
Abstract
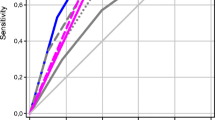
The ankle-brachial index is a commonly used tool for identifying peripheral artery disease for cardiovascular risk stratification. An abnormal ankle-brachial index occurs only following extensive peripheral atherosclerosis occlusion, and thus has poor sensitivity for coronary atherosclerosis. There is a critical need for the development of tools that can detect risk prior to advanced stages of atherosclerosis. We sought to determine the sensitivity of femoral ultrasound for coronary artery disease. In this prospective, cross-sectional study, participants (n = 124) underwent ankle-brachial index measurement and femoral ultrasound for assessment of intima-media thickness, maximal plaque height, and total plaque area following coronary angiography. Receiver operating characteristic areas under the curve were plotted for identifying significant coronary artery disease (≥ 50% stenosis). Logistic regression was utilized to evaluate associations. 64% of participants had significant, angiography-confirmed coronary artery disease. Femoral ultrasound plaque area yielded the highest area under the curve for detecting significant coronary disease (area under the curve = 0.731). In contrast, an abnormal ankle-brachial index (≤ 0.90) produced an area under the curve of 0.568. Femoral ultrasound had a higher sensitivity (85%) than the ankle-brachial index (25%) for ruling out significant coronary artery disease. Both ankle-brachial index and femoral ultrasound have similar capacity to detect peripheral artery disease. Femoral ultrasound has a significantly greater discriminatory power than ankle-brachial index to detect clinically significant coronary artery disease. Ultrasound-captured femoral plaque burden directly delineates the extent of peripheral arterial disease and is better at ruling out significant coronary atherosclerosis than the ankle-brachial index.



Similar content being viewed by others


Data availability
On request.
Abbreviations
- ABI:
-
Ankle-brachial index
- AUC:
-
Area under the curve
- BMI:
-
Body mass index
- CAD:
-
Coronary artery disease
- eGFR:
-
Estimated glomerular filtration rate
- IMT:
-
Intima-media thickness
- PAD:
-
Peripheral arterial disease
- MPH:
-
Maximal plaque height
- ROC:
-
Receiver operating characteristic
- TPA:
-
Total plaque area
References
Nicolaides A, Panayiotou AG (2016) Screening for atherosclerotic cardiovascular risk using ultrasound. J Am Coll Cardiol 67(11):1275–1277
Abbott JD, Lombardero MS, Barsness GW, Pena-Sing I, Buitron LV, Singh P et al (2012) Ankle-brachial index and cardiovascular outcomes in the bypass angioplasty revascularization investigation 2 diabetes trial. Am Heart J 164(4):585-590.e4
Resnick HE, Lindsay RS, McDermott MM, Devereux RB, Jones KL, Fabsitz RR et al (2004) Relationship of high and low ankle brachial index to all-cause and cardiovascular disease mortality: the strong heart study. Circulation 109(6):733–739
Heald CL, Fowkes FG, Murray GD, Price JF, Ankle Brachial Index C (2006) Risk of mortality and cardiovascular disease associated with the ankle-brachial index: systematic review. Atherosclerosis 189(1):61–69
Goff DC Jr, Lloyd-Jones DM, Bennett G, Coady S, D’Agostino RB, Gibbons R et al (2014) 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation 129(25 Suppl 2):S49-73
Anand SS, Bosch J, Eikelboom JW, Connolly SJ, Diaz R, Widimsky P et al (2018) Rivaroxaban with or without aspirin in patients with stable peripheral or carotid artery disease: an international, randomised, double-blind, placebo-controlled trial. Lancet 391(10117):219–229
Papanas N, Tziakas D, Maltezos E, Kekes A, Hatzinikolaou E, Parcharidis G et al (2004) Peripheral arterial occlusive disease as a predictor of the extent of coronary atherosclerosis in patients with coronary artery disease with and without diabetes mellitus. J Int Med Res 32(4):422–428
Sadeghi M, Tavasoli A, Roohafza H, Sarrafzadegan N (2010) The relationship between ankle-brachial index and number of involved coronaries in patients with stable angina. ARYA Atheroscler 6(1):6–10
Flanigan DP, Ballard JL, Robinson D, Galliano M, Blecker G, Harward TR (2008) Duplex ultrasound of the superficial femoral artery is a better screening tool than ankle-brachial index to identify at risk patients with lower extremity atherosclerosis. J Vasc Surg 47(4):789–792
Kafetzakis A, Kochiadakis G, Laliotis A, Peteinarakis I, Touloupakis E, Igoumenidis N et al (2005) Association of subclinical wall changes of carotid, femoral, and popliteal arteries with obstructive coronary artery disease in patients undergoing coronary angiography. Chest 128(4):2538–2543
Yerly P, Marques-Vidal P, Owlya R, Eeckhout E, Kappenberger L, Darioli R et al (2015) The atherosclerosis burden score (ABS): a convenient ultrasound-based score of peripheral atherosclerosis for coronary artery disease prediction. J Cardiovasc Transl Res 8(2):138–147
Colledanchise KN, Mantella LE, Bullen M, Hetu MF, Abunassar JG, Johri AM (2020) Combined femoral and carotid plaque burden identifies obstructive coronary artery disease in women. J Am Soc Echocardiogr 33(1):90–100
Johri AM, Chitty DW, Matangi M, Malik P, Mousavi P, Day A et al (2013) Can carotid bulb plaque assessment rule out significant coronary artery disease? A comparison of plaque quantification by two- and three-dimensional ultrasound. J Am Soc Echocardiogr 26(1):86–95
Maddox TM, Stanislawski MA, Grunwald GK, Bradley SM, Ho PM, Tsai TT et al (2014) Nonobstructive coronary artery disease and risk of myocardial infarction. JAMA 312(17):1754–1763
Touboul PJ, Hennerici MG, Meairs S, Adams H, Amarenco P, Bornstein N et al (2012) Mannheim carotid intima-media thickness and plaque consensus (2004-2006-2011). An update on behalf of the advisory board of the 3rd, 4th and 5th watching the risk symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cerebrovasc Dis 34(4):290–296
Johri AM, Calnan CM, Matangi MF, MacHaalany J, Hetu MF (2016) Focused vascular ultrasound for the assessment of atherosclerosis: a proof-of-concept study. J Am Soc Echocardiogr 29(9):842–849
Johri AM, Behl P, Hétu MF, Haqqi M, Ewart P, Day AG et al (2016) Carotid ultrasound maximum plaque height-a sensitive imaging biomarker for the assessment of significant coronary artery disease. Echocardiography 33(2):281–289
Fowkes FG, Murray GD, Butcher I, Heald CL, Lee RJ, Ankle Brachial Index C et al (2008) Ankle brachial index combined with Framingham risk score to predict cardiovascular events and mortality: a meta-analysis. JAMA 300(2):197–208
Dachun X, Jue L, Liling Z, Yawei X, Dayi H, Pagoto SL et al (2010) Sensitivity and specificity of the ankle–brachial index to diagnose peripheral artery disease: a structured review. Vasc Med 15(5):361–369
Su HM, Voon WC, Lin TH, Lee KT, Chu CS, Lee MY et al (2004) Ankle-brachial pressure index measured using an automated oscillometric method as a predictor of the severity of coronary atherosclerosis in patients with coronary artery disease. Kaohsiung J Med Sci 20(6):268–272
Finn AV, Kolodgie FD, Virmani R (2010) Correlation between carotid intimal/medial thickness and atherosclerosis: a point of view from pathology. Arterioscler Thromb Vasc Biol 30(2):177–181
Acknowledgements
We thank the staff of the Kingston General Hospital Cardiac Catheterization and Vascular Doppler Laboratories for their help and support of this study. We also thank Gopi Krishnan Rajbahadur for assistance in the study. The authors declare that there is no conflict of interest.
Funding
This work was supported by Queen’s University, Kingston, ON, a Canada Foundation for Innovation and Ontario Research Fund (CFI#29051), a Ministry of Research, Innovation and Science Early Research Award (#ER15-11-029 to AMJ), the South Eastern Ontario Academic Medical Organization (Clinician Scientist Development Program to AMJ), the Heart and Stroke Foundation of Canada (Clinician Scientist Phase I #7500 to AMJ), and a Natural Sciences and Engineering Research Council of Canada scholarship to KNC.
Author information
Authors and Affiliations
Contributions
KNC, study design, data collection, analysis and interpretation, manuscript writing; LEM and JGA, data collection and analysis, critical review of manuscript; KL manuscript writing and critical review of the manuscript; MFH study conception and design, ethical clearance, image review, statistical analysis, critical review; and AMJ, study conception and design, supervision, critical review of manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The author declare that they have no conflict of interest.
Ethical approval
This study was approved by Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics board. The investigation conformed to the principles outlined in the Declaration of Helsinki.
Consent to participate
All involved participants provided informed, written consent.
Consent for publication
All authors consent to publication and participants were informed that the results of the study would be used for research and publication.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Colledanchise, K.N., Mantella, L.E., Hétu, MF. et al. Femoral plaque burden by ultrasound is a better indicator of significant coronary artery disease over ankle brachial index. Int J Cardiovasc Imaging 37, 2965–2973 (2021). https://doi.org/10.1007/s10554-021-02334-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-021-02334-9