
Abstract
Background
The phenotypic expression of Crohn’s disease may vary over time. Establishment of Crohn’s disease phenotypes is important for definition of patient care strategies.
Aims
The aim of the study was to evaluate the long-term evolution of patients based on disease phenotypes and the main factors associated with this evolution.
Methods
Data from 179 patients were collected from a unicentric prospective database. Montreal classification was employed. Kaplan–Meier method was used to estimate the cumulative probability of complication development and surgery. Poisson regression for multivariate analysis was applied. The Local Institutional Review Board approved the research.
Results
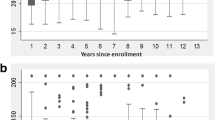
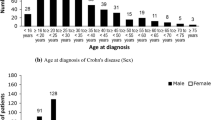
Female: 54.2%. Mean age at diagnosis: 32.7 (±13.7) years. Behavior at presentation: inflammatory 62.0%, stricturing 24.6%, penetrating 13.4%; perianal disease: 31.8%; median follow-up time: 65.2 months (IQR 31.0–108.8). Behavior at follow-up period end: inflammatory 43.6%, stricturing 38.0%, penetrating 18.4%; perianal disease: 46.4%. Cumulative probability of being complication free in 5, 10, and 20 years: 86.3, 66.4, and 52.2%, respectively. Cumulative probability of being surgery free in 5, 10, and 20 years: 87.3, 79.2, and 64.1%, respectively. L1 and L4 locations, use of immunosuppressive therapy, smoking, number of hospitalization/patient-year, abdominal surgery, age at diagnosis <40 years, and biological therapy were the factors associated with changes in phenotype or development of complications and perianal disease.
Conclusion
Clinical behavior altered in about one-third of patients. The most frequent complication was a change to stricturing pattern. Disease location, current smoker, immunosuppressive therapy use, hospitalization, and abdominal surgery were factors associated with an unfavorable clinical evolution.





Similar content being viewed by others

References
Cosnes J, Cattan S, Blain A, et al. Long-term evolution of disease behavior of Crohn’s disease. Inflamm Bowel Dis. 2002;8:244–250.
Cosnes J, Bourrier A, Nion-Larmurier I, Sokol H, Beaugerie L, Seksik P. Factors affecting outcomes in Crohn’s disease over 15 years. Gut. 2012;61:1140–1145.
Freeman HJ. Natural history and clinical behavior of Crohn’s disease extending beyond two decades. J Clin Gastroenterol. 2003;37:216–219.
Louis E, Collard A, Oger AF, Degroote E, Aboul Nasr El Yafi FA, Belaiche J. Behaviour of Crohn’s disease according to the Vienna classification: changing pattern over the course of the disease. Gut. 2001;49:777–782.
Nos P, Garrigues V, Bastida G, Maroto N, Ponce M, Ponce J. Outcome of patients with nonstenotic, nonfistulizing Crohn’s disease. Dig Dis Sci. 2004;49:1771–1776. doi:10.1007/s10620-004-9568-1.
Thia KT, Sandborn WJ, Harmsen WS, Zinsmeister AR, Loftus EV Jr. Risk factors associated with progression to intestinal complications of Crohn’s disease in a population-based cohort. Gastroenterology. 2010;139:1147–1155.
Chow DK, Leong RW, Lai LH. Changes in Crohn’s disease phenotype over time in the Chinese population: validation of the Montreal classification system. Inflamm Bowel Dis. 2008;14:536–541.
Henriksen M, Jahnsen J, Lygren I. Clinical course in Crohn’s disease: results of a five-year population-based follow-up study (the IBSEN study). Scand J Gastroenterol. 2007;42:602–610.
Solberg IC, Vatn MH, Høie O, et al. Clinical course in Crohn’s disease: results of a Norwegian population-based ten-year follow-up study. Clin Gastroenterol Hepatol. 2007;5:1430–1438.
Baumgart DC, Sandborn WJ. Crohn’s disease. Lancet. 2012;380:1590–1605.
Sartor RB. Mechanisms of disease: pathogenesis of Crohn’s disease and ulcerative colitis. Nat Clin Pract Gastroenterol Hepatol. 2006;3:390–407.
Satsangi J, Silverberg MS, Vermeire S, Colombel JF. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut. 2006;55:749–753.
Silverberg MS, Satsangi J, Ahmad T, et al. Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: report of a Working Party of the 2005 Montreal World Congress of Gastroenterology. Can J Gastroenterol. 2005;19 Suppl A:5A–36A.
Parente JM, Coy CS, Campelo V, et al. Inflammatory bowel disease in an underdeveloped region of Northeastern Brazil. World J Gastroenterol. 2015;21:1197–1206.
Santana GO, Lyra LG, Santana TC, et al. Crohn’s disease in one mixed-race population in Brazil. World J Gastroenterol. 2007;13:4489–4492.
Torres Udos S, Rodrigues JO, Junqueira MS, Uezato S, Netinho JG. The Montreal classification for Crohn’s disease: clinical application to a Brazilian single-center cohort of 90 consecutive patients. Arq Gastroenterol. 2010;47:279–284.
Tarrant KM, Barclay ML, Frampton CM, Gearry RB. Perianal disease predicts changes in Crohn’s disease phenotype-results of a population-based study of inflammatory bowel disease phenotype. Am J Gastroenterol. 2008;103:3082–3093.
Prideaux L, Kamm MA, De Cruz PP, Chan FK, Ng SC. Inflammatory bowel disease in Asia: a systematic review. J Gastroenterol Hepatol. 2012;27:1266–1280.
Louis E, Michel V, Hugot JP, et al. Early development of stricturing or penetrating pattern in Crohn’s disease is influenced by disease location, number of flares, and smoking but not by NOD2/CARD15 genotype. Gut. 2003;52:552–557.
Veloso FT, Ferreira JT, Barros L, Almeida S. Clinical outcome of Crohn’s disease: analysis according to the Vienna classification and clinical activity. Inflamm Bowel Dis. 2001;7:306–313.
Magro F, Portela F, Lago P, et al. Crohn’s disease in a southern European country: Montreal classification and clinical activity. Inflamm Bowel Dis. 2009;15:1343–1350.
Santana GO, Souza LR, Azevedo M, Sá AC, Bastos CM, Lyra AC. Application of the Vienna classification for Crohn’s disease to a single center from Brazil. Arq Gastroenterol. 2008;45:64–68.
Romberg-Camps MJ, Dagnelie PC, Kester AD, et al. Influence of phenotype at diagnosis and of other potential prognostic factors on the course of inflammatory bowel disease. Am J Gastroenterol. 2009;104:371–383.
Eglinton TW, Roberts R, Pearson J, et al. Clinical and genetic risk factors for perianal Crohn’s disease in a population-based cohort. Am J Gastroenterol. 2012;107:589–596.
Sands BE, Arsenault JE, Rosen MJ, et al. Risk of early surgery for Crohn’s disease: implications for early treatment strategies. Am J Gastroenterol. 2003;98:2712–2718.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
de Barros, K.S.C., Flores, C., Harlacher, L. et al. Evolution of Clinical Behavior in Crohn’s Disease: Factors Associated with Complicated Disease and Surgery. Dig Dis Sci 62, 2481–2488 (2017). https://doi.org/10.1007/s10620-017-4685-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-017-4685-9