
Abstract
Background
Adherence to post-polypectomy surveillance guideline recommendations is suboptimal. Surveillance is frequently over- and under-recommend, resulting in strained colonoscopy capacity, potential risks without expected benefits, and missed opportunities for colorectal cancer risk reduction.
Aims
To identify factors associated with adherence to post-polypectomy surveillance guidelines.
Methods
We conducted a three-phase study with a retrospective review of usual care post-polypectomy surveillance recommendations through medical chart abstraction (Phase I), prospective online physician survey (Phase II), and analysis of survey-based and other physician-based predictors of usual care surveillance recommendations (Phase III). Subjects included patients who underwent usual care colonoscopy 2011–2012 (Phases I and III) and gastroenterology (GI) attendings and fellows (Phases II and III). We identified rates of recommendations consistent with guideline adherence, surveillance overuse, and surveillance underuse based on usual care medical chart documentation and physician survey, as well as predictors of physician adherence to guidelines.
Results
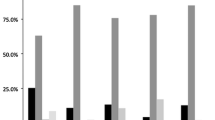
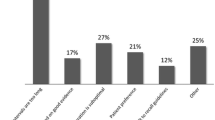
We reviewed 640 patient charts for 28 survey respondents. Rates of usual practice recommendations consistent with guideline adherence, surveillance overutilization, and underutilization were 84, 13, and 3 %, respectively. At survey, 82 % of physicians were concerned about missed cancer. Eleven percentage believed that guidelines were not aggressive enough. GI trainees were 2.5 times more likely to issue guideline-adherent recommendations [OR 2.5, 95 % CI (1.5–4.2)]. Disagreement with guideline aggressiveness was independently associated with 40 % lower likelihood of adherence [OR 0.6, 95 % CI (0.4–0.8)].
Conclusions
Belief in the appropriate aggressiveness of guidelines and trainee position, but not fear of missed cancer or guideline knowledge, was associated with adherence to post-polypectomy surveillance guidelines.



Similar content being viewed by others

References
Schoen RE, Pinsky PF, Weissfeld JL, et al. Utilization of surveillance colonoscopy in community practice. Gastroenterology. 2010;138:73–81.
Laiyemo AO, Pinsky PF, Marcus PM, et al. Utilization and yield of surveillance colonoscopy in the continued follow-up study of the polyp prevention trial. Clin Gastroenterol Hepatol. 2009;7:562–567; quiz 497.
van Heijningen EM, Lansdorp-Vogelaar I, Steyerberg EW, et al. Adherence to surveillance guidelines after removal of colorectal adenomas: a large, community-based study. Gut. 2015. doi:10.1136/gutjnl-2013-306453.
Mysliwiec PA, Brown ML, Klabunde CN, et al. Are physicians doing too much colonoscopy? A national survey of colorectal surveillance after polypectomy. Ann Intern Med. 2004;141:264–271.
Pohl H, Srivastava A, Bensen SP, et al. Incomplete polyp resection during colonoscopy-results of the complete adenoma resection (CARE) study. Gastroenterology. 2013;144:74 e1–80 e1.
Pabby A, Schoen RE, Weissfeld JL, et al. Analysis of colorectal cancer occurrence during surveillance colonoscopy in the dietary Polyp Prevention Trial. Gastrointest Endosc. 2005;61:385–391.
Farrar WD, Sawhney MS, Nelson DB, et al. Colorectal cancers found after a complete colonoscopy. Clin Gastroenterol Hepatol. 2006;4:1259–1264.
Ransohoff DF. Economic impact of surveillance. Gastrointest Endosc. 1999;49:S67–S71.
Sint Nicolaas J, de Jonge V, van Baalen O, et al. Optimal resource allocation in colonoscopy: timing of follow-up colonoscopies in relation to adenoma detection rates. Endoscopy. 2013;45:545–552.
Menees SB, Elliott E, Govani S, et al. Adherence to recommended intervals for surveillance colonoscopy in average-risk patients with 1 to 2 small (<1 cm) polyps on screening colonoscopy. Gastrointest Endosc. 2014;79:551–557.
Shah TU, Voils CI, McNeil R, et al. Understanding gastroenterologist adherence to polyp surveillance guidelines. Am J Gastroenterol. 2012;107:1283–1287.
Saini SD, Nayak RS, Kuhn L, et al. Why don’t gastroenterologists follow colon polyp surveillance guidelines? Results of a national survey. J Clin Gastroenterol. 2009;43:554–558.
CMS. CMS proposes hospital outpatient and ambulatory surgical centers policy and payment changes for 2014 Fact Sheets. 2013, July 8 ed, 2013.
Rex DK, Kahi CJ, Levin B, et al. Guidelines for colonoscopy surveillance after cancer resection: a consensus update by the American Cancer Society and the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2006;130:1865–1871.
Winawer SJ, Zauber AG, Fletcher RH, et al. Guidelines for colonoscopy surveillance after polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer and the American Cancer Society. CA Cancer J Clin. 2006;56:143–159; quiz 184–185.
Lieberman DA, Rex DK, Winawer SJ, et al. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012;143:844–857.
Lieberman DA, Weiss DG, Harford WV, et al. Five-year colon surveillance after screening colonoscopy. Gastroenterology. 2007;133:1077–1085.
Laiyemo AO, Murphy G, Albert PS, et al. Postpolypectomy colonoscopy surveillance guidelines: predictive accuracy for advanced adenoma at 4 years. Ann Intern Med. 2008;148:419–426.
Martinez ME, Baron JA, Lieberman DA, et al. A pooled analysis of advanced colorectal neoplasia diagnoses after colonoscopic polypectomy. Gastroenterology. 2009;136:832–841.
Pinsky PF, Schoen RE, Weissfeld JL, et al. The yield of surveillance colonoscopy by adenoma history and time to examination. Clin Gastroenterol Hepatol. 2009;7:86–92.
Ransohoff DF, Yankaskas B, Gizlice Z, et al. Recommendations for post-polypectomy surveillance in community practice. Dig Dis Sci. 2011;56:2623–2630.
le Clercq CM, Bouwens MW, Rondagh EJ, et al. Postcolonoscopy colorectal cancers are preventable: a population-based study. Gut. 2014;63:957–963.
Acknowledgments
The project described was supported in part by Merit Review Award number 1 I01 HX001574-01A1 (Gupta, PI) from the United States Department of Veterans Affairs Health Services Research & Development Service of the VA Office of Research and Development. The views expressed in this article are those of the author(s) and do not necessarily represent the views of the Department of Veterans Affairs. Support was also provided in part by the NCI-funded consortium Population-Based Research Optimizing Screening through Personalized Regiments (PROSPR) through NIH/NCI Grant U54CA163308-01 (Singal, CO-I). We thank Drs. Kenneth R. McQuaid, Robert H. Lee, and John E. Pandolfino for reviewing and providing feedback on the physician survey.
Conflict of interest
The authors have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Patel, N., Tong, L., Ahn, C. et al. Post-polypectomy Guideline Adherence: Importance of Belief in Guidelines, Not Guideline Knowledge or Fear of Missed Cancer. Dig Dis Sci 60, 2937–2945 (2015). https://doi.org/10.1007/s10620-015-3685-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-015-3685-x