readmission and death and characterize these changes in the first year following hospital discharge.
Methods
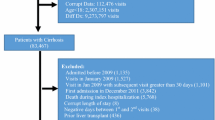
We conducted a retrospective cohort study of patients who were hospitalized with cirrhosis at all Veterans Affairs hospitals and discharged home between 01/01/2010 and 12/31/2013. We used separate survival models to determine risk of first readmission and death after hospital discharge. We also examined the absolute daily risks for first readmission and death by day and identified the time required for risks of readmission and death to decline 50% and 75% from maximum values.
Results
Of the 38,955 patients who survived index hospitalization for cirrhosis, 23,318 patients (59.9%) had at least one readmission and 11,567 patients (29.7%) died within the first year. Daily risk of readmission was the highest on day 1 (1.23%) and declined 50% by day 71 and 75% by day 260. After 1 year, daily risk of readmission did not plateau. Daily risk of death was the highest on day 1 (0.78%) and declined 50% by day 31 and 75% by day 64.
Conclusion
The risk of readmission and death after cirrhosis-related hospitalization remains elevated for prolonged periods. Patients and providers should remain vigilant for clinical health deterioration beyond the first 30 days following hospitalization.



Similar content being viewed by others


References
Tapper EB, Halbert B, Mellinger J. Rates of and reasons for hospital readmissions in patients with cirrhosis: a multistate population-based cohort study. Clin. Gastroenterol. Hepatol. 2016;14:1181–1188.e2.
Roberts SE, Goldacre MJ, Yeates D. Trends in mortality after hospital admission for liver cirrhosis in an English population from 1968 to 1999. Gut. 2005;54:1615–1621. https://doi.org/10.1136/gut.2004.058636.
Sohn M-W, Arnold N, Maynard C, Hynes DM. Accuracy and completeness of mortality data in the Department of Veterans Affairs. Popul. Health Metr. 2006;4:2. https://doi.org/10.1186/1478-7954-4-2.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 1992;45:613–619.
Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J. Am. Stat. Assoc. 1999;94:496–509. https://doi.org/10.1080/01621459.1999.10474144.
Rothman KJ. Epidemiology: An Introduction. Oxford: Oxford University Press; 2012.
Hamada C. Bootstrap Cox regression using SAS procedures. http://www.sascommunity.org/sugi/SUGI95/Sugi-95-211HamadaKishimoto.pdf.
Efron B, Tibshirani R. An Introduction to the Bootstrap. Boca Raton: Chapman & Hall; 1994.
Altman DG, Andersen PK. Bootstrap investigation of the stability of a Cox regression model. Stat. Med. 1989;8:771–783.
Schmidt ML, Barritt AS, Orman ES, Hayashi PH. Decreasing mortality among patients hospitalized with cirrhosis in the United States from 2002 through 2010. Gastroenterology. 2015;148:967–977.e2.
Meier SK, Shah ND, Talwalkar JA. Adapting the patient-centered specialty practice model for populations with cirrhosis. Clin. Gastroenterol. Hepatol. 2016;14:492–496.
Nuti SV, Qin L, Rumsfeld JS, et al. Association of admission to Veterans Affairs hospitals vs non-Veterans Affairs hospitals with mortality and readmission rates among older men hospitalized with acute myocardial infarction, heart failure, or pneumonia. JAMA. 2016;315:582.
Myers RP, Papay KD, Shaheen AAM, Kaplan GG. Relationship between hospital volume and outcomes of esophageal variceal bleeding in the United States. Clin. Gastroenterol. Hepatol. 2008;6:789–798.
Orman ES, Ghabril M, Chalasani N. Poor performance status is associated with increased mortality in patients with cirrhosis. Clin. Gastroenterol. Hepatol. 2016;14:1189–1195.e1.
Kramer JR, Davila JA, Miller ED, Richardson P, Giordono TP, El-Serag HB. The validity of viral hepatitis and chronic liver disease diagnoses in Veterans Affairs administrative databases. Aliment. Pharmacol. Ther. 2007;27:274–282.
Acknowledgments
Aylin Tansel is supported by NIH T-32 5T32DK083266-07 Grant.
Author’s contribution
Aylin Tansel conceived and designed the study, acquired the data, interpreted the data, and wrote the manuscript; Jennifer Kramer conceived and designed the study, interpreted the data, and critically revised the manuscript for important intellectual content; Hua Feng acquired the data, analyzed the data, interpreted the data, and critically revised the manuscript for important intellectual content; Hashem El-Serag interpreted the data and critically revised the manuscript for important intellectual content; and Fasiha Kanwal conceived and designed the study, acquired the data, interpreted the data, critically revised the manuscript for important intellectual content, and supervised the study. All authors approved the final version of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No conflict of interest to declare.
Additional information
Guarantor: Fasiha Kanwal.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Tansel, A., Kramer, J., Feng, H. et al. Risk Trajectories for Readmission and Death After Cirrhosis-Related Hospitalization. Dig Dis Sci 64, 1470–1477 (2019). https://doi.org/10.1007/s10620-019-5459-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-019-5459-3