
Abstract
Aims
To assess the existence, components and clinical relevance of cardiac causes of death and cardiovascular (CV) hospitalizations in a population-wide database of patients with breast cancer (BC).
Methods and results
A population-wide database of the Puglia Region, Italy was analyzed, with a prospective comparative design. Three successive closely matched case/control cohorts representing current care in the period 2007–2014 were also stratified according to age to focus specifically on the potential interaction of treatment-related cardiac toxicity and the expected different baseline CV risk profiles.
Results
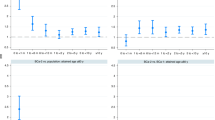
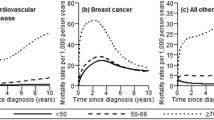
At 3-year follow-up, in the successive cohorts the incidence of BC-related (7.7, 7.0, 6.5%) and cardiac causes of death, specifically attributed to heart failure (HF, 1.3, 0.5, 0.5%), decreased. Significant mortality hazard ratio (HR) for HF was found in the total population (1.47, 95% CI 1.14–1.90), in particular in the 2007–2009 cohort (1.71, 95% CI 1.19–2.46) and in the 50–69 age group (7.96, 95% CI 2.81–22.55). Results at 5 years confirm the mortality findings, and a significant HR for hospitalizations for HF, non-atrial arrhythmias and ischemic heart disease in the younger than 50 subpopulation pointed to a late expression of toxicity in the youngest BC population.
Conclusions
The incidence of CV causes of death 3 and 5 years after BC diagnosis was very low, even if an excess in risk of death for HF as compared with the control cohort was observed. While younger patients seems to tolerate BC and BC therapy better in the short term, HF mortality and morbidity resulted significantly increased at 5-year follow-up. As the risk for hospitalization for CV reasons increased at 5-year follow-up in particular in women aged less than 50 years, CV monitoring in this subgroup of patients seems mandatory.
Similar content being viewed by others

References
Lenihan DJ, Hartlage G, DeCara J et al (2016) Cardio-oncology training: a proposal from the International Cardiooncology Society and Canadian Cardiac Oncology Network for a new multidisciplinary specialty. J Card Fail 22:465–471
Zamorano JL, Lancellotti P, Rodriguez Muñoz D et al (2017) 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: the Task Force for Cancer Treatments and Cardiovascular Toxicity of the European Society of Cardiology (ESC). Eur J Heart Fail 19:9–42
Armenian SH, Lacchetti C, Barac A et al (2017) Prevention and monitoring of cardiac dysfunction in survivors of adult cancers: American Society of Clinical Oncology clinical practice guideline. J Clin Oncol Off J Am Soc Clin Oncol 35:893–911
Mehta LS, Watson KE, Barac A et al (2018) Cardiovascular disease and breast cancer: where these entities intersect: a scientific statement from the American Heart Association. Circulation 137:e30–e66
Levis BE, Binkley PF, Shapiro CL (2017) Cardiotoxic effects of anthracycline-based therapy: what is the evidence and what are the potential harms? Lancet Oncol 18:e445–e456
Gernaat SAM, Ho PJ, Rijnberg N et al (2017) Risk of death from cardiovascular disease following breast cancer: a systematic review. Breast Cancer Res Treat 164:537–555
Cardinale D, Ciceri F, Latini R et al (1990) Anthracycline-induced cardiotoxicity: a multicenter randomised trial comparing two strategies for guiding prevention with enalapril: the International Cardio-oncology Society-one trial. Eur J Cancer Oxf Engl 2018(94):126–137
Bosch X, Rovira M, Sitges M et al (2013) Enalapril and carvedilol for preventing chemotherapy-induced left ventricular systolic dysfunction in patients with malignant hemopathies: the OVERCOME trial (preventiOn of left Ventricular dysfunction with Enalapril and caRvedilol in patients submitted to intensive ChemOtherapy for the treatment of Malignant hEmopathies). J Am Coll Cardiol 61:2355–2362
Gulati G, Heck SL, Ree AH et al (2016) Prevention of cardiac dysfunction during adjuvant breast cancer therapy (PRADA): a 2 × 2 factorial, randomized, placebo-controlled, double-blind clinical trial of candesartan and metoprolol. Eur Heart J 37:1671–1680
Banke A, Fosbøl EL, Møller JE et al (2018) Long-term effect of epirubicin on incidence of heart failure in women with breast cancer: insight from a randomized clinical trial. Eur J Heart Fail 20:1447–1453
Gulati G, Heck SL, Røsjø H et al (2017) Neurohormonal blockade and circulating cardiovascular biomarkers during anthracycline therapy in breast cancer patients: results from the PRADA (Prevention of Cardiac Dysfunction During Adjuvant Breast Cancer Therapy) Study. J Am Heart Assoc. https://doi.org/10.1161/JAHA.117.006513
Meessen JMTA, Cardinale D, Ciceri F et al (2020) Circulating biomarkers and cardiac function over 3 years after chemotherapy with anthracyclines: the ICOS-ONE trial. ESC Heart Fail. https://doi.org/10.1002/ehf2.12695(published online May 1)
Macchia A, Romero M, D’Ettorre A, Mariani J, Tognoni G (2012) Temporal trends of the gaps in post-myocardial infarction secondary prevention strategies of co-morbid and elderly populations vs. younger counterparts: an analysis of three successive cohorts between 2003 and 2008. Eur Heart J 33:515–522
De Berardis G, Lucisano G, D’Ettorre A et al (2012) Association of aspirin use with major bleeding in patients with and without diabetes. JAMA 307:2286–2294
Cosmi F, Shen L, Magnoli M et al (2018) Treatment with insulin is associated with worse outcome in patients with chronic heart failure and diabetes. Eur J Heart Fail 20:888–895
Robusto F, Lepore V, D’Ettorre A et al (2016) The drug derived complexity index (DDCI) predicts mortality, unplanned hospitalization and hospital readmissions at the population level. PLoS ONE 11:e0149203
Bradshaw PT, Stevens J, Khankari N, Teitelbaum SL, Neugut AI, Gammon MD (2016) Cardiovascular disease mortality among breast cancer survivors. Epidemiology (Camb Mass) 27:6–13
Abdel-Qadir H, Austin PC, Lee DS et al (2017) A population-based study of cardiovascular mortality following early-stage breast cancer. JAMA Cardiol 2:88–93
Gernaat SAM, Boer JMA, van den Bongard DHJ et al (2018) The risk of cardiovascular disease following breast cancer by Framingham risk score. Breast Cancer Res Treat 170:119–127
Thavendiranathan P, Abdel-Qadir H, Fischer HD et al (2016) Breast cancer therapy-related cardiac dysfunction in adult women treated in routine clinical practice: a population-based cohort study. J Clin Oncol Off J Am Soc Clin Oncol 34:2239–2246
Boekel NB, Jacobse JN, Schaapveld M et al (2018) Cardiovascular disease incidence after internal mammary chain irradiation and anthracycline-based chemotherapy for breast cancer. Br J Cancer 119:408–418
Dasgupta P, Aitken JF, Pyke C, Baade PD (2018) Competing mortality risks among women aged 50–79 years when diagnosed with invasive breast cancer, Queensland, 1997–2012. Breast (Edinb Scotl) 41:113–119
Campia U, Moslehi JJ, Amiri-Kordestani L et al (2019) Cardio-oncology: vascular and metabolic perspectives: a scientific statement from the American Heart Association. Circulation 139:e579–e602
Hershman DL, Till C, Shen S et al (2018) Association of cardiovascular risk factors with cardiac events and survival outcomes among patients with breast cancer enrolled in SWOG Clinical Trials. J Clin Oncol Off J Am Soc Clin Oncol 36:2710–2717
Sturgeon KM, Deng L, Bluethmann SM et al (2019) A population-based study of cardiovascular disease mortality risk in US cancer patients. Eur Heart J 40:3889–3897
Boekel NB, Schaapveld M, Gietema JA et al (2016) Cardiovascular disease risk in a large, population-based cohort of breast cancer survivors. Int J Radiat Oncol Biol Phys 94:1061–1072
Colzani E, Liljegren A, Johansson ALV et al (2011) Prognosis of patients with breast cancer: causes of death and effects of time since diagnosis, age, and tumor characteristics. J Clin Oncol Off J Am Soc Clin Oncol 29:4014–4021
Pinder MC, Duan Z, Goodwin JS, Hortobagyi GN, Giordano SH (2007) Congestive heart failure in older women treated with adjuvant anthracycline chemotherapy for breast cancer. J Clin Oncol Off J Am Soc Clin Oncol 25:3808–3815
Weberpals J, Jansen L, Müller OJ, Brenner H (2018) Long-term heart-specific mortality among 347,476 breast cancer patients treated with radiotherapy or chemotherapy: a registry-based cohort study. Eur Heart J 39:3896–3903
Strongman H, Gadd S, Matthews A et al (2019) Medium and long-term risks of specific cardiovascular diseases in survivors of 20 adult cancers: a population-based cohort study using multiple linked UK electronic health records databases. Lancet (Lond Engl) 394:1041–1054
Cancer statistics—specific cancers—statistics explained. https://ec.europa.eu/eurostat/statistics-explained/index.php/Cancer_statistics-specific_cancers#Breast_cancer.%2520Accessed%2520September%252030,%25202019. Accessed 25 Sep 2019
Redelings MD, Sorvillo F, Simon P (2006) A comparison of underlying cause and multiple causes of death: US vital statistics, 2000–2001. Epidemiology (Camb Mass) 17:100–103
Piffaretti C, Moreno-Betancur M, Lamarche-Vadel A, Rey G (2016) Quantifying cause-related mortality by weighting multiple causes of death. Bull World Health Organ 94:870–879
Acknowledgements
We are grateful to Jennifer Meessen for her statistical assistance and Judith Baggott for language editing. This study is part of the work covered by the 2015–2020 Collaboration between the Regional Healthcare Agency of Puglia Region (AReS Puglia), Italy and the Istituto di Ricerche Farmacologiche Mario Negri IRCCS.
Author information
Authors and Affiliations
Contributions
LS, FR, GT, RL and VL contributed to the conception and design of the study and data interpretation; LS contributed to the literature search, AD, LB and BP to the data extraction; FR contributed to data analysis; GT and RL conducted the quality assessment. All authors contributed to writing the manuscript, and all authors approved the manuscript. FR, LS, VL, RL and GT guarantees the integrity of the work. The authors had full access to all the data in the study and the final responsibility for the decision to submit for publication. The corresponding author attests that all listed authors meet authorship criteria.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Research involving human participants and/or animals
This article does not contain any study involving humans or animals.
Ethical approval
In this study, we use aggregated anonymous data. Data anonymization prior to any analysis and data protection procedures followed the strict criteria adopted by the Puglia Region Health Care Agency, in full compliance with national regulations, and the ethical requirements foreseen for the epidemiological utilization of administrative databases (https://eurlex.europa.eu/eli/reg/2016/679/oj; DL August 10, 2018 No. 101; Act of Department of Health of the Puglia Region (No. 16; May 4, 2015). The use of data in this project does not require review by a Research Ethics Board.
Informed consent
According to the Italian Personal Data Protection Code (LD 30 June 2003, No. 196 and Appendix), no informed consent from patients is required when using anonymous aggregated data.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Staszewsky, L., Robusto, F., Lepore, V. et al. Cardiovascular mortality and morbidity burden in successive and age pre-stratified case–control cohorts of breast cancer women. A population-based study. Breast Cancer Res Treat 183, 177–188 (2020). https://doi.org/10.1007/s10549-020-05758-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-020-05758-4