
Abstract
Background
Patients with active upper gastrointestinal bleeding (UGIB) require urgent endoscopy, but appropriate criteria for urgent endoscopy in these patients have not yet been established.
Aims
The goal of this study is to establish a simple system for the selection of UGIB patients who may benefit from urgent endoscopy.
Methods
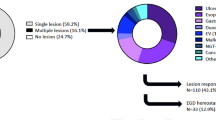
Of the 335 patients who required emergency hospitalization for UGIB from May 2010 to March 2012 at Nagoya Daini Red Cross Hospital, 166 patients who underwent placement of a nasogastric tube (NGT) were retrospectively identified. Active bleeding on the endoscopic image was used as an endpoint that reflected the need for urgent endoscopy.
Results
The ratio of the heart rate to the systolic blood pressure (HR/SBP ratio) and aspiration of fresh or dark red fluid from the NGT [NGT(+)] were significant predictors of active bleeding in the univariate analysis [HR/SBP ratio, P = 0.016; NGT(+), P < 0.001]. The HR/SBP ratio [odds ratio (OR) 8.118; 95 % confidence intervals (CI) 1.696–38.850; P = 0.009] and NGT(+) (OR 4.630; 95 % CI 2.092–10.204; P < 0.001) were also significantly associated with active bleeding in the multivariate analysis. Moreover, receiver operating characteristic analysis revealed a setting with HR/SBP ratio >1.4 or NGT(+) to be optimal criteria to predict active bleeding. These criteria were associated with a sensitivity of 64.9 % (24/37) and a specificity of 76.7 % (99/129) for the prediction of active bleeding; consequently, they are superior to the sensitivity and specificity of previously proposed criteria.
Conclusions
A novel and simple criteria system using NGT(+) and HR/SBP is a good predictor of the need for urgent endoscopy in patients with nonvariceal UGIB.


Similar content being viewed by others


References
Targownik LE, Nabalamba A. Trends in management and outcomes of acute nonvariceal upper gastrointestinal bleeding: 1993–2003. Clin Gastroenterol Hepatol. 2006;4:1459–1466.
van Leerdam ME, Vreeburg EM, Rauws EA, et al. Acute upper GI bleeding: did anything change? Time trend analysis of incidence and outcome of acute upper GI bleeding between 1993/1994 and 2000. Am J Gastroenterol. 2003;98:1494–1499.
Hearnshaw SA, Logan RF, Lowe D, et al. Acute upper gastrointestinal bleeding in the UK: patient characteristics, diagnoses and outcomes in the 2007 UK audit. Gut. 2011;60:1327–1335.
Lau JY, Sung JJ, Lam YH, et al. Endoscopic retreatment compared with surgery in patients with recurrent bleeding after initial endoscopic control of bleeding ulcers. N Engl J Med. 1999;340:751–756.
Wong TC, Wong KT, Chiu PW, et al. A comparison of angiographic embolization with surgery after failed endoscopic hemostasis to bleeding peptic ulcers. Gastrointest Endosc. 2011;73:900–908.
Barkun AN, Bardou M, Kuipers EJ, et al. International consensus recommendations on the management of patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med. 2010;152:101–113.
Chen IC, Hung MS, Chiu TF, et al. Risk scoring systems to predict need for clinical intervention for patients with nonvariceal upper gastrointestinal tract bleeding. Am J Emerg Med. 2007;25:774–779.
Blatchford O, Murray WR, Blatchford M. A risk score to predict need for treatment for upper-gastrointestinal haemorrhage. Lancet. 2000;356:1318–1321.
Chak A, Cooper GS, Lloyd LE, et al. Effectiveness of endoscopy in patients admitted to the intensive care unit with upper GI hemorrhage. Gastrointest Endosc. 2001;53:6–13.
Spiegel BM, Vakil NB, Ofman JJ. Endoscopy for acute nonvariceal upper gastrointestinal tract hemorrhage: is sooner better? A systematic review. Arch Intern Med. 2001;161:1393–1404.
Lee JG, Turnipseed S, Romano PS, et al. Endoscopy-based triage significantly reduces hospitalization rates and costs of treating upper GI bleeding: a randomized controlled trial. Gastrointest Endosc. 1999;50:755–761.
Cook DJ, Guyatt GH, Salena BJ, et al. Endoscopic therapy for acute nonvariceal upper gastrointestinal hemorrhage: a meta-analysis. Gastroenterology. 1992;102:139–148.
Sacks HS, Chalmers TC, Blum AL, et al. Endoscopic hemostasis. An effective therapy for bleeding peptic ulcers. JAMA. 1990;264:494–499.
Bjorkman DJ, Zaman A, Fennerty MB, et al. Urgent vs. elective endoscopy for acute non-variceal upper-GI bleeding: an effectiveness study. Gastrointest Endosc. 2004;60:1–8.
Lin HJ, Wang K, Perng CL, et al. Early or delayed endoscopy for patients with peptic ulcer bleeding. A prospective randomized study. J Clin Gastroenterol. 1996;22:267–271.
Tai CM, Huang SP, Wang HP, et al. High-risk ED patients with nonvariceal upper gastrointestinal hemorrhage undergoing emergency or urgent endoscopy: a retrospective analysis. Am J Emerg Med. 2007;25:273–278.
Jairath V, Kahan BC, Logan RF, et al. Outcomes following acute nonvariceal upper gastrointestinal bleeding in relation to time to endoscopy: results from a nationwide study. Endoscopy. 2012;44:723–730.
Sarin N, Monga N, Adams PC. Time to endoscopy and outcomes in upper gastrointestinal bleeding. Can J Gastroenterol. 2009;23:489–493.
Lim LG, Ho KY, Chan YH, et al. Urgent endoscopy is associated with lower mortality in high-risk but not low-risk nonvariceal upper gastrointestinal bleeding. Endoscopy. 2011;43:300–306.
Aljebreen AM, Fallone CA, Barkun AN. Nasogastric aspirate predicts high-risk endoscopic lesions in patients with acute upper-GI bleeding. Gastrointest Endosc. 2004;59:172–178.
Huang ES, Karsan S, Kanwal F, et al. Impact of nasogastric lavage on outcomes in acute GI bleeding. Gastrointest Endosc. 2011;74:971–980.
Cuellar RE, Gavaler JS, Alexander JA, et al. Gastrointestinal tract hemorrhage. The value of a nasogastric aspirate. Arch Intern Med. 1990;150:1381–1384.
Rockall TA, Logan RF, Devlin HB, et al. Risk assessment after acute upper gastrointestinal haemorrhage. Gut. 1996;38:316–321.
Adamopoulos AB, Baibas NM, Efstathiou SP, et al. Differentiation between patients with acute upper gastrointestinal bleeding who need early urgent upper gastrointestinal endoscopy and those who do not. A prospective study. Eur J Gastroenterol Hepatol. 2003;15:381–387.
Heldwein W, Schreiner J, Pedrazzoli J, et al. Is the Forrest classification a useful tool for planning endoscopic therapy of bleeding peptic ulcers? Endoscopy. 1989;21:258–262.
Tham TC, James C, Kelly M. Predicting outcome of acute non-variceal upper gastrointestinal haemorrhage without endoscopy using the clinical Rockall Score. Postgrad Med J. 2006;82:757–759.
Attar A, Sebbagh V, Vicaut E, et al. Urgent endoscopy in severe non-variceal upper gastrointestinal hemorrhage: does the Glasgow-Blatchford score help endoscopists? Scand J Gastroenterol. 2012;8–9:1086–1093.
Pallin DJ, Saltzman JR. Is nasogastric tube lavage in patients with acute upper GI bleeding indicated or antiquated? Gastrointest Endosc. 2011;74:981–984.
Hwang JH, Fisher DA, Ben-Menachem T, et al. The role of endoscopy in the management of acute non-variceal upper GI bleeding. Gastrointest Endosc. 2012;75:1132–1138.
Gilbert DA, Silverstein FE, Tedesco FJ, et al. The national ASGE survey on upper gastrointestinal bleeding. III. Endoscopy in upper gastrointestinal bleeding. Gastrointest Endosc. 1981;27:94–102.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Iwasaki, H., Shimura, T., Yamada, T. et al. Novel Nasogastric Tube-Related Criteria for Urgent Endoscopy in Nonvariceal Upper Gastrointestinal Bleeding. Dig Dis Sci 58, 2564–2571 (2013). https://doi.org/10.1007/s10620-013-2706-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-013-2706-x