
Abstract
Background and Study Aim
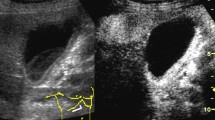
We aimed to assess radial endoscopic ultrasound (EUS) features of the bile duct wall as well as biliary luminal liquid characteristics in cases with acute cholangitis.
Patients and Methods
This prospective study was performed during the period from January 2009 to February 2010 in a tertiary referral center. Twenty-eight patients with acute cholangitis and 60 patients without acute cholangitis but with cholestasis due to gallstone disease were enrolled in the study. During radial EUS examination, sonographic features of the common bile duct wall, the intraductal luminal content, and nearby periductal structures were investigated. Mild hyperechogenic–heterogenic appearances with waving-type movements without acoustic shadowing enclosing one-third of the common bile duct were noted as purulent materials.
Results
EUS indicated an increased focal and/or diffuse concentric bile duct wall thickness (>1.5 mm) in 68 and 27% of the cases with and without acute cholangitis, respectively. The mean bile duct wall thickness was 1.9 mm (0.9–2.9 mm) and 1.1 mm (0.6–2.1 mm) in the study and control groups, respectively (P < 0.05). On EUS, a pericholedochal hypoechoic strand more than 1.5 cm in length was present in 13 of 28 patients with acute cholangitis (46%). It was less than 1 cm long in 11 cases without acute cholangitis (18%). Bile duct content with heterogenous dense echogenicity without acoustic shadowing was present in 18 patients (64%) with acute cholangitis and in two patients (3%) without cholangitis. Those 20 patients were successfully drained with a same-day endoscopic retrograde cholangiography (ERCP) procedure which confirmed purulent biliary content after sphincterotomy. Same-day ERCP revealed no purulent material drainage from the bile duct in the other eight patients without cholangitis. The accuracy and positive and negative predictivity of diffuse concentric wall thickening and a peribiliary hypoechoic strand of greater than 1.5 cm in length for a diagnosis of acute cholangitis were 91, 86.3, and 67.1%, and 76, 72, and 54%, respectively. For purulent material, the accuracy and positive and negative predictive values of EUS for acute cholangitis were noted to be 87, 93.3, and 82%, respectively.
Conclusion
Through this study, it was concluded that EUS findings such as diffuse and/or concentric wall thickening of more than 1.5 mm and intraductal heterogenous echogenicity without acoustic shadowing are highly accurate and predictive for diagnosing acute cholangitis.


Similar content being viewed by others


References
Agarwal N, Sharma BC, Sarin SK. Endoscopic management of acute cholangitis in elderly patients. World J Gastroenterol. 2006;12:6551–6555.
Gallix BP, Aufort S, Pierredon MA, et al. Acute cholangitis: Imaging diagnosis and management. J Radiol. 2006;87:430–440.
Lee JG. Diagnosis and management of acute cholangitis. Nat Rev Gastroenterol Hepatol. 2009;6:533–541.
Yusuf TE, Bhutani MS. Role of endoscopic ultrasonography in diseases of the extrahepatic biliary system. J Gastroenterol Hepatol. 2004;19:243–250.
Nagino M, Takada T, Kawarada Y, et al. Methods and timing of biliary drainage for acute cholangitis: Tokyo Guidelines. J Hepatobiliary Pancreat Surg. 2007;14:68–77.
Tsujino T, Sugita R, Yoshida H, et al. Risk factors for acute suppurative cholangitis caused by bile duct stones. Eur J Gastroenterol Hepatol. 2007;19:585–588.
Chau EM, Leong LL, Chan FL. Recurrent pyogenic cholangitis: Ultrasound evaluation compared with endoscopic retrograde cholangiopancreatography. Clin Radiol. 1987;38:79–85.
Watanabe Y, Nagayama M, Okumura A, et al. MR imaging of acute biliary disorders. Radiographics. 2007;27:477–495.
Bilgin M, Shaikh F, Semelka RC, et al. Magnetic resonance imaging of gallbladder and biliary system. Top Magn Reson Imaging. 2009;20:31–42.
Yeh BM, Liu PS, Soto JA, et al. MR imaging and CT of the biliary tract. Radiographics. 2009;29:1669–1688.
Aljebreen A, Azzam N, Eloubeidi MA. Prospective study of endoscopic ultrasound performance in suspected choledocholithiasis. J Gastroenterol Hepatol. 2008;23:741–745.
Petrov MS, Savides TJ. Systematic review of endoscopic ultrasonography versus endoscopic retrograde cholangiopancreatography for suspected choledocholithiasis. Br J Surg. 2009;96:967–974.
Schulte SJ, Baron RL, Teefey SA, et al. CT of the extrahepatic bile ducts: Wall thickness and contrast enhancement in normal and abnormal ducts. AJR Am J Roentgenol. 1990;154:79–85.
Kikuchi Y, Tsuyuguchi T, Saisho H. Evaluation of normal bile duct and cholangitis by intraductal ultrasonography. Abdom Imaging. 2008;33:452–456.
Krishna NB, Saripalli S, Safdar R, et al. Intraductal US in evaluation of biliary strictures without a mass lesion on CT scan or magnetic resonance imaging: significance of focal wall thickening and extrinsic compression at the stricture site. Gastrointest Endosc. 2007;66:90–96.
Mesenas S, Vu C, Doig L, et al. Duodenal EUS to identify thickening of the extrahepatic biliary tree wall in primary sclerosing cholangitis. Gastrointest Endosc. 2006;63:403–408.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Alper, E., Unsal, B., Buyrac, Z. et al. Role of Radial Endosonography in the Diagnosis of Acute Cholangitis. Dig Dis Sci 56, 2191–2196 (2011). https://doi.org/10.1007/s10620-010-1552-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-010-1552-3