
Abstract
Background: Non-invasive evaluation of haemodynamic variables remains a preferable and attractive option in both pharmacologic research and clinical cardiology.
Objectives: The objective of this study was to evaluate the correlation, feasibility and diagnostic value of haemodynamic measurements by ICG with the thermodilution (TD) method at rest and during exercise testing.
Methods: We measured stroke volume (SV) and cardiac output (CO) with both methods in 20 patients with suspected coronary artery disease (CAD). All measurements were performed simultaneously at rest and during bicycle exercise.
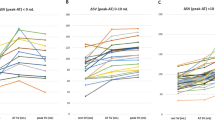
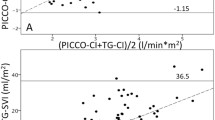
Results: There was a highly significant correlation (p < 0.001) for measurements of SV between both methods at rest (r = 0.83) and during exercise (r = 0.85–0.87) with 50–100 watts. For measurements of CO, the respective correlations were r = 0.85 at rest and r = 0.92–0.94 during exercise. The mean difference for measurements of SV were 3.8 ± 12.6 ml at rest and 6.5± 11.4 ml during exercise. For measurements of CO, the mean difference between both methods was 0.9 ± 1.0 l/min at rest and 1.0± 0.8 l/min during exercise. Compared to TD measurements, ICG had a bias to overestimate SV and CO of approximately by 5–10%. One patient had to be excluded because of inappropriate quality of the ICG signals during exercise.
Conclusions: ICG is a feasible and accurate method for non-invasive measurements of SV and CO. Haemodynamic measurements by ICG were correlated highly significant to simultaneous measurements by the TD method.
Similar content being viewed by others

References
Kubicek WG, Karnegis JN, Patterson RP, Witsoe DA, Mattson RH. Development and evaluation of an impedance cardiography output system. Aerospace Med 1966;37:1208–1212.
Kubicek WG, Kottke FJ, Ramos MU, et al. The Minnesota impedance cardiograph—theory and applications. Biomed Eng 1974;9:410–416.
Sramek BB. Electrical bioimpedance. Med Electron 1983;14:95–103.
Bernstein DP. Continuous noninvasive real-time monitoring of stroke volume and cardiac output by thoracic electrical bioimpedance. Crit Care Med 1986;14:898.
Acton G, Broom C. A comparison of attenuation compensated volume flow based Doppler echocardiography and impedance cardiography in healthy volunteers. Am J Noninvasiv Cardiol 1990;4:290–297.
Breithaupt K, Erb A, Neumann B, Wolf GZ, Belz GG. Comparison of four noninvasiv Techniques to measure stroke volume: Dual-beam Doppler echoaortography, electrical bioimpedance Cardiography, Mechanosphygmography and M-mode echocardiography of the left ventricle. Am J Noninvas Cardiol 1990;4:203–209.
Ng HW, Walley T, Tsao Y, Breckenridge AM. Comparison and reproducibility of transthoracic bioimpedance and dual beam Doppler ultrasound measurement of cardiac function in healthy volunteers. Br J Clin Pharmacol 1991;32:275–282.
Robin ED. Death by pulmonary artery flow-directed catheter: Time for amoratorium? Chest 1987;92:727–31.
Fuller HD. The validity of cardiac output measurement by thoracic impedance: A meta-analysis. Clin Invest Med 1992;15:103–112.
Jensen L, Yakimets J, Teo KK. Issues in cardiovascular care. A review of impedance cardiography. Heart Lung 1995;24:83–93.
Woltjer HH, Bogaard HJ, de Vries PMJM. The technique of impedance cardiography. Eur Heart J 1997;18:1396–1403.
Clancy TV, Norman K, Reynolds R. Cardiac output measurement in critical care patients: Thoracic electrical bioimpedance versus thermodilution. J Trauma 1991;31:1116–1121.
van der Meer M, de Vries P. The reliability and applicability of impedance cardiography in the ICU. Intensivmed 1996:33:495–500.
Spahn DR, Schmid ER, Tornic EM, et al. Noninvasive versus invasive assessment of cardiac output after cardiac surgery: Clinical validation. J Cardiothorac Anesth 1990;4:46–59.
Perrino AC, Lippman A, Ariyan C, O’Connor TZ, Luther M. Intraoperative cardiac output monitoring: Comparison of impedance cardiography and thermodilution. J Cardiothorac Vasc Anesth 1994;8:24–29.
Goldstein DS, Cannon RO, Ziemlichman R, Keiser HR. Clinical evaluation of imdedacne cardiography. Clinical Physiology 1986;6:235–251.
Scherhag A, Pfleger S, de Mey C, Schreckenberger AB, Staedt U, Heene DL. Continuous measurement of hemodynamic alterations during pharmacologic cardiovascular stress using automated impedance cardiography. J Clin Pharmacol 1997;37:21–28.
Teo KK, Hetherington MD, Haennel RG, Greenwood PV, Rossall RE, Kappagoda T. Cardiac output measured by impedance cardiography during maximal exercise tests. Cardiovasc Res 1985;19:737–743.
Thomas SH. Impedance cardiography using the Sramek-Bernstein method: Accuracy and variability at rest and during exercise. Br J Clin Pharmacol 1992;34:467–476.
Belardinelli R, Ciampani N, Costantini C, Blandini A, Purcaro A. Comparison of impedance cardiography with thermodilution and direct Fick methods for noninvasive measurement of stroke volume and cardiac output during incremental exercise in patients with ischemic cardiomyopathy. Am J Cardiol 1996;77:1293–1301.
Charloux A, Lonsdorfer-Wolf E, Richard R, et al. A new impedance cardiograph device for the non-invasive evaluation of cardiac output at rest and during exercise: Comparison with the “direct” Fick method. Eur J Appl Physiol 2000:82:313–320.
Tordi N, Mourot L, Matusheski B, Hughson RL. Measurements of cardiac output during constant exercises: comparison of two non-invasive techniques. Int J Sports Med 2004;25:145–149.
Richard R, Lonsdorfer-Wolf E, Charloux A, et al. Non-invasive cardiac output evaluation during a maximal progressive exercise test, using a new impedance cardiograph device. Eur J Appl Physiol 2001;85:202–207.
Christensen TB, Jensen BV, Hjerpe J, Kanstrup IL. Cardiac outpur measurement by electrical bioimpedance compared with the CO2 rebreathing technique at different levels of exercise. Clin Physiol 200:20:101–105.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;(I):307–310.
Capan LM, Bernstein DP, Patel KP, Sanger J, Turndof H. Measurement of ejection fraction by bioimpedance method. Crit Care Med 1987;15:402.
Salandin V, Zussa C, Risica G, et al. Comparison of cardiac output estimation by thoracic electrical bioimpedance, thermodilution and Fick methods. Crit Care Med 1988;16:1157–1158.
Wong DH, Tremper KK, Stemmer EA, et al. Noninvasive cardiac output: Simultaneous comparison of two different methods with thermodilution. Anesthesiology 1990;72:784–92.
Pickett BR, Buell JC. Validity of Cardiac Output Measurement by Computer-Averaged Impedance Cardiography, and comparison with simultaneous thermodilution determinations. Am J Cardiol 1992;69:1354–1358.
Yung GL, Gedullo PF, Kinninger K, Johnson W, Channick RN. Comparison of impedance cardiography to direct fick and thermodilution cardiac output determination in pulmonary arterial hypertension. CHF 2004;10(2 suppl. 2):7–10.
De Mey C, Enterling D. Noninvasive assessment of cardiac performance by impedance cardiography: disagreement between two equations to estimate stroke volume. Aviat Space Environ Med 1988;59:57–62.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Scherhag, A., Kaden, J.J., Kentschke, E. et al. Comparison of Impedance Cardiography and Thermodilution-Derived Measurements of Stroke Volume and Cardiac Output at Rest and During Exercise Testing. Cardiovasc Drugs Ther 19, 141–147 (2005). https://doi.org/10.1007/s10557-005-1048-0
Issue Date:
DOI: https://doi.org/10.1007/s10557-005-1048-0