
Abstract
Purpose
We aimed to develop a simple risk score for patients with HFpEF and assessed the efficacy of spironolactone across baseline risk.
Methods
We developed risk stratification scheme for cardiovascular death in placebo arm of the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist trial (TOPCAT). We screened candidate risk indicators and determined strong risk predictors using COX regression. The absolute risk reduction (ARR) in cardiovascular death with spironolactone was evaluated across baseline risk groups. COX regressions were performed to assess the hazard ratios (HRs) of spironolactone therapy for cardiovascular death and drug discontinuation in each risk category.
Results
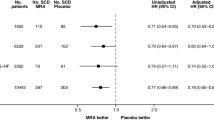
A simple risk score scheme was constructed based on five risk indicators weighted by estimates from the model, including age, diastolic blood pressure, renal dysfunction, white blood cell, and left ventricular ejection fraction. The risk score scheme showed good discrimination in placebo cohort (C index=0.70). ARR with spironolactone therapy was observed only in patients at very high risk (7.9%). Spironolactone therapy significantly reduced the risk of cardiovascular death in the very high-risk group (HR: 0.57; 95%CI, 0.39–0.84; P =0.005 and P for interaction 0.03) but showed similar risk of drug discontinuation across risk categories (P for interaction=0.928).
Conclusion
This simple risk score stratifies patients with HFpEF by their baseline risk of cardiovascular death. Patients at very high risk derive great benefits from spironolactone therapy. This easy-to-use risk score provides a practical tool that can facilitate risk stratification and tailoring therapy for those who benefit most from spironolactone.
Trial Registration
ClinicalTrials.gov Identifier: NCT00094302.


Similar content being viewed by others


Availability of Data and Material
This study used TOPCAT trial data that are available to eligible researchers after registration.
Code Availability
Not applicable
References
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–200.
Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. New Engl J Med. 2006;355:251–9.
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Colvin MM, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2017;70:776–803.
Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B, et al. Spironolactone for heart failure with preserved ejection fraction. New Engl J Med. 2014;370:1383–92.
Cohen JB, Schrauben SJ, Zhao L, Basso MD, Cvijic ME, Li Z, et al. Clinical Phenogroups in Heart Failure With Preserved Ejection Fraction: Detailed Phenotypes, Prognosis, and Response to Spironolactone. JACC Heart Fail. 2020;8:172–84.
Desai AS, Lewis EF, Li R, Solomon SD, Assmann SF, Boineau R, et al. Rationale and design of the treatment of preserved cardiac function heart failure with an aldosterone antagonist trial: a randomized, controlled study of spironolactone in patients with symptomatic heart failure and preserved ejection fraction. Am Heart J. 2011;162:966–972.e10.
Thorvaldsen T, Claggett BL, Shah A, Cheng S, Agarwal SK, Wruck LM, et al. Predicting Risk in Patients Hospitalized for Acute Decompensated Heart Failure and Preserved Ejection Fraction: The Atherosclerosis Risk in Communities Study Heart Failure Community Surveillance. Circ Heart Fail. 2017;10:e003992.
Jones RC, Francis GS, Lauer MS. Predictors of mortality in patients with heart failure and preserved systolic function in the Digitalis Investigation Group trial. J Am Coll Cardiol. 2004;44:1025–9.
Lee DS, Austin PC, Rouleau JL, Liu PP, Naimark D, Tu JV. Predicting mortality among patients hospitalized for heart failure: derivation and validation of a clinical model. JAMA. 2003;290:2581–7.
Pocock SJ, Ariti CA, McMurray JJ, Maggioni A, Køber L, Squire IB, et al. Predicting survival in heart failure: a risk score based on 39 372 patients from 30 studies. Eur Heart J. 2013;34:1404–13.
Kasahara S, Sakata Y, Nochioka K, Tay WT, Claggett BL, Abe R, et al. The 3A3B score: The simple risk score for heart failure with preserved ejection fraction - A report from the CHART-2 Study. Int J Cardiol. 2019;284:42–9.
Wehner GJ, Jing L, Haggerty CM, Suever JD, Leader JB, Hartzel DN, et al. Routinely reported ejection fraction and mortality in clinical practice: where does the nadir of risk lie? Eur Heart J. 2020;41:1249–57.
Jentzer JC, van Diepen S, Barsness GW, Henry TD, Menon V, Rihal CS, et al. Cardiogenic Shock Classification to Predict Mortality in the Cardiac Intensive Care Unit. J Am Coll Cardiol. 2019;74:2117–28.
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62:e147–239.
Bajaj NS, Kalra R, Gupta K, Aryal S, Rajapreyar I, Lloyd SG, et al. Leucocyte count predicts cardiovascular risk in heart failure with preserved ejection fraction: insights from TOPCAT Americas. ESC Heart Fail. 2020;7:1676–87.
Solomon SD, Claggett B, Lewis EF, Desai A, Anand I, Sweitzer NK, et al. Influence of ejection fraction on outcomes and efficacy of spironolactone in patients with heart failure with preserved ejection fraction. Eur Heart J. 2016;37:455–62.
Ramalho SHR, Claggett BL, Sweitzer NK, Fang JC, Shah SJ, Anand IS, et al. Impact of pulmonary disease on the prognosis in heart failure with preserved ejection fraction: the TOPCAT trial. Eur J Heart Fail. 2020;22:557–9.
Agostoni P, Magini A, Andreini D, Contini M, Apostolo A, Bussotti M, et al. Spironolactone improves lung diffusion in chronic heart failure. Eur Heart J. 2005;26:159–64.
Cikes M, Claggett B, Shah AM, Desai AS, Lewis EF, Shah SJ, et al. Atrial Fibrillation in Heart Failure With Preserved Ejection Fraction: The TOPCAT Trial. JACC Heart Fail. 2018;6:689–97.
Anand IS, Claggett B, Liu J, Shah AM, Rector TS, Shah SJ, et al. Interaction Between Spironolactone and Natriuretic Peptides in Patients With Heart Failure and Preserved Ejection Fraction: From the TOPCAT Trial. JACC Heart Fail. 2017;5:241–52.
Elkholey K, Papadimitriou L, Butler J, Thadani U, Stavrakis S. Effect of Obesity on Response to Spironolactone in Patients with Heart Failure with Preserved Ejection Fraction. Am J Cardiol. 2021. https://doi.org/10.1016/j.amjcard.2021.01.018
Zile MR, Baicu CF, Ikonomidis JS, Stroud RE, Nietert PJ, Bradshaw AD, et al. Myocardial stiffness in patients with heart failure and a preserved ejection fraction: contributions of collagen and titin. Circulation. 2015;131:1247–59.
Kasner M, Westermann D, Lopez B, Gaub R, Escher F, Kühl U, et al. Diastolic tissue Doppler indexes correlate with the degree of collagen expression and cross-linking in heart failure and normal ejection fraction. J Am Coll Cardiol. 2011;57:977–85.
Ravassa S, Trippel T, Bach D, Bachran D, González A, López B, et al. Biomarker-based phenotyping of myocardial fibrosis identifies patients with heart failure with preserved ejection fraction resistant to the beneficial effects of spironolactone: results from the Aldo-DHF trial. Eur J Heart Fail. 2018;20:1290–9.
Steiner J, Guglin M. BNP or NTproBNP? A clinician’s perspective. Int J Cardiol. 2008;129:5–14.
Acknowledgements
We thank the staff and participants of the TOPCAT study and ARIC study for their contributions. We express our appreciation to Shuyi Wang, MD, for her generous assistance in manuscript editing.
Funding
This work was supported by the National Natural Science Foundation of China (81600206 to ZXD; 81870195 to LXX) and Natural Science Foundation of Guangdong Province (2016A030310140 to ZXD; 2016A020220007 and 2019A1515011582 to LXX).
Author information
Authors and Affiliations
Contributions
LXX, ZXD, and LYF contributed to the conception or design of the work. All authors were responsible for the acquisition, analysis, and interpretation of data. LYF, ZXB, and ZSZ drafted the manuscript. Critical revision of the manuscript for important intellectual content were performed by all authors. All authors agreed with the content of the article to be submitted.
Corresponding authors
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Ethics Approval
The institutional review board at each participating center approved the study protocol.
Consent to Participate
All patients provided written informed consent.
Consent for Publication
All authors have reviewed and agree with the content of the article for publication.
Disclaimer
The supporting organizations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(PDF 691 kb)
Rights and permissions
About this article

Cite this article
Lin, Y., Zhong, X., Liu, M. et al. Risk Stratification and Efficacy of Spironolactone in Patients with Heart Failure with Preserved Ejection Fraction: Secondary Analysis of the TOPCAT Randomized Clinical Trial. Cardiovasc Drugs Ther 36, 323–331 (2022). https://doi.org/10.1007/s10557-021-07178-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10557-021-07178-y