
Abstract
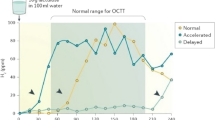
Patients with cystic fibrosis (CF) have recently been deemed highly susceptible for bacterial intestinal overgrowth (BIO). We aimed to define the prevalence of BIO in children with CF by applying the H2-glucose breath test. Forty children with CF and ten healthy children received 1 g/kg D-glucose orally. Breath samples for H2 content (ppm) were collected for 3 h. BIO was suspected if the breath hydrogen content increased by more than 20 ppm or if baseline concentrations topped 20 ppm. In 27 of 40 CF children (68%), breath hydrogen content exceeded 20 ppm. Whereas the breath hydrogen exhalation persisted above 20 ppm in almost all these children throughout the sampling period, none of the remaining children increased above this threshold. The high rate of CF children with elevated fasting hydrogen breath concentrations indicates that this phenomenon is less a sign of BIO rather than a consequence of global malabsorption and intestinal dysmotility.



Similar content being viewed by others

References
Donaldson RM Jr. Small bowel bacterial overgrowth. Adv Intern Med. 1970;16:191–212.
Barbara G, Stanghellini V, Brandi G, et al. Interactions between commensal bacteria and gut sensorimotor function in health and disease. Am J Gastroenterol. 2005;100:2560–2568. doi:10.1111/j.1572-0241.2005.00230.x.
Quigley EM, Quera R. Small intestinal bacterial overgrowth: roles of antibiotics, prebiotics and probiotics. Gastroenterology. 2006;130:S78–S90. doi:10.1053/j.gastro.2005.11.046.
Husebye E. The pathogenesis of gastrointestinal bacterial overgrowth. Chemotherapy. 2005;51(Suppl 1):1–22. doi:10.1159/000081988.
Gunnarsdottir SA, Sadik R, Shev S, et al. Small intestinal motility disturbances and bacterial overgrowth in patients with liver cirrhosis and portal hypertension. Am J Gastroenterol. 2003;98:1362–1370. doi:10.1111/j.1572-0241.2003.07475.x.
Lin HC. Small intestinal bacterial overgrowth. A framework for understanding irritable bowel syndrome. JAMA. 2004;292:852–858. doi:10.1001/jama.292.7.852.
King CE, Toskes PP. Small intestine bacterial overgrowth. Gastroenterology. 1979;76:1035–1055.
Banwell JG, Kistler LA, Giannella RA, Weber FL, Lieber A, Powell DE. Small intestinal bacterial overgrowth syndrome. Gastroenterology. 1981;80:834–845.
Schjonsby H, Hofstad T. The uptake of vitamin B12 by the sediment of jejunal contents in patients with blind loop syndrome. Scand J Gastroenterol. 1975;10:305–309.
Steffen EK, Berg RD, Deitch EA. Comparison of translocation rates of various indigenous bacteria from the gastrointestinal tract to the mesenteric lymph node. J Infect Dis. 1988;157:1023–1028.
Riordan SM, McIver CJ, Wakefield D, Thomas MC, Dunscombe VM, Bolin TD. Serum immunoglobulin and soluble IL-2 receptor levels in small intestinal bacterial overgrowth with indigenous gut flora. Dig Dis Sci. 1999;44:939–944. doi:10.1023/A:1026652412554.
Bjorneklett A, Fausa O, Midtvedt T. Small-bowel bacterial overgrowth in the postgastrectomy syndrome. Scand J Gastroenterol. 1983;18:277–287.
Walters B, Vanner SJ. Detection of bacterial overgrowth in IBS using the lactulose H2 breath test: comparison with 14C-D-xylose and healthy controls. Am J Gastroenterol. 2005;100:1566–1570. doi:10.1111/j.1572-0241.2005.40795.x.
Pimentel M, Chow EJ, Lin HC. Eradication of small intestinal bacterial overgrowth reduces symptomas of irritable bowel syndrome. Am J Gastroenterol. 2000;95:3503–3506. doi:10.1111/j.1572-0241.2000.03368.x.
Lewindon PJ, Robb TA, Moore DJ, Davidson GP, Martin AJ. Bowel dysfunction in cystic fibrosis: importance of breath testing. J Paediatr Child Health. 1998;34:79–82. doi:10.1046/j.1440-1754.1998.00159.x.
Fridge JL, Conrad C, Gerson L, Castillo RO, Cox K. Risk factors for small bowel bacterial overgrowth in cystic fibrosis. J Pediatr Gastroenterol Nutr. 2007;44:212–218. doi:10.1097/MPG.0b013e31802c0ceb.
Norkina O, Burnett TG, de Lisle RC. Bacterial overgrowth in the cystic fibrosis transmembrane conductance regulator null mouse small intestine. Infect Immun. 2004;72:6040–6049. doi:10.1128/IAI.72.10.6040-6049.2004.
Kerem E, Conway S, Elborn S, Heijerman H. Consensus committee: standards of care for patients with cystic fibrosis: a European consensus. J Cyst Fibros. 2005;4:7–26. doi:10.1016/j.jcf.2004.12.002.
Kerlin P, Wong L. Breath hydrogen testing in bacterial overgrowth of the small intestine. Gastroenterology. 1988;95:982–988.
King CE, Toskes PP. Comparison of the 1 g [14C]xylose, 10 g lactulose- H2, and 80 g glucose-H2 breath tests in patients with small intestine bacterial overgrowth. Gastroenterology. 1986;91:1447–1451.
King CE, Toskes PP. Breath tests in the diagnosis of small intestine bacterial overgrowth. Crit Rev Clin Lab Sci. 1984;21:269–281.
Corazza G, Sorge M, Strocchi A, Gasbarrini G. Glucose-H2 breath test for small intestine bacterial overgrowth. Gastroenterology. 1990;98:253–254.
Keller J, Franke A, Storr M, et al. Clinically relevant breath tests in gastroenterological diagnostics-recommendations of the German Society for Neurogastroenterology and Motility as well as the German Society for Digestive and Metabolic Diseases. Z Gastroenterol. 2005;43:1071–1090. doi:10.1055/s-2005-858479.
Norkina O, Kaur S, Ziemer D, De Lisle RC. Inflammation of the cystic fibrosis mouse small intestine. Am J Physiol Gastrointest Liver Physiol. 2004;286:G1032–G1041. doi:10.1152/ajpgi.00473.2003.
De Lisle RC, Roach EA, Norkina O. Eradication of small intestinal bacterial overgrowth in the cystic fibrosis mouse reduces mucus accumulation. J Pediatr Gastroenterol Nutr. 2006;42:46–52. doi:10.1097/01.mpg.0000189322.34582.3e.
Romagnuolo J, Schiller D, Bailey RJ. Using breath tests wisely in a gastroenterology practice: an evidence-based review of indications and pitfalls in interpretation. Am J Gastroenterol. 2002;97:1113–1126. doi:10.1111/j.1572-0241.2002.05664.x.
Bali A, Stableforth DE, Asquith P. Prolonged small-intestinal transit time in cystic fibrosis. Br Med J (Clin Res Ed). 1983;287:1011–1013.
Gregory PC. Gastrointestinal pH, motility/transit and permeability in cystic fibrosis. J Pediatr Gastroenterol Nutr. 1996;23:513–523. doi:10.1097/00005176-199612000-00001.
Escobar H, Perdomo M, Vasconez F, Camarero C, del Olmo MT, Suarez L. Intestinal permeability to 51Cr-EDTA and orocecal transit time in cystic fibrosis. J Pediatr Gastroenterol Nutr. 1992;14:204–207. doi:10.1097/00005176-199202000-00015.
Dalzell AM, Freestone NS, Billington D, Heaf DP. Small intestinal permeability and orocaecal transit time in cystic fibrosis. Arch Dis Child. 1990;65:585–588.
Acknowledgment
This study was performed without funding from third parties. The authors do not have any disclosures to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schneider, A.R.J., Klueber, S., Posselt, HG. et al. Application of the Glucose Hydrogen Breath Test for the Detection of Bacterial Overgrowth in Patients with Cystic Fibrosis––A Reliable Method?. Dig Dis Sci 54, 1730–1735 (2009). https://doi.org/10.1007/s10620-008-0559-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-008-0559-5