
Abstract
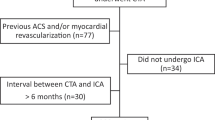
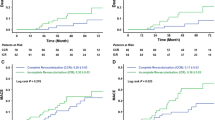
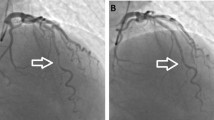
To assess the anatomical background and significance of incomplete invasive coronary angiography (ICA) and to evaluate the value of coronary computed tomography angiography (CTA) in this scenario. The current study is an analysis of high volume center experience with prospective registry of coronary CTA and ICA. The target population was identified through a review of the electronic database. We included consecutive patients referred for coronary CTA after ICA, which did not visualize at least one native coronary artery or by-pass graft. Between January 2009 and April 2013, 13,603 diagnostic ICA were performed. There were 45 (0.3 %) patients referred for coronary CTA after incomplete ICA. Patients were divided into 3 groups: angina symptoms without previous coronary artery by-pass grafting (CABG) (n = 11,212), angina symptoms with previous CABG (n = 986), and patients prior to valvular surgery (n = 925). ICA did not identify by-pass grafts in 21 (2.2 %) patients and in 24 (0.2 %) cases of native arteries. The explanations for an incomplete ICA included: 11 ostium anomalies, 2 left main spasms, 5 access site problems, 5 ascending aorta aneurysms, and 2 tortuous take-off of a subclavian artery. However, in 20 (44 %) patients no specific reason for the incomplete ICA was identified. After coronary CTA revascularization was performed in 11 (24 %) patients: 6 successful repeat ICA and percutaneous intervention and 5 CABG. Incomplete ICA constitutes rare, but a significant clinical problem. Coronary CTA provides adequate clinical information in these patients.






Similar content being viewed by others
References
Ropers D, Pohle FK, Kuettner A, Pflederer T, Anders K, Daniel WG, Bautz W, Baum U, Achenbach S (2006) Diagnostic accuracy of noninvasive coronary angiography in patients after bypass surgery using 64-slice spiral computed tomography with 330-ms gantry rotation. Circulation 114(22):2334–2341
Pache G, Saueressig U, Frydrychowicz A, Foell D, Ghanem N, Kotter E, Geibel-Zehender A, Bode C, Langer M, Bley T (2006) Initial experience with 64-slice cardiac CT: non-invasive visualization of coronary artery bypass grafts. Eur Heart J 27(8):976–980
Nieman K, Pattynama PM, Rensing BJ, Van Geuns RJ, De Feyter PJ (2003) Evaluation of patients after coronary artery by-pass surgery: CT angiographic assessment of grafts and coronary arteries. Radiology 229:749–756
Schroeder S, Achenbach S, Bengel F, Burgstahler C, Cademartiri F, de Feyter P, George R, Kaufmann P, Kopp AF, Knuuti J, Ropers D, Schuijf J, Tops LF, Bax JJ (2008) Cardiac computed tomography: indications, applications, limitations, and training requirements: report of a Writing Group deployed by the Working Group Nuclear Cardiology and Cardiac CT of the European Society of Cardiology and the European Council of Nuclear Cardiology. Eur Heart J 29(4):531–556
Burgstahler C, Beck T, Kuettner A, Drosch T, Kopp AF, Heuschmid M, Claussen CD, Schroeder S (2006) Non-invasive evaluation of coronary artery bypass grafts using 16-row multi-slice computed tomography with 188 ms temporal resolution. Int J Cardiol 106:244–249
Hecht HS, Jelnin V, Roubin GS (2008) Indications for multidetector computed tomographic coronary angiography after catheter-based coronary angiography. J Invasive Cardiol. 20:1–6
Taylor AJ, Cerqueira M, Hodgson JM, Mark D, Min J, O’Gara P, Rubin GD (2010) ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. J Am Coll Cardiol 56(22):1864–1894
Boyle AJ, Chan M, Dib J, Resar J (2006) Catheter-induced coronary artery dissection: risk factors, prevention and management. J Invasive Cardiol. 10:500–503
Karalis DG, Quinn V, Victor MF, Ross JJ, Polansky M, Spratt KA, Chandrasekaran K (1996) Risk of catheter-related emboli in patients with atherosclerotic debris in the thoracic aorta. Am Heart J 131(6):1149–1155
Eggebrecht H, Oldenburg O, Dirsch O, Haude M, Baumgart D, Welge D, Herrmann J, Arnold G, Schmid KW, Erbel R (2000) Potential embolization by atherosclerotic debris dislodged from aortic wall during cardiac catheterization: histological and clinical findings in 7,621 patients. Catheter Cardiovasc Interv 49(4):389–394
Pouleur AC, de Waroux JB, Kefer J, Pasquet A, Coche E, Vanoverschelde JL, Gerber BL (2007) Usefulness of 40-slice multidetector row computed tomography to detect coronary disease in patients prior to cardiac valve surgery. Eur Radiol 17(12):3199–3207
Galas A, Hryniewiecki T, Kępka C, Michałowska I, Abramczuk E, Orłowska Baranowska E, Demkow M, Rużyłło W (2012) May dual-source computed tomography angiography replace invasive coronary angiography in the evaluation of patients referred for valvular disease surgery? Kardiol Pol. 70(9):877–882
Conflict of interest
There are no conflicts of interest related to this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pregowski, J., Kepka, C., Kruk, M. et al. The clinical significance and management of patients with incomplete coronary angiography and the value of additional computed tomography coronary angiography. Int J Cardiovasc Imaging 30, 825–832 (2014). https://doi.org/10.1007/s10554-014-0397-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-014-0397-9